

Abstract
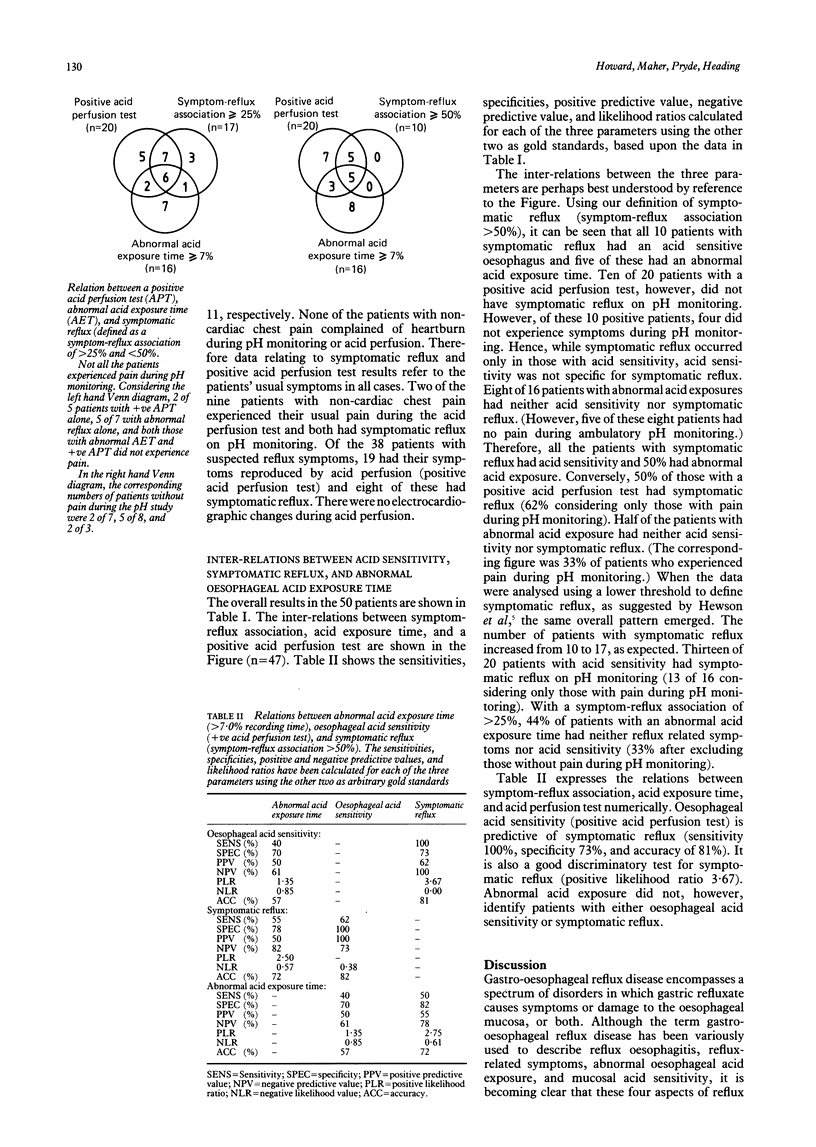
The Bernstein test has been used as a test of oesophageal acid sensitivity for over 30 years but its clinical value has been challenged by the advent of ambulatory pH monitoring. Furthermore, the relation between mucosal acid sensitivity, symptomatic reflux, and abnormal oesophageal acid exposure time is unclear. This study examined the relation between these three parameters in patients referred for pH monitoring with unexplained chest pain or heartburn. Fifty consecutive patients were studied - nine with non-cardiac chest pain and 41 with a history of heartburn. Symptomatic reflux was defined as a greater than or equal to 50% temporal association between pain episodes and reflux events (pH less than 4) during pH monitoring. A positive acid perfusion test (in which the patient's usual symptoms were evoked by acid, though not saline) had a 100% sensitivity, 73% specificity, and 81% accuracy for the detection of symptomatic reflux. All 10 patients with symptomatic reflux during pH monitoring had evidence of mucosal acid sensitivity. A negative acid perfusion test made symptomatic reflux unlikely. However, symptomatic reflux or a positive acid perfusion test, or both, were found in some patients with a normal oesophageal acid exposure time during pH monitoring. Mucosal acid sensitivity, abnormal oesophageal acid exposure time, and symptomatic reflux should be regarded as separate, though related aspects of reflux disease. The Bernstein test is simple, safe, and easily performed. A positive test helps to identify an oesophageal cause of symptoms, particularly in patients in whom other aspects of 'gastro-oesophageal reflux disease' are absent, or who do not have symptoms during pH monitoring.
Full text
PDF


Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- BERNSTEIN L. M., BAKER L. A. A clinical test for esophagitis. Gastroenterology. 1958 May;34(5):760–781. [PubMed] [Google Scholar]
- Behar J., Biancani P., Sheahan D. G. Evaluation of esophageal tests in the diagnosis of reflux esophagitis. Gastroenterology. 1976 Jul;71(1):9–15. [PubMed] [Google Scholar]
- Bennett J. R., Atkinson M. Oesophageal acid-perfusion in the diagnosis of precordial pain. Lancet. 1966 Nov 26;2(7474):1150–1152. doi: 10.1016/s0140-6736(66)90472-7. [DOI] [PubMed] [Google Scholar]
- Benz L. J., Hootkin L. A., Margulies S., Donner M. W., Cauthorne R. T., Hendrix T. R. A comparison of clinical measurements of gastroesophageal reflux. Gastroenterology. 1972 Jan;62(1):1–5. [PubMed] [Google Scholar]
- Breen K. J., Whelan G. The diagnosis of reflux oesophagitis: an evaluation of five investigative procedures. Aust N Z J Surg. 1978 Apr;48(2):156–161. doi: 10.1111/j.1445-2197.1978.tb07294.x. [DOI] [PubMed] [Google Scholar]
- De Caestecker J. S., Pryde A., Heading R. C. Comparison of intravenous edrophonium and oesophageal acid perfusion during oesophageal manometry in patients with non-cardiac chest pain. Gut. 1988 Aug;29(8):1029–1034. doi: 10.1136/gut.29.8.1029. [DOI] [PMC free article] [PubMed] [Google Scholar]
- DeMeester T. R., Wang C. I., Wernly J. A., Pellegrini C. A., Little A. G., Klementschitsch P., Bermudez G., Johnson L. F., Skinner D. B. Technique, indications, and clinical use of 24 hour esophageal pH monitoring. J Thorac Cardiovasc Surg. 1980 May;79(5):656–670. [PubMed] [Google Scholar]
- Hewson E. G., Sinclair J. W., Dalton C. B., Wu W. C., Castell D. O., Richter J. E. Acid perfusion test: does it have a role in the assessment of non cardiac chest pain? Gut. 1989 Mar;30(3):305–310. doi: 10.1136/gut.30.3.305. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Janssens J., Vantrappen G., Ghillebert G. 24-hour recording of esophageal pressure and pH in patients with noncardiac chest pain. Gastroenterology. 1986 Jun;90(6):1978–1984. doi: 10.1016/0016-5085(86)90270-2. [DOI] [PubMed] [Google Scholar]
- Johansson K. E., Boeryd B., Johansson K., Tibbling L. Double-blind crossover study of ranitidine and placebo in gastro-oesophageal reflux disease. Scand J Gastroenterol. 1986 Sep;21(7):769–778. doi: 10.3109/00365528609011116. [DOI] [PubMed] [Google Scholar]
- Kaul B., Petersen H., Grette K., Myrvold H. E., Halvorsen T. The acid perfusion test in gastroesophageal reflux disease. Scand J Gastroenterol. 1986 Jan;21(1):93–96. doi: 10.3109/00365528609034629. [DOI] [PubMed] [Google Scholar]
- Kjellén G., Tibbling L. Oesophageal motility during acid-provoked heartburn and chest pain. Scand J Gastroenterol. 1985 Oct;20(8):937–940. doi: 10.3109/00365528509088851. [DOI] [PubMed] [Google Scholar]
- Palmer E. D. The hiatus hernia-esophagitis-esophageal stricture complex. Twenty-year prospective study. Am J Med. 1968 Apr;44(4):566–579. doi: 10.1016/0002-9343(68)90057-0. [DOI] [PubMed] [Google Scholar]
- Peters L., Maas L., Petty D., Dalton C., Penner D., Wu W., Castell D., Richter J. Spontaneous noncardiac chest pain. Evaluation by 24-hour ambulatory esophageal motility and pH monitoring. Gastroenterology. 1988 Apr;94(4):878–886. [PubMed] [Google Scholar]
- Richter J. E., Barish C. F., Castell D. O. Abnormal sensory perception in patients with esophageal chest pain. Gastroenterology. 1986 Oct;91(4):845–852. doi: 10.1016/0016-5085(86)90685-2. [DOI] [PubMed] [Google Scholar]
- SIEGEL C. I., HENDRIX T. R. Esophageal motor abnormalities induced by acid perfusion in patients with heartburn. J Clin Invest. 1963 May;42:686–695. doi: 10.1172/JCI104760. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Schindlbeck N. E., Heinrich C., König A., Dendorfer A., Pace F., Müller-Lissner S. A. Optimal thresholds, sensitivity, and specificity of long-term pH-metry for the detection of gastroesophageal reflux disease. Gastroenterology. 1987 Jul;93(1):85–90. doi: 10.1016/0016-5085(87)90318-0. [DOI] [PubMed] [Google Scholar]
- Simel D. L. Playing the odds. Lancet. 1985 Feb 9;1(8424):329–330. doi: 10.1016/s0140-6736(85)91093-1. [DOI] [PubMed] [Google Scholar]
- Skinner D. B., Booth D. J. Assessment of distal esophageal function in patients with hiatal hernia and-or gastroesophageal reflux. Ann Surg. 1970 Oct;172(4):627–637. doi: 10.1097/00000658-197010000-00009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sladen G. E., Riddell R. H., Willoughby J. M. Oesophagoscopy, biopsy, and acid perfusion test in diagnosis of "reflux oesophagitis". Br Med J. 1975 Jan 11;1(5949):71–76. doi: 10.1136/bmj.1.5949.71. [DOI] [PMC free article] [PubMed] [Google Scholar]
- TUTTLE S. G., BETTARELLO A., GROSSMAN M. I. Esophageal acid perfusion test and a gastroesophageal reflux test in patients with esophagitis. Gastroenterology. 1960 Jun;38:861–872. [PubMed] [Google Scholar]
- TUTTLE S. G., RUFIN F., BETTARELLO A. The physiology of heartburn. Ann Intern Med. 1961 Aug;55:292–300. doi: 10.7326/0003-4819-55-2-292. [DOI] [PubMed] [Google Scholar]
- Vantrappen G., Janssens J., Ghillebert G. The irritable oesophagus--a frequent cause of angina-like pain. Lancet. 1987 May 30;1(8544):1232–1234. doi: 10.1016/s0140-6736(87)92686-9. [DOI] [PubMed] [Google Scholar]
- de Caestecker J. S., Blackwell J. N., Brown J., Heading R. C. The oesophagus as a cause of recurrent chest pain: which patients should be investigated and which tests should be used? Lancet. 1985 Nov 23;2(8465):1143–1146. doi: 10.1016/s0140-6736(85)92676-5. [DOI] [PubMed] [Google Scholar]
- de Caestecker J. S. Twenty-four-hour oesophageal pH monitoring: advances and controversies. Neth J Med. 1989 Mar;34 (Suppl):S20–S39. [PubMed] [Google Scholar]