

Abstract
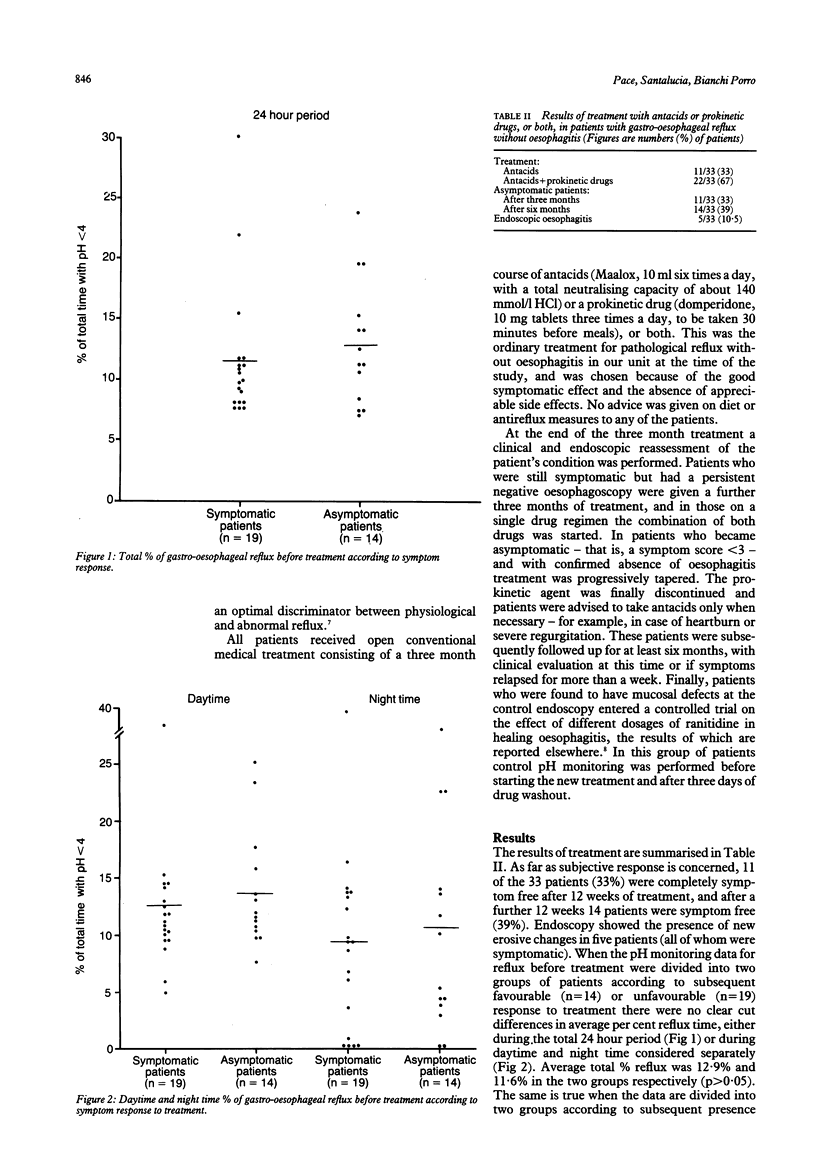
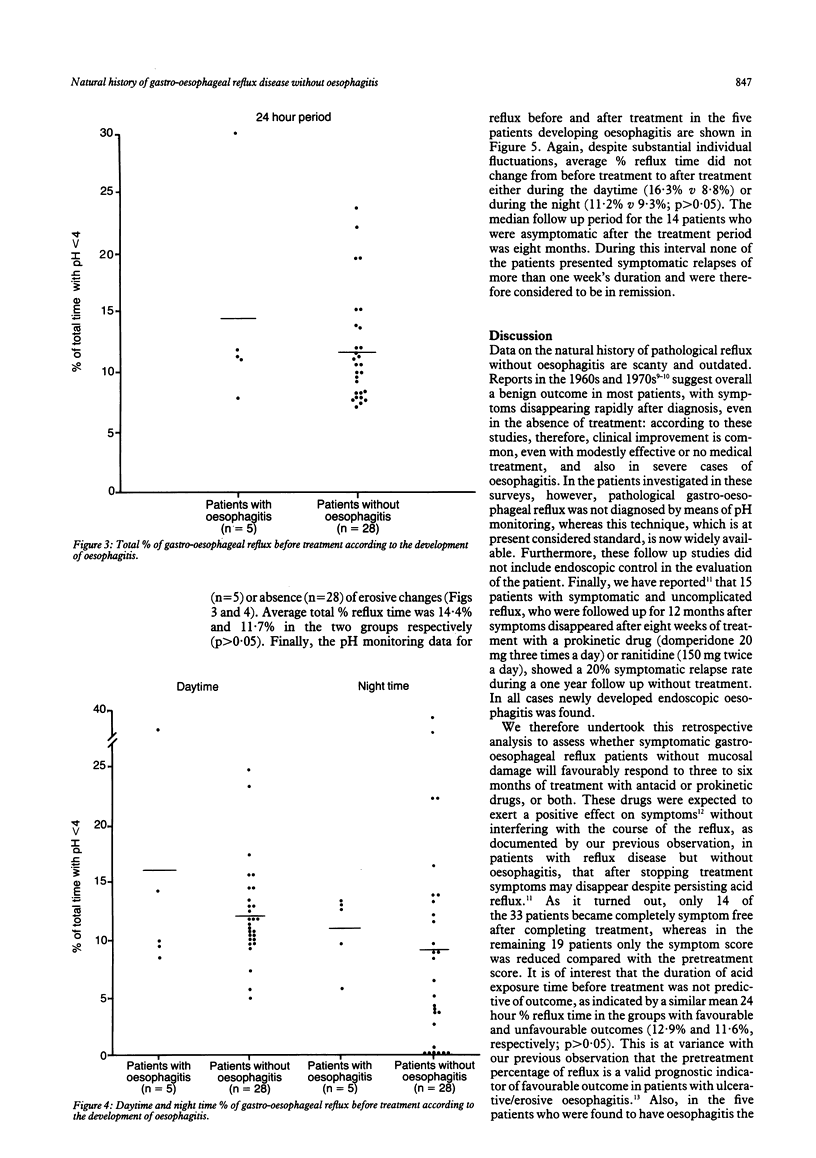
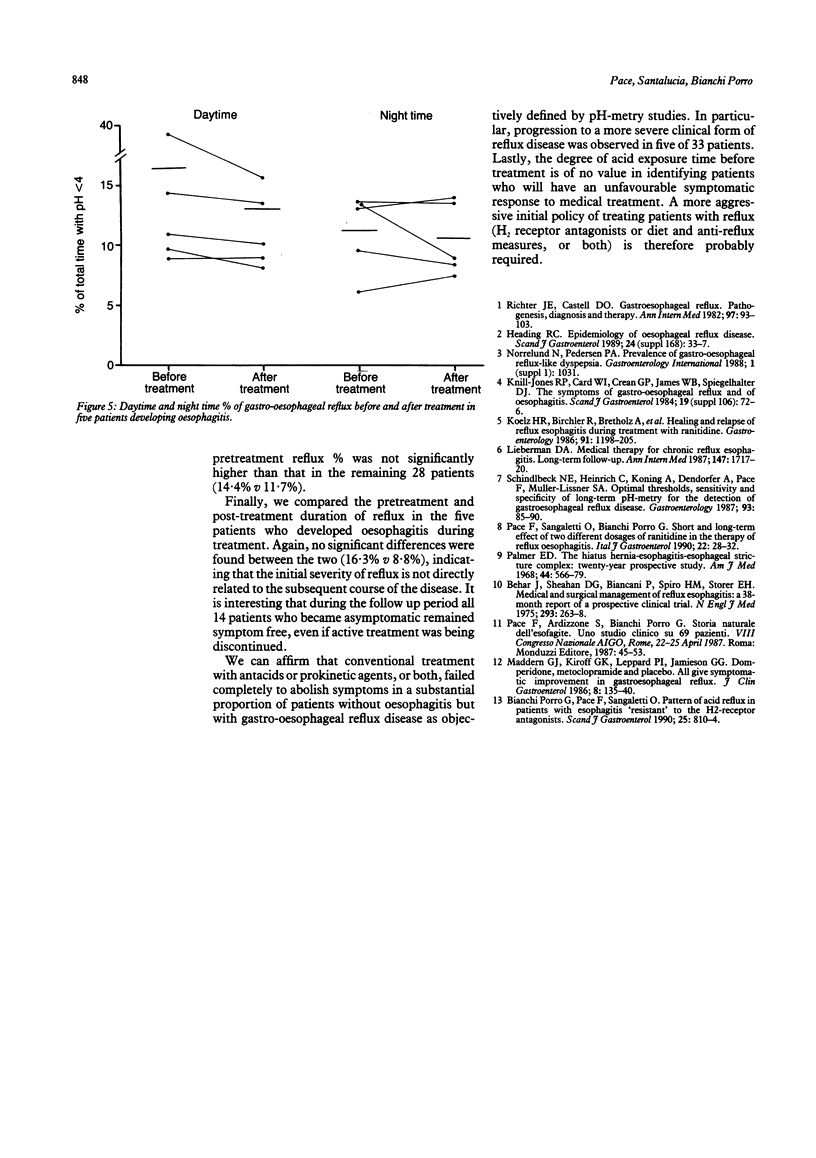
This retrospective study was undertaken to characterise the clinical course and reflux pattern of patients with gastro-oesophageal reflux without evidence of oesophagitis. We investigated 33 patients (12 women, 21 men; mean age 36 years) with typical symptoms, a negative oesophagoscopy, and a 24 hour oesophageal pH-metry indicative of pathological gastro-oesophageal reflux. All patients received antacids or prokinetic drugs or both for three to six months. Nineteen of 33 patients still had symptoms at the end of treatment, of whom five had developed erosive changes of the oesophageal mucosa. The other 14 discontinued treatment and remained asymptomatic during a six month follow up period. Comparison of the pretreatment pH-metry data of the 19 symptomatic patients and the 14 asymptomatic patients showed no differences in the pattern of gastro-oesophageal reflux in the two groups. We conclude that in a substantial proportion of patients with pathological reflux without oesophagitis symptoms may persist and mucosal lesions may develop during conventional treatment without any apparent change in the reflux. Patients who developed endoscopic oesophagitis did not have a more severe pretreatment pattern of gastro-oesophageal reflux when compared with those who did not develop oesophageal mucosal damage.
