

Abstract
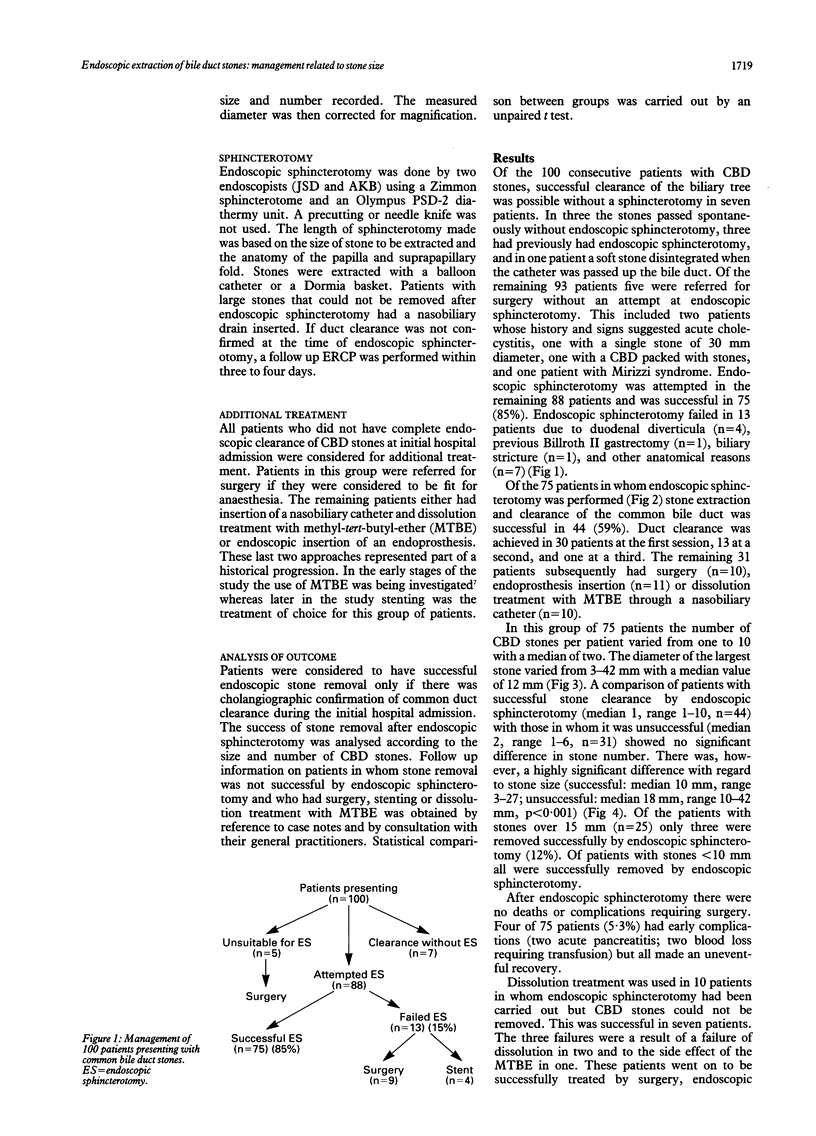
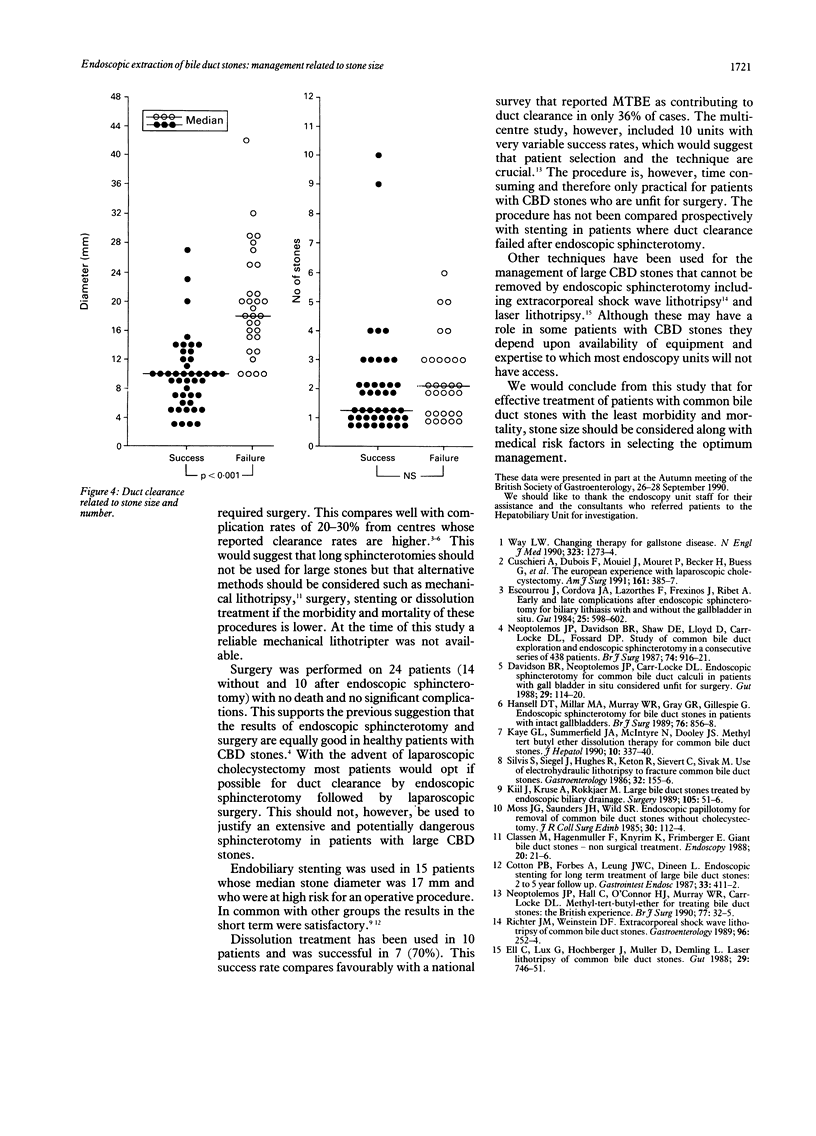
Endoscopic sphincterotomy has become the first line treatment for patients with common bile duct (CBD) stones. This technique may fail, however, due to difficult anatomy, previous surgery, periampullary diverticula or the presence of a large stone. The importance of stone size to the success of endoscopic sphincterotomy has not been fully assessed. A prospective study was carried out over the period January 1987 to December 1989 on 100 patients (45 male, 55 female, median age 69 years, range 19-97) with CBD stones in which a policy of early duct clearance was followed. Endoscopic retrograde cholangiopancreatography (ERCP) was performed and the stone size and number recorded from the cholangiograms and corrected for magnification. Sphincterotomy was performed using a diathermy unit with a cutting current and stones were extracted using a balloon catheter or a Dormia basket. Of the 100 patients with CBD stones receiving ERCP, successful clearance of the biliary tree was possible in seven without endoscopic sphincterotomy and five were felt to be unsuitable for endoscopic sphincterotomy. Of the remaining 88 patients endoscopic sphincterotomy was successful in 75 (85%). Of the 75 patients having endoscopic sphincterotomy stone clearance was successful in 44 (59%). There were no deaths and only four complications, which rapidly resolved on conservative treatment (two acute pancreatitis, two bleeding). The number of CBD stones present was similar in those patients with successful endoscopic sphincterotomy and duct clearance (median 1, range 1-10, n = 44) as in those in whom it failed (median 2, range 1-6, n = 31). In contrast there was a highly significant difference when stone size was analysed (successful clearance median stone size 10 mm, range 3-27 mm; unsuccessful: median 18 mm, range 10-42, p<0.001). Stones less than 10 mm in diameter (n=21) were all removed successfully whereas in patients with stones over 15 mm (n=25) only three were removed endoscopically (12%). All patients with evidence of residual stones had additional treatment. Of these 31 patients, 10 had surgery, 11 had insertion of an endoprosthesis, and 10 had dissolution treatment with methyl-tert-butyl ether through a nasobiliary catheter. This study shows the importance of stone size to the success rate of endoscopic removal of bile duct stones.
Full text
PDF

Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Classen M., Hagenmüller F., Knyrim K., Frimberger E. Giant bile duct stones--non-surgical treatment. Endoscopy. 1988 Jan;20(1):21–26. doi: 10.1055/s-2007-1018119. [DOI] [PubMed] [Google Scholar]
- Cotton P. B., Forbes A., Leung J. W., Dineen L. Endoscopic stenting for long-term treatment of large bile duct stones: 2- to 5-year follow-up. Gastrointest Endosc. 1987 Dec;33(6):411–412. doi: 10.1016/s0016-5107(87)71675-7. [DOI] [PubMed] [Google Scholar]
- Cuschieri A., Dubois F., Mouiel J., Mouret P., Becker H., Buess G., Trede M., Troidl H. The European experience with laparoscopic cholecystectomy. Am J Surg. 1991 Mar;161(3):385–387. doi: 10.1016/0002-9610(91)90603-b. [DOI] [PubMed] [Google Scholar]
- Davidson B. R., Neoptolemos J. P., Carr-Locke D. L. Endoscopic sphincterotomy for common bile duct calculi in patients with gall bladder in situ considered unfit for surgery. Gut. 1988 Jan;29(1):114–120. doi: 10.1136/gut.29.1.114. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ell C., Lux G., Hochberger J., Müller D., Demling L. Laserlithotripsy of common bile duct stones. Gut. 1988 Jun;29(6):746–751. doi: 10.1136/gut.29.6.746. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Escourrou J., Cordova J. A., Lazorthes F., Frexinos J., Ribet A. Early and late complications after endoscopic sphincterotomy for biliary lithiasis with and without the gall bladder 'in situ'. Gut. 1984 Jun;25(6):598–602. doi: 10.1136/gut.25.6.598. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hansell D. T., Millar M. A., Murray W. R., Gray G. R., Gillespie G. Endoscopic sphincterotomy for bile duct stones in patients with intact gallbladders. Br J Surg. 1989 Aug;76(8):856–858. doi: 10.1002/bjs.1800760831. [DOI] [PubMed] [Google Scholar]
- Kaye G. L., Summerfield J. A., McIntyre N., Dooley J. S. Methyl tert butyl ether dissolution therapy for common bile duct stones. J Hepatol. 1990 May;10(3):337–340. doi: 10.1016/0168-8278(90)90142-e. [DOI] [PubMed] [Google Scholar]
- Kiil J., Kruse A., Rokkjaer M. Large bile duct stones treated by endoscopic biliary drainage. Surgery. 1989 Jan;105(1):51–56. [PubMed] [Google Scholar]
- Moss J. G., Saunders J. H., Wild S. R. Endoscopic papillotomy for removal of common bile duct stones without cholecystectomy. J R Coll Surg Edinb. 1985 Apr;30(2):112–114. [PubMed] [Google Scholar]
- Neoptolemos J. P., Davidson B. R., Shaw D. E., Lloyd D., Carr-Locke D. L., Fossard D. P. Study of common bile duct exploration and endoscopic sphincterotomy in a consecutive series of 438 patients. Br J Surg. 1987 Oct;74(10):916–921. doi: 10.1002/bjs.1800741014. [DOI] [PubMed] [Google Scholar]
- Neoptolemos J. P., Hall C., O'Connor H. J., Murray W. R., Carr-Locke D. L. Methyl-tert-butyl-ether for treating bile duct stones: the British experience. Br J Surg. 1990 Jan;77(1):32–35. doi: 10.1002/bjs.1800770111. [DOI] [PubMed] [Google Scholar]
- Richter J. M., Weinstein D. F. Extracorporeal shock-wave lithotripsy of common bile duct stones. Gastroenterology. 1989 Jan;96(1):252–254. doi: 10.1016/0016-5085(89)90791-9. [DOI] [PubMed] [Google Scholar]
- Way L. W. Changing therapy for gallstone disease. N Engl J Med. 1990 Nov 1;323(18):1273–1274. doi: 10.1056/NEJM199011013231810. [DOI] [PubMed] [Google Scholar]