

Abstract
The forced oscillation technique (FOT) is a method for non-invasively assessing respiratory mechanics that is applicable both in paralysed and non-paralysed patients. As the FOT requires a minimal modification of the conventional ventilation setting and does not interfere with the ventilation protocol, the technique is potentially useful to monitor patient mechanics during invasive and noninvasive ventilation. FOT allows the assessment of the respiratory system linearity by measuring resistance and reactance at different lung volumes or end-expiratory pressures. Moreover, FOT allows the physician to track the changes in patient mechanics along the ventilation cycle. Applying FOT at different frequencies may allow the physician to interpret patient mechanics in terms of models with pathophysiological interest. The current methodological and technical experience make possible the implementation of portable and compact computerised FOT systems specifically addressed to its application in the mechanical ventilation setting.
Keywords: forced oscillation technique, monitoring, respiratory impedance, respiratory resistance, airway mechanics
Introduction
The mechanical properties of the respiratory system in paralysed and mechanically ventilated patients are commonly measured by means of occlusion techniques [1] or by multilinear regression analysis [2]. Respiratory resistance and elastance are computed from pressure and flow recorded at the airway opening under the assumption that the contribution of the patient's respiratory muscles is nil, so that airway pressure coincides with transpulmonary pressure. Although these measurements can readily be performed on paralysed patients, their application during assisted ventilation in patients with active inspiratory muscles is not possible. The only conventional procedure for assessing respiratory mechanics when the patient's respiratory muscles are active is to employ an oesophageal balloon catheter. However, the use of an oesophageal balloon is not practicable in applications during mechanical ventilation such as noninvasive ventilation or weaning.
FOT is a method for noninvasively assessing respiratory mechanics during mechanical ventilation [3] and is applicable both in paralysed [4,5,6,7] and nonparalysed patients [8,9,10]. FOT is based on the application of a small pressure oscillation (about 2 cmH2O) at the airway opening by means of an external generator, and on recording the oscillation pressure and flow [11]. When employed in non-paralysed patients, forced oscillation is applied at a frequency (more than 2 Hz) that is much higher than the patient's breathing rate. At such high frequencies the activity of the muscle pump, which operates at the breathing frequency and its first harmonics, is negligible. Under this assumption the only driving pressure at the forced oscillation frequency is the pressure applied at the mouth by the external generator. Consequently, FOT applied at a sufficiently high frequency allows the noninvasive assessment of respiratory mechanics in patients with artificial respiratory support regardless of the degree of activity of their respiratory muscles.
Oscillatory resistance and reactance
Assessment of respiratory mechanics by the application of FOT requires a minimal modification of the conventional ventilation setting. As shown in Fig. 1, a forced oscillation generator is connected in parallel with the ventilator. Flow is recorded by a pneumotachograph placed at the inlet of the endotracheal tube and a differential pressure transducer. Pressure is recorded by a pressure transducer placed at the airway opening. When FOT is applied in nonintubated patients with ventilatory support, the endotracheal tube is replaced by a nasal or face mask. With the setting shown in Fig. 1, the forced oscillation pressure can be superimposed on the ventilator pressure waveform without modifying or interfering with the ventilation protocol. Figure 2 shows an example of the pressure and flow signals recorded during a FOT measurement at a frequency of 5 Hz during noninvasive mechanical ventilation.
Figure 1.
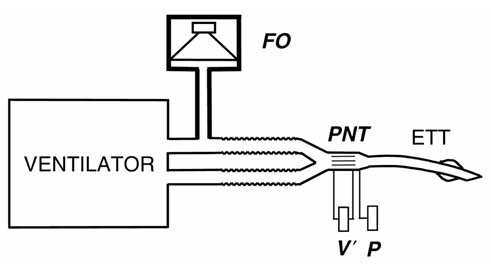
Diagram of the setting to apply the forced oscillation technique during mechanical ventilation. A forced oscillation generator (OF) is connected in parallel to the ventilator. Flow (V') and pressure (P) are measured by means of a pneumotachograph (PNT) and a pressure transducer, respectively.
Figure 2.
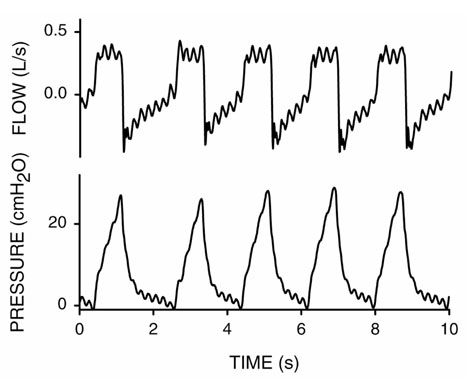
Example of the pressure and flow signals recorded during application of a 5 Hz forced oscillation during volume-controlled noninvasive mechanical ventilation in a patient with a chest wall restrictive defect. The 5 Hz forced oscillation technique component is superimposed on the pressure and flow ventilator waveforms.
To assess oscillatory mechanics by FOT, the recorded signals (Fig. 2) are filtered to isolate the 5 Hz oscillatory signals from the low-frequency breathing components. The patient's mechanics is characterised by means of his/her respiratory impedance, which quantifies the relationship between oscillatory pressure and flow. As explained elsewhere [11], respiratory impedance is a complex quantity represented by two components: respiratory resistance (Rrs) and reactance (Xrs). Rrs is define as the quotient between the oscillatory pressure component in phase with flow and the oscillatory flow amplitude. Similarly, Xrs is computed from the oscillatory pressure component out of phase with oscillatory flow and the oscillatory flow amplitude [11].
Rrs and Xrs measured by FOT can be interpreted by means of mechanistic models of the respiratory system mechanics. For instance, the respiratory system can be modelled by a simple resistance (R), an inertance (I) and an elastance (E), in an R-I-E model. According to the definition of Rrs and of Xrs, it follows [11] that for a given oscillation frequency (f) the oscillatory resistance coincides with the resistance value of the simple R-I-E model (Rrs = R). Moreover, the reactance of the R-I-E model is Xrs = 2πfI – E/(2πf). Therefore, when applied to a homogeneous R-I-E model, FOT results in a Rrs value that is independent of frequency, whereas Xrs depends on frequency and accounts for the elastic (E) and inertial (I) properties. Accordingly, measuring Rrs and Xrs at different frequencies and fitting the R-I-E model to the data make it possible to derive the values of the parameters R, I and E that characterise the mechanical properties of the patient's respiratory system. The pattern of frequency dependence of Rrs and Xrs described by the R-I-E homogeneous model is observed in healthy subjects [11]. Nevertheless, when FOT is applied in ventilated patients this simple model is no longer applicable owing to the complexity of the patient's respiratory system [5,6,7]. For this application, respiratory impedance data should be interpreted in terms of models that take into consideration the different mechanisms that determine the behaviour of the respiratory system at the oscillatory frequencies investigated [7,12,13]. In particular, modelling should include coefficients that account for the expected serial and/or parallel inhomogeneities [5] and the viscoelasticity of respiratory tissues [14]. In this regard, FOT has the advantage that the frequency band explored can be modified depending on the pathophysiological aim of the measurement. For instance, if interest is focused on studying respiratory tissue properties, low-frequency (less than 2 Hz) impedance data would be more sensitive [7]. By contrast, measurements at higher frequency would afford more sensitive data on airway characteristics [5]. A frequency of 5 Hz or higher should be used when applying a simple sinusoidal oscillation (Fig. 1) for monitoring respiratory mechanics along the ventilation cycle [5,15,16].
Equipment
The basic FOT set-up shown in Fig. 1 can be implemented by means of different technical approaches. The main practical issues are the type of oscillation generator, the procedure for measuring pressure and flow, and the type of oscillatory signal employed to measure Rrs and Xrs.
As shown in Fig. 1, the forced oscillation generator should be able to withstand the high positive ventilator pressure during inspiration and should be able to generate the forced oscillation pressure [17]. In the absence of a FOT generator specially designed to withstand high positive pressures, the technique was employed by disconnecting the patient from the ventilator for a few seconds and applying pressure oscillation with a loudspeaker attached to the inlet of the endotracheal tube [4]. Another method for applying FOT in ventilated patients with a simple loudspeaker-in-box system is to connect it to the expiratory outlet of the ventilator [18]. During the inspiratory phase the expiratory valve of the ventilator is occluded with the result that the loudspeaker is not subjected to the high pressures applied to the patient. During the expiratory phase the valve is opened and the pressure oscillation generated by the loudspeaker is transmitted to the patient through the expiratory tubing. This simple method, which can be applied to both paralysed and nonparalysed patients, allows measurements only during expiration. The application of FOT during all the ventilation cycle and for any external positive end-expiratory pressure (PEEP) applied is currently possible by means of two procedures. One of the generators employed [5] consists of a loudspeaker-in-box system including a pneumatic filter that allows the device to withstand positive pressures. This procedure has the advantage of being very simple but its main drawback is that forced oscillation can be applied only for frequencies greater than 5 Hz, which excludes the physiological frequency band close to the breathing rate. To overcome this limitation, a more complex FOT generator based on a servocontrolled loudspeaker-in-box system has been described [19]. This allows the extension of forced oscillation measurements to frequencies close to the breathing rate (0.25 Hz). It is of interest to note that future technical developments could enable the ventilator to generate the oscillation signal superimposed on the ventilation waveform [10,20], which would considerably simplify the routine application of FOT.
An important issue in the assessment of respiratory mechanics by FOT in ventilated patients is the measurement of flow and pressure. For practical reasons the pressure transducers are placed at a certain distance from the inlet of the endotracheal tube. Consequently, the effects of the tubes connecting the transducers to the pneumotachograph, and the pneumotachograph to the airway opening, on the frequency response of the sensors [21] should be taken into consideration and corrected [22]. Although flow measurement is readily performed by a pneumotachograph, a good common-mode rejection ratio in the differential pressure transducer connected to the pneumotachograph should be ensured [23] or data should be corrected [24]. This requirement, which is general in FOT measurements, is particularly relevant in this application given that the impedance values characterising ventilated patients are high. Increasing the resistance of the pneumotachograph, which could reduce potential artefacts [23,24], is not practicable because this would promote auto-PEEP. Pressure measurement in ventilated patients is influenced by the nonlinear pressure-flow relationship in the endotracheal tube. The most direct way of rounding off the artefacts caused by tube nonlinearities is to measure pressure at the tracheal level instead of at the endotracheal tube inlet. This procedure can be performed by using a special tube incorporating a catheter [25] or by introducing a catheter into the trachea through the endotracheal tube. In both cases, the tube nonlinearity does not affect the measurements because the recorded pressure does not include the pressure drop across the tube. These two procedures for directly recording tracheal pressure suffer from the practical drawback that they require the use of a special endotracheal tube or the introduction of an extra catheter, respectively. For routine purposes, it is more practical to measure pressure at the inlet of the endotracheal tube and to correct for its nonlinear effects in the measured impedance [5].
Assessment of the frequency dependence of Rrs and Xrs provides information for a better characterisation of the patient's respiratory mechanics. Determining Rrs and Xrs at several frequencies with sinusoidal oscillation (Fig. 2) would require several measurements at the different frequencies of interest, which would not be practicable in routine. Alternatively, it is possible to characterise respiratory mechanics in greater detail by measuring Rrs and Xrs at different frequencies simultaneously in a single measurement. For this purpose, a complex signal containing several frequencies is employed instead of a sinusoidal oscillation [11]. The multifrequency signal might consist of a random noise, of a fundamental frequency plus its harmonics (for example 2, 4, 6, 8 Hz) or of a more complex combination of optimised frequencies, which is particularly useful in the case of marked nonlinearities in the respiratory system [26]. The analysis of the complex multifrequency signals recorded and the computation of Rrs and Xrs at the different frequencies are performed automatically by means of a computer. Conventional data processing also provides an index of impedance reliability [27].
Application of FOT in ventilated patients
The basic approach to the assessment of respiratory mechanics by FOT is the application of a sinusoidal oscillation (Fig. 2). This procedure is particularly suitable for computing an index of respiratory impedance to monitor the changes in the patient's respiratory mechanics within the ventilation cycle during invasive and noninvasive ventilation [5,8]. Moreover, sinusoidal oscillation is also useful for assessing patient mechanics during noninvasive ventilation with continuous positive airway pressure, pressure support, volume control or proportional assist ventilation [8,9,10,28]. Given its simplicity, sinusoidal oscillation is a potential tool for routinely determining the response to different pharmacological treatments or interventions during mechanical ventilation (such as postural change [28], aspiration, application of PEEP [19,28], weaning).
Extending the frequency band of FOT measurements down to low frequencies (about 0.25 Hz) allows the assessment of Rrs and Xrs over a wide band, including frequencies close to breathing rates. The advantage of such a measurement is that it enables us to compare Rrs and Xrs measured by FOT with the results obtained by more conventional techniques in respiratory mechanics (such as airway occlusions or multilinear regression analysis) [6,7]. Using low frequencies (that is, long periods) to assess respiratory mechanics at a given lung volume requires the patient to be paralysed and the measurements to be performed during inspiratory (Fig. 3) or expiratory (Fig. 4) pauses so as to keep the respiratory system at a fixed operating point (in terms of volume or transpulmonary pressure) during a measurement lasting several seconds. A short pause is readily achieved by pushing the corresponding ventilator control buttons with minimum disturbance of the ventilation pattern.
Figure 3.
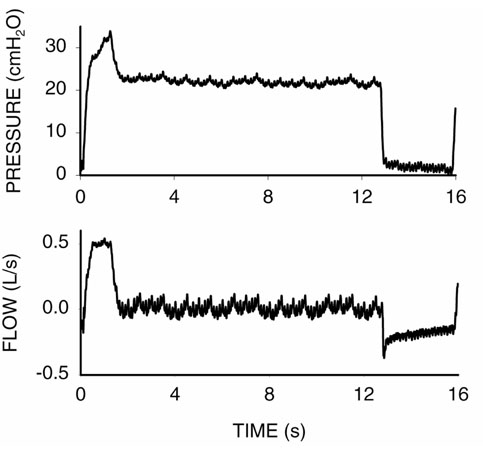
Pressure and flow signals recorded in a forced oscillation technique measurement (0.25-16 Hz) during an inspiratory pause in a paralysed and mechanically ventilated patient with chronic obstructive pulmonary disease.
Figure 4.
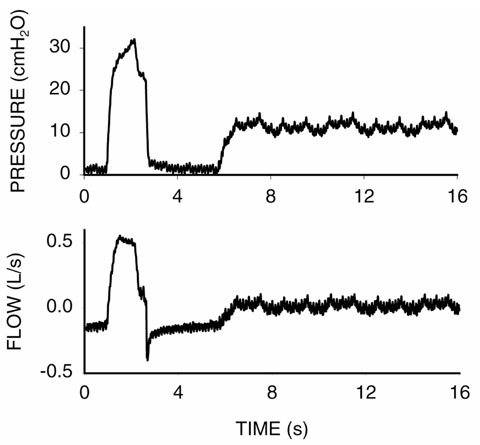
Pressure and flow signals recorded in a forced oscillation technique measurement (0.25-16 Hz) during an expiratory pause in a paralysed and mechanically ventilated patient with chronic obstructive pulmonary disease.
One advantage of measuring Rrs and Xrs during inspiratory and expiratory pauses in a given patient is to quantify the dependence of respiratory mechanics on lung volume or transpulmonary pressure. Indeed, as shown in Fig. 5, Rrs and Xrs computed from the measurements in Figs 3 and 4 show that in this patient with chronic obstructive pulmonary disease (COPD), impedance was considerably greater during expiratory than inspiratory pauses, particularly at the lower frequencies. Rrs during the expiratory pause was considerably dependent on frequency over the whole frequency band. By contrast, Rrs during the inspiratory pause was much less dependent on frequency (Fig. 5). Xrs also was also different during inspiratory and expiratory pauses, particularly at more than 1 Hz. This pattern of frequency dependence has been interpreted in terms of increased peripheral resistance due to airway closure at end-expiration [5,7]. This interpretation is in keeping with the observations in Fig. 6, namely that Rrs at end-expiration progressively and considerably decreased as transpulmonary pressure (PEEP) increased. The values of Rrs and Xrs provided by FOT can be compared with the resistance and elastance indices derived from the application of the airway occlusion technique, which has been used extensively to assess airway mechanics in ventilated patients [6,7]. Indeed, FOT data are obtained from small-amplitude oscillations at the extreme points of a conventional inflation (end-expiration and end-inspiration), whereas data from the occlusion manoeuvres are obtained from a high-amplitude excursion across those extreme points. Such a comparison sheds some light on the mechanisms determining the nonlinear properties of the respiratory system in patients and might be useful for predicting the relationship between pressure, flow and volume during mechanical ventilation.
Figure 5.
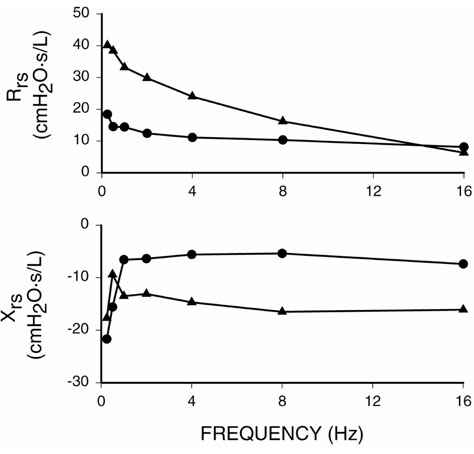
Respiratory resistance (Rrs) and reactance (Xrs) during inspiratory (●) and expiratory (▲) pauses (Figs 3 and 4) in a paralysed and mechanically ventilated patient with chronic obstructive pulmonary disease.
Figure 6.
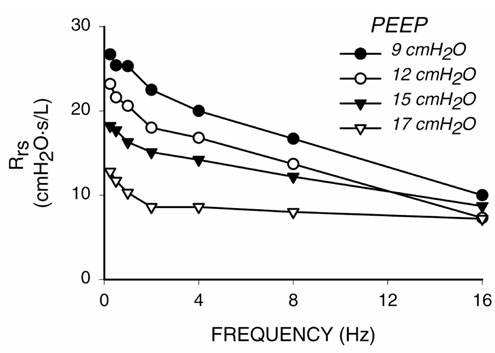
Respiratory resistance (Rrs) measured during expiratory pauses at different positive end-expiratory pressure levels in a paralysed and mechanically ventilated patient with chronic obstructive pulmonary disease.
The interpretation of Rrs and Xrs measured under nonlinear conditions (Figs 5 and 6) is difficult. However, the results obtained in analogue models, in animals and in patients suggest that FOT is useful for characterising the viscoelas-tic properties of respiratory tissues [7], for assessing inhomogeneities in the respiratory system [5,6,7] and for detecting expiratory flow limitation during mechanical ventilation [16,29]. The interpretation of measured Rrs and Xrs can be performed in terms of models with a pathophysiological interest. For instance, a simple model proposed to analyse Rrs and Xrs in mechanically ventilated COPD patients consists of a central airway resistance plus a shunt elastance due to the bronchial wall, in parallel with peripheral airway resistance and tissue elastance [7]. As shown in Fig. 7, this simple model can mimic the pattern of frequency dependence of Rrs and Xrs during end-inspiratory and end-expiratory pauses (Fig. 5) by means of an increase in the peripheral resistance due to airway closure during expiration. Figure 7 shows that, in inhomogeneous models, a change in airway properties, for example an increase in peripheral resistance, modifies both Rrs and Xrs. Nevertheless, it should be stressed that so far there is no solid evidence in favour of using a specific model to interpret FOT data in mechanically ventilated patients. Consequently, the values of Rrs and Xrs measured at certain frequencies are probably the best indices for monitoring the mechanical status and evolution of the ventilated patient in clinical practice.
Figure 7.
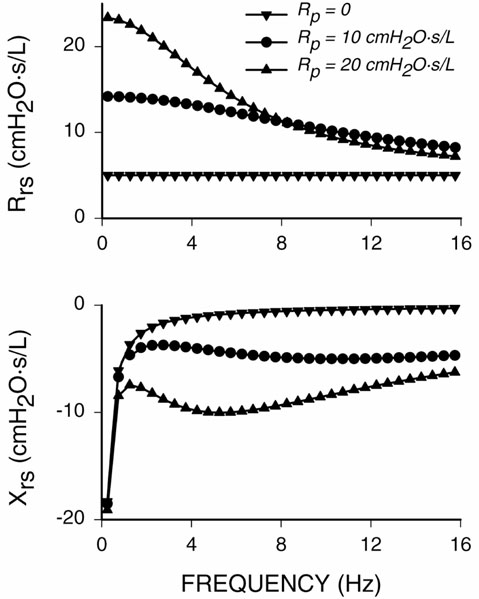
Respiratory resistance (Rrs) and reactance (Xrs) in a model [7] consisting of a central airway resistance of 5 cmH2O s L-1 plus a bronchial wall elastance of 700 cmH2O L-1 in parallel with a peripheral airway resistance (Rp) and a tissue elastance of 30 cmH2O L-1. Rrs and Xrs are shown for three different values of Rp.
Conclusion
FOT is useful for characterising the respiratory mechanics in patients subjected to noninvasive or invasive mechanical ventilation. The main advantage of this technique is that it is readily and continuously applicable during mechanical ventilation, obviating the need for disturbing or modifying the ventilation pattern. Moreover, it allows automatic and on-line monitoring of Rrs and Xrs to assess the dependence of the patient's respiratory mechanics on pressure, flow and volume as well as to detect expiratory flow limitation. Continuous FOT monitoring of the status and evolution of the ventilated patient provides updated information that is potentially useful for resetting the ventilator. Although at present the application of FOT in ventilated patients has been mainly confined to research, current methodological and technical experience enables the application of portable and compact computerised FOT systems during mechanical ventilation [30,31].
Acknowledgments
Acknowledgement
This work was supported in part by Comisión Interministerial de Ciencia y Tecnología (CICYT, SAF99-0001) and Dirección General de Enseñanza Superior e Investigación Científica (DGESIC, PM98-0027).
References
- Eissa NT, Ranieri VM, Corbeil C, Chasse M, Robatto FM, Braidy J, Milic-Emili J. Analysis of behavior of the respiratory system in ARDS patients: effect of flow, volume, and time. J Appl Physiol. 1991;70:2719–2729. doi: 10.1152/jappl.1991.70.6.2719. [DOI] [PubMed] [Google Scholar]
- Peslin R, Felicio-da-Silva J, Chabot F, Duvivier C. Respiratory mechanics studied by multiple linear regression in unsedated ventilated patients. Eur Respir J. 1992;5:871–878. [PubMed] [Google Scholar]
- Van de Woestijne K. The forced oscillation technique in intubated, mechanically-ventilated patients [editorial]. Eur Respir J. 1993;6:767–769. [PubMed] [Google Scholar]
- Navajas D, Farré R, Canet J, Rotger M, Sanchis J. Respiratory input impedance in anestethized paralyzed patients. J Appl Physiol. 1990;69:1372–1379. doi: 10.1152/jappl.1990.69.4.1372. [DOI] [PubMed] [Google Scholar]
- Peslin R, Felicio-da SJ, Duvivier C, Chabot F. Respiratory mechanics studied by forced oscillations during artificial ventilation. Eur Respir J. 1993;6:772–784. [PubMed] [Google Scholar]
- Beydon L, Malassiné P, Lorino AM, Mariette C, Bonnet F, Harf A, Lorino H. Respiratory resistance by end-inspiratory occlusion and forced oscillations in intubated patients. J Appl Physiol. 1996;80:1105–1111. doi: 10.1152/jappl.1996.80.4.1105. [DOI] [PubMed] [Google Scholar]
- Farré R, Ferrer M, Rotger M, Torres A, Navajas D. Respiratory mechanics in ventilated COPD patients: forced oscillation versus occlusion techniques. Eur Respir J. 1998;12:170–176. doi: 10.1183/09031936.98.12010170. [DOI] [PubMed] [Google Scholar]
- Navajas D, Farré R, Rotger M, Puig-de-Morales M, Montserrat JM. Assessment of airflow obstruction during CPAP by means of forced oscillation in patients with sleep apnea. Am J Respir Crit Care Med. 1998;157:1526–1530. doi: 10.1164/ajrccm.157.5.9710026. [DOI] [PubMed] [Google Scholar]
- Ferrer M, Iglesia R, Roca J, Escarrabill J, Farrero E, Gomez FP, Farré R, Barbera JA, Rodriguez-Roisin R. Factors determining arterial respiratory blood gases during noninvasive ventilation in clinically stable chronic respiratory failure. Eur Respir J. 1998;12(suppl 28):52s. [Google Scholar]
- Navajas D, Gavela E, Mancini M, Rotger M, Roca J, Farré R. Respiratory resistance assessed by forced oscillation during proportional assist ventilation in COPD patients. Eur Respir J. 1999;14(suppl 30):394s. [Google Scholar]
- Navajas D, Farré R. Oscillation mechanics. In Respiratory Mechanics Edited by Milic-Emili J Sheffield: European Respiratory Society, Sheffield University [European Respiratory monographs, vol 4]; 1999. pp. 112–140.
- Lutchen KR, Greenstein JL, Suki B. How inhomogeneities and airway walls affect frequency dependence and separation of airway and tissue properties. J Appl Physiol. 1996;80:1696–1707. doi: 10.1152/jappl.1996.80.5.1696. [DOI] [PubMed] [Google Scholar]
- Lutchen KR, Gillis H. Relationship between heterogeneous changes in airway morphometry and lung resistance and elastance. J Appl Physiol. 1997;83:1192–1201. doi: 10.1152/jappl.1997.83.4.1192. [DOI] [PubMed] [Google Scholar]
- Similowski T, Bates JHT. Two-compartment modelling of respiratory system mechanics: gas redistribution or tissue rheology. Eur Respir J. 1991;4:353–358. [PubMed] [Google Scholar]
- Farré R, Peslin R, Rotger M, Barbera JA, Navajas D. Forced oscillation total respiratory resistance and spontaneous breathing lung resistance in COPD patients. Eur Respir J. 1999;14:172–178. doi: 10.1034/j.1399-3003.1999.14a29.x. [DOI] [PubMed] [Google Scholar]
- Peslin R, Farré R, Rotger M, Navajas D. Effect of expiratory flow limitation on respiratory mechanical impedance: a model study. J Appl Physiol. 1996;81:2399–2406. doi: 10.1152/jappl.1996.81.6.2399. [DOI] [PubMed] [Google Scholar]
- Farré R, Navajas D. Mechanical impedance of the forced excitation generator in respiratory impedance measurements [review]. Eur Respir Rev. 1991;1:132–138. [Google Scholar]
- Navajas D, Farré R, Rotger M, Torres A. Monitoring respiratory impedance by forced oscillation in mechanically ventilated patients [review]. Eur Respir Rev. 1994;4:216–218. [Google Scholar]
- Farré R, Ferrer M, Rotger M, Navajas D. Servocontrolled generator to measure respiratory impedance from 0.25 to 26 Hz in ventilated patients at different PEEP levels. Eur Respir J. 1995;8:1222–1227. doi: 10.1183/09031936.95.08071222. [DOI] [PubMed] [Google Scholar]
- Farré R, Rotger M, Montserrat JM, Navajas D. A system to generate simultaneous forced oscillation and continuous positive airway pressure. Eur Respir J. 1997;10:1349–1353. doi: 10.1183/09031936.97.10061349. [DOI] [PubMed] [Google Scholar]
- Farré R, Peslin R, Navajas D, Gallina C, Suki B. Analysis of the dynamic characteristics of pressure transducers for studying respiratory mechanics at high frequencies. Med Biol Eng Comput. 1989;27:531–537. doi: 10.1007/BF02441474. [DOI] [PubMed] [Google Scholar]
- Delavault E, Saumon G, Georges R. Identification of transducer defect in respiratory impedance measurements by forced random noise. Correction of experimental data. Resp Physiol. 1980;40:107–117. doi: 10.1016/0034-5687(80)90008-0. [DOI] [PubMed] [Google Scholar]
- Peslin R, Jardin P, Duvivier C, Begin P. In-phase rejection requirements for measuring respiratory input impedance. J Appl Physiol. 1984;56:804–809. doi: 10.1152/jappl.1984.56.3.804. [DOI] [PubMed] [Google Scholar]
- Farré R, Navajas D, Peslin R, Rotger M, Duvivier C. A correction procedure for the asymmetry of differential pressure transducers in respiratory impedance measurements. IEEE Trans Biomed Eng. 1989;36:1137–1140. doi: 10.1109/10.40822. [DOI] [PubMed] [Google Scholar]
- Navajas D, Farré R, Rotger M, Canet J. Recording pressure at the distal end of the endotracheal tube to measure respiratory impedance. Eur Respir J. 1989;2:178–184. [PubMed] [Google Scholar]
- Suki B, Lutchen KR. Pseudoramdon signals to estimate apparent transfer ad coherence functions of nonlinear systems: applications to respiratory mechanics. IEEE Trans Biomed Eng. 1992;39:1142–1151. doi: 10.1109/10.168693. [DOI] [PubMed] [Google Scholar]
- Van de Woestijne KP, Desager KN, Duiverman EJ, Marchal F. Recommendations for measurement of respiratory input impedance by means of the forced oscillation method. Eur Respir Rev. 1994;4:235–237. [Google Scholar]
- Farré R, Gavela E, Rotger M, Ferrer M, Roca J, Navajas D. Noninvasive assessment of respiratory resistance in severe chronic respiratory patients with nasal CPAP. Eur Respir J. 2000;15:314–319. doi: 10.1183/09031936.00.15231400. [DOI] [PubMed] [Google Scholar]
- Vassiliou M, Peslin R, Saunier C, Duvivier C. Expiratory flow limitation during mechanical ventilation detected by forced oscillation method. Eur Respir J. 1996;9:779–786. doi: 10.1183/09031936.96.09040779. [DOI] [PubMed] [Google Scholar]
- Farré R, Rotger M, Montserrat JM, Navajas D. Analog circuit for real-time computation of respiratory mechanical impedance in sleep studies. IEEE Trans Biomed Eng. 1997;44:1156–1159. doi: 10.1109/10.641343. [DOI] [PubMed] [Google Scholar]
- Rigau J, Navajas D, Montserrat JM, Farré R. Microprocessor-based system for data acquisition and processing in the forced oscillation technique. Eur Respir J. 2000;1(suppl 31):80s. [Google Scholar]