Full text
PDF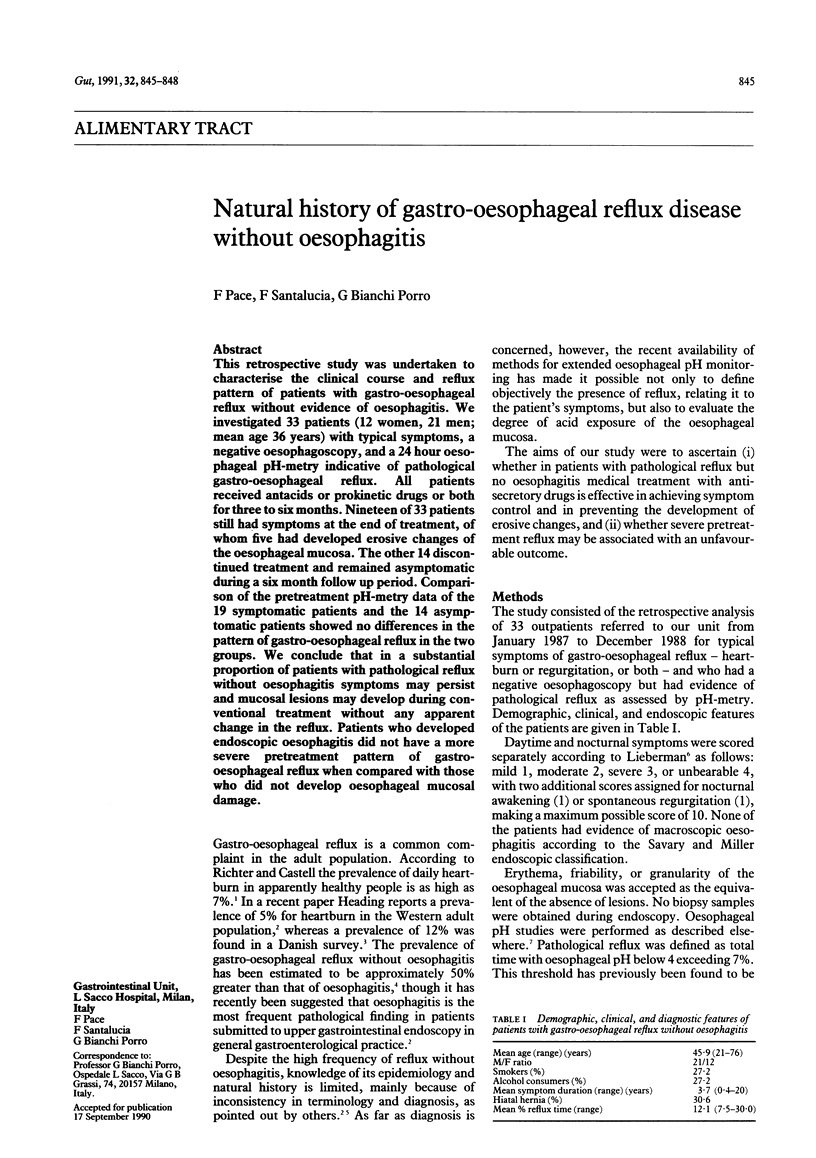
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Behar J., Sheahan D. G., Biancani P., Spiro H. M., Storer E. H. Medical and surgical management of reflux esophagitis. A 38-month report of a prospective clinical trial. N Engl J Med. 1975 Aug 7;293(6):263–268. doi: 10.1056/NEJM197508072930602. [DOI] [PubMed] [Google Scholar]
- Bianchi Porro G., Pace F., Sangaletti O. Pattern of acid reflux in patients with reflux esophagitis 'resistant' to H2-receptor antagonists. Scand J Gastroenterol. 1990 Aug;25(8):810–814. doi: 10.3109/00365529008999219. [DOI] [PubMed] [Google Scholar]
- Heading R. C. Epidemiology of oesophageal reflux disease. Scand J Gastroenterol Suppl. 1989;168:33–37. [PubMed] [Google Scholar]
- Koelz H. R., Birchler R., Bretholz A., Bron B., Capitaine Y., Delmore G., Fehr H. F., Fumagalli I., Gehrig J., Gonvers J. J. Healing and relapse of reflux esophagitis during treatment with ranitidine. Gastroenterology. 1986 Nov;91(5):1198–1205. doi: 10.1016/s0016-5085(86)80017-8. [DOI] