

Abstract
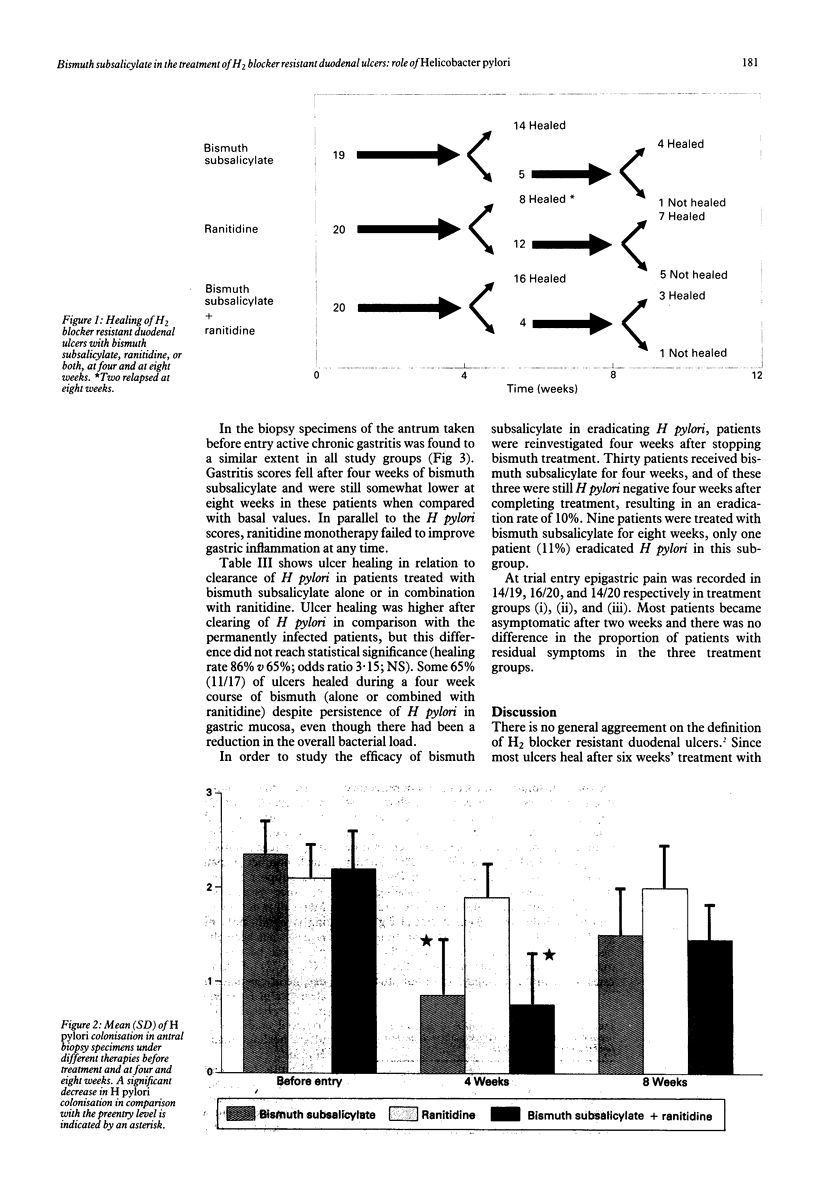
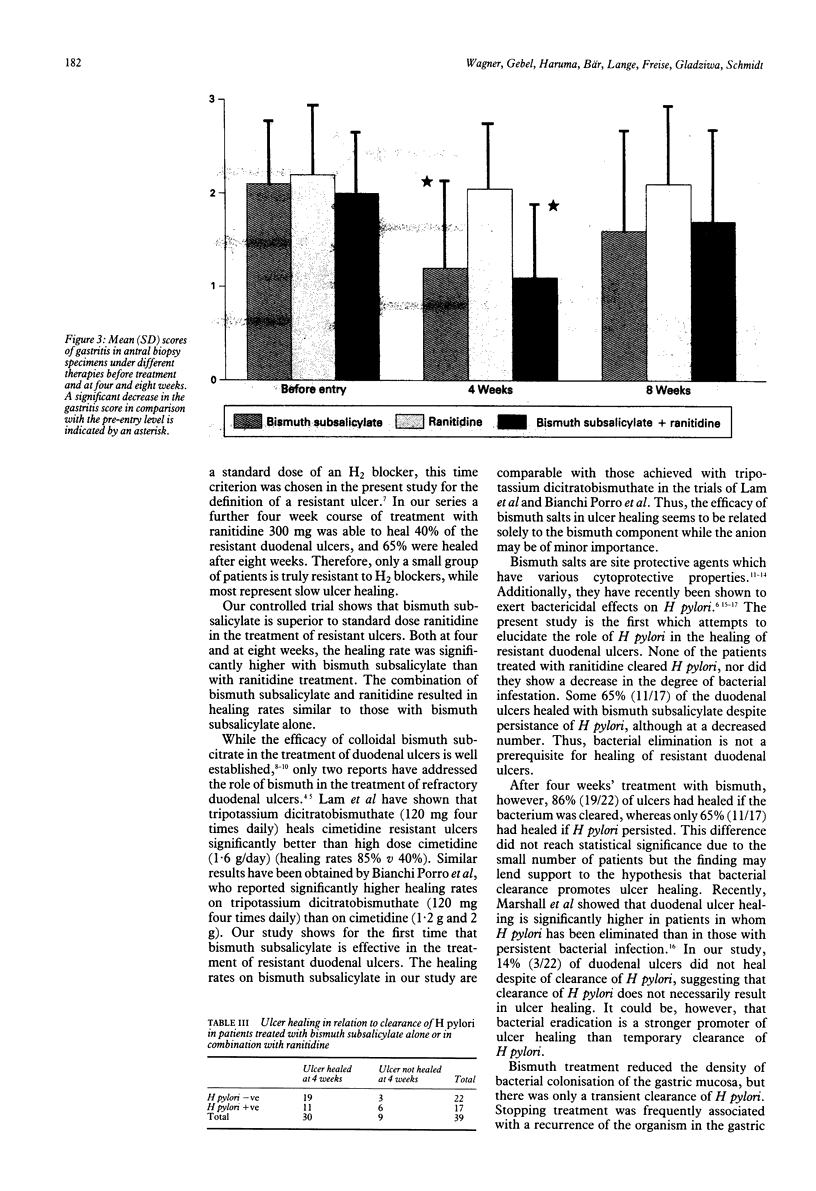
Fifty nine patients with Helicobacter pylori positive duodenal ulcers that failed to heal after a six week course of treatment with H2 blockers were randomly assigned to one of the following three regimens: (i) bismuth subsalicylate, 600 mg three times daily (n = 19), (ii) ranitidine, 300 mg at night (n = 20), (iii) bismuth subsalicylate plus ranitidine (n = 20). Cumulative ulcer healing rates after four and eight weeks respectively were as follows: bismuth subsalicylate 74% (14/19) and 95% (18/19), ranitidine 40% (8/20) and 65% (13/20), bismuth subsalicylate plus ranitidine 80% (16/20) and 95% (19/20). Bismuth subsalicylate treatment was better than ranitidine at both four and at eight weeks (p less than 0.05). The clearance rates for H pylori after four weeks were: bismuth subsubsalicylate 58%, ranitidine 0%, bismuth subsalicylate plus ranitidine 55%. After stopping bismuth therapy bacterial recrudescence frequently occurred. After bismuth treatment 86% (19/22) of ulcers had healed if H pylori had been cleared, whereas only 65% (11/17) had healed if H pylori persisted (NS). This study shows that bismuth subsalicylate is more effective in the treatment of resistant duodenal ulcers than standard dose ranitidine. It may be that suppression of H pylori by bismuth subsalicylate promotes ulcer healing.
Full text
PDF

Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Bianchi Porro G., Parente F., Lazzaroni M. Tripotassium dicitrato bismuthate (TDB) versus two different dosages of cimetidine in the treatment of resistant duodenal ulcers. Gut. 1987 Jul;28(7):907–911. doi: 10.1136/gut.28.7.907. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Brunner G., Creutzfeldt W., Harke U., Lamberts R. Therapy with omeprazole in patients with peptic ulcerations resistant to extended high-dose ranitidine treatment. Digestion. 1988;39(2):80–90. doi: 10.1159/000199610. [DOI] [PubMed] [Google Scholar]
- Coghlan J. G., Gilligan D., Humphries H., McKenna D., Dooley C., Sweeney E., Keane C., O'Morain C. Campylobacter pylori and recurrence of duodenal ulcers--a 12-month follow-up study. Lancet. 1987 Nov 14;2(8568):1109–1111. doi: 10.1016/s0140-6736(87)91545-5. [DOI] [PubMed] [Google Scholar]
- Collen M. J., Stanczak V. J., Ciarleglio C. A. Refractory duodenal ulcers (nonhealing duodenal ulcers with standard doses of antisecretory medication). Dig Dis Sci. 1989 Feb;34(2):233–237. doi: 10.1007/BF01536057. [DOI] [PubMed] [Google Scholar]
- Delchier J. C., Isal J. P., Eriksson S., Soule J. C. Double blind multicentre comparison of omeprazole 20 mg once daily versus ranitidine 150 mg twice daily in the treatment of cimetidine or ranitidine resistant duodenal ulcers. Gut. 1989 Sep;30(9):1173–1178. doi: 10.1136/gut.30.9.1173. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gledhill T., Buck M., Hunt R. H. Effect of no treatment, cimetidine 1 g/day, cimetidine 2 g/day and cimetidine combined with atropine on nocturnal gastric secretion in cimetidine non-responders. Gut. 1984 Nov;25(11):1211–1216. doi: 10.1136/gut.25.11.1211. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hall D. W. Review of the modes of action of colloidal bismuth subcitrate. Scand J Gastroenterol Suppl. 1989;157:3–22. doi: 10.3109/00365528909091043. [DOI] [PubMed] [Google Scholar]
- Hamilton I., O'Connor H. J., Wood N. C., Bradbury I., Axon A. T. Healing and recurrence of duodenal ulcer after treatment with tripotassium dicitrato bismuthate (TDB) tablets or cimetidine. Gut. 1986 Jan;27(1):106–110. doi: 10.1136/gut.27.1.106. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Johnston D. A., Wormsley K. G. The effects of fasting on 24-h gastric secretion of patients with duodenal ulcers resistant to ranitidine. Aliment Pharmacol Ther. 1989 Oct;3(5):471–479. doi: 10.1111/j.1365-2036.1989.tb00238.x. [DOI] [PubMed] [Google Scholar]
- Konturek S. J., Radecki T., Piastucki I., Drozdowicz D. Advances in the understanding of the mechanism of cytoprotective action by colloidal bismuth subcitrate. Scand J Gastroenterol Suppl. 1986;122:6–10. doi: 10.3109/00365528609102578. [DOI] [PubMed] [Google Scholar]
- Lam S. K., Lee N. W., Koo J., Hui W. M., Fok K. H., Ng M. Randomised crossover trial of tripotassium dicitrato bismuthate versus high dose cimetidine for duodenal ulcers resistant to standard dose of cimetidine. Gut. 1984 Jul;25(7):703–706. doi: 10.1136/gut.25.7.703. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lee F. I., Samloff I. M., Hardman M. Comparison of tri-potassium di-citrato bismuthate tablets with ranitidine in healing and relapse of duodenal ulcers. Lancet. 1985 Jun 8;1(8441):1299–1302. doi: 10.1016/s0140-6736(85)92793-x. [DOI] [PubMed] [Google Scholar]
- Manhart M. D. In vitro antimicrobial activity of bismuth subsalicylate and other bismuth salts. Rev Infect Dis. 1990 Jan-Feb;12 (Suppl 1):S11–S15. doi: 10.1093/clinids/12.supplement_1.s11. [DOI] [PubMed] [Google Scholar]
- Marshall B. J., Goodwin C. S., Warren J. R., Murray R., Blincow E. D., Blackbourn S. J., Phillips M., Waters T. E., Sanderson C. R. Prospective double-blind trial of duodenal ulcer relapse after eradication of Campylobacter pylori. Lancet. 1988 Dec 24;2(8626-8627):1437–1442. doi: 10.1016/s0140-6736(88)90929-4. [DOI] [PubMed] [Google Scholar]
- Rauws E. A., Langenberg W., Houthoff H. J., Zanen H. C., Tytgat G. N. Campylobacter pyloridis-associated chronic active antral gastritis. A prospective study of its prevalence and the effects of antibacterial and antiulcer treatment. Gastroenterology. 1988 Jan;94(1):33–40. [PubMed] [Google Scholar]
- Rauws E. A., Tytgat G. N. Cure of duodenal ulcer associated with eradication of Helicobacter pylori. Lancet. 1990 May 26;335(8700):1233–1235. doi: 10.1016/0140-6736(90)91301-p. [DOI] [PubMed] [Google Scholar]
- Savarino V., Mela G. S., Scalabrini P., Celle G. H2-receptor antagonist non-responders. Lancet. 1987 Nov 28;2(8570):1281–1281. doi: 10.1016/s0140-6736(87)91898-8. [DOI] [PubMed] [Google Scholar]
- Stolte M., Eidt S., Ritter M., Bethke B. Campylobacter pylori und Gastritis. Assoziation oder Induktion? Pathologe. 1989 Jan;10(1):21–26. [PubMed] [Google Scholar]
- Tytgat G. N. Colloidal bismuth subcitrate in peptic ulcer--a review. Digestion. 1987;37 (Suppl 2):31–41. doi: 10.1159/000199556. [DOI] [PubMed] [Google Scholar]
- Tytgat G. N., Lamers C. B., Hameeteman W., Jansen J. M., Wilson J. A. Omeprazole in peptic ulcers resistant to histamine H2-receptor antagonists. Aliment Pharmacol Ther. 1987 Feb;1(1):31–38. doi: 10.1111/j.1365-2036.1987.tb00603.x. [DOI] [PubMed] [Google Scholar]
- Wagner S., Freise J., Bär W., Fritsch S., Schmidt F. W. Epidemiologie und Therapie der Campylobacter-pylori-Infektion. Dtsch Med Wochenschr. 1989 Mar 17;114(11):407–413. doi: 10.1055/s-2008-1066609. [DOI] [PubMed] [Google Scholar]
- Wagstaff A. J., Benfield P., Monk J. P. Colloidal bismuth subcitrate. A review of its pharmacodynamic and pharmacokinetic properties, and its therapeutic use in peptic ulcer disease. Drugs. 1988 Aug;36(2):132–157. doi: 10.2165/00003495-198836020-00002. [DOI] [PubMed] [Google Scholar]
- Wormsley K. G. Duodenal ulcers which do not heal rapidly. Br Med J (Clin Res Ed) 1984 Oct 27;289(6452):1095–1095. doi: 10.1136/bmj.289.6452.1095. [DOI] [PMC free article] [PubMed] [Google Scholar]