

Abstract
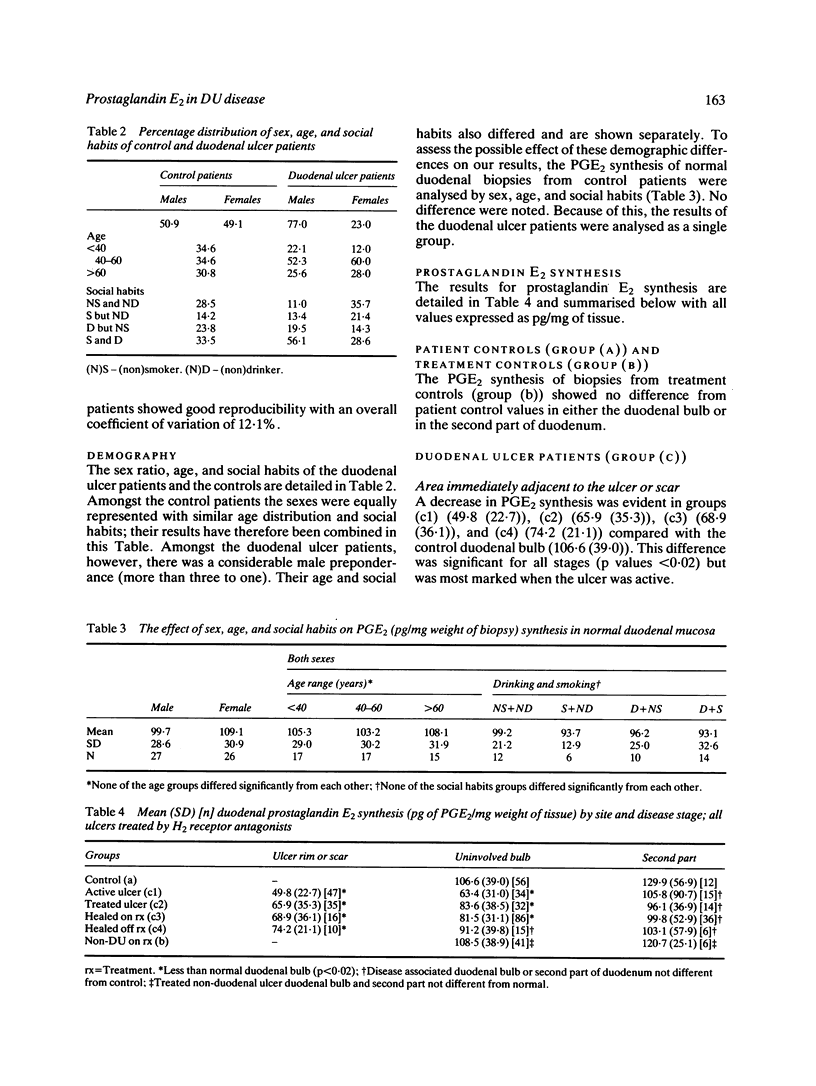
We tested the hypothesis that the production of prostaglandin E2 (PGE2) is impaired in duodenal ulcer disease and affected by treatment and healing. This was investigated by a study of maximal PGE2 synthesis rates in duodenal and antral mucosal biopsies obtained at endoscopy. The patients were divided into three groups. Group (a): endoscopically normal controls (n = 56); group (b): treatment controls (non-DU disease: gastric ulcer or oesophagitis treated by histamine H2 receptor antagonists) (n = 41); and group (c): patients with DU disease (n = 183) further subdivided into group (c1) active ulcer not on treatment (n = 47), (c2) treated active ulcer (n = 35), (c3) healed ulcer on treatment (n = 86), and (c4) healed ulcer not on treatment (n = 15). Group (a) synthesised (mean (SD] 106.6 (39.0) pg PGE2/mg wt of tissue from the duodenal bulb and 129.9 (56.9) from the second part of the duodenum. No difference was found between group (a) and (b) at either site. Group (c1) ulcer rim made 49.8 (22.7) and at all stages ulcer rim and scar made less than the control duodenal bulb (p less than 0.02). Uninvolved duodenal bulb form groups (c1) (63.4 (31.0], (c2) (83.6 (38.5], and (c3) (81.5 (31.1], however, also made significantly less than controls (p less than 0.02) and a similar though non-significant trend was seen in group (c4). Biopsies from the second part of the duodenum did not synthesise significantly less than the control group but a similar trend was noticed at each stage of ulcer treatment. Biopsies of control antrum synthesised 124.5 (32.2) but only 93.7 (44.2) in group (cl) (p < 0.005). All stages of duodenal ulcer healing were associated with a decreased capacity to synthesise the major prostaglandin PGE2 at the ulcer site and the uninvolved duodenal bulb and, in acute untreated duodenal ulcer, the uninvolved antrum. This decreased capacity may be the consequence of the disease process itself and not secondary to the treatment, indicating a basic pathophysiological abnormality which may explain the characteristic tendency of the disease to relapse.
Full text
PDF
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Crampton J. R., Gibbons L. C., Rees W. D. Simultaneous measurement of in vitro gastroduodenal prostaglandin E2 synthesis and degradation in peptic ulcer disease. Scand J Gastroenterol. 1987 May;22(4):425–430. doi: 10.3109/00365528708991485. [DOI] [PubMed] [Google Scholar]
- Dajani E. Z. Is peptic ulcer a prostaglandin deficiency disease? Hum Pathol. 1986 Feb;17(2):106–107. doi: 10.1016/s0046-8177(86)80281-7. [DOI] [PubMed] [Google Scholar]
- Hawkey C. J., Rampton D. S. Prostaglandins and the gastrointestinal mucosa: are they important in its function, disease, or treatment? Gastroenterology. 1985 Nov;89(5):1162–1188. doi: 10.1016/0016-5085(85)90225-2. [DOI] [PubMed] [Google Scholar]
- Hillier K., Smith C. L., Jewell R., Arthur M. J., Ross G. Duodenal mucosa synthesis of prostaglandins in duodenal ulcer disease. Gut. 1985 Mar;26(3):237–240. doi: 10.1136/gut.26.3.237. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Isenberg J. I., Selling J. A., Hogan D. L., Koss M. A. Impaired proximal duodenal mucosal bicarbonate secretion in patients with duodenal ulcer. N Engl J Med. 1987 Feb 12;316(7):374–379. doi: 10.1056/NEJM198702123160704. [DOI] [PubMed] [Google Scholar]
- McCready D. R., Clark L., Cohen M. M. Cigarette smoking reduces human gastric luminal prostaglandin E2. Gut. 1985 Nov;26(11):1192–1196. doi: 10.1136/gut.26.11.1192. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Miller J. P., Faragher E. B. Relapse of duodenal ulcer: does it matter which drug is used in initial treatment? Br Med J (Clin Res Ed) 1986 Nov 1;293(6555):1117–1118. doi: 10.1136/bmj.293.6555.1117. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Puurunen J. Effect of prostaglandin E2, cimetidine, and atropine on ethanol-induced gastric mucosal damage in the rat. Scand J Gastroenterol. 1980;15(4):485–488. doi: 10.3109/00365528009181505. [DOI] [PubMed] [Google Scholar]
- Quigley E. M., Turnberg L. A. pH of the microclimate lining human gastric and duodenal mucosa in vivo. Studies in control subjects and in duodenal ulcer patients. Gastroenterology. 1987 Jun;92(6):1876–1884. doi: 10.1016/0016-5085(87)90619-6. [DOI] [PubMed] [Google Scholar]
- Robert A. Antisecretory, antiulcer, cytoprotective and diarrheogenic properties of prostaglandins. Adv Prostaglandin Thromboxane Res. 1976;2:507–520. [PubMed] [Google Scholar]
- Robert A., Nezamis J. E., Lancaster C., Hanchar A. J. Cytoprotection by prostaglandins in rats. Prevention of gastric necrosis produced by alcohol, HCl, NaOH, hypertonic NaCl, and thermal injury. Gastroenterology. 1979 Sep;77(3):433–443. [PubMed] [Google Scholar]
- Sharon P., Cohen F., Zifroni A., Karmeli F., Ligumsky M., Rachmilewitz D. Prostanoid synthesis by cultured gastric and duodenal mucosa: Possible role in the pathogenesis of duodenal ulcer. Scand J Gastroenterol. 1983 Nov;18(8):1045–1049. doi: 10.3109/00365528309181838. [DOI] [PubMed] [Google Scholar]
- Wright J. P., Young G. O., Klaff L. J., Weers L. A., Price S. K., Marks I. N. Gastric mucosal prostaglandin E levels in patients with gastric ulcer disease and carcinoma. Gastroenterology. 1982 Feb;82(2):263–267. [PubMed] [Google Scholar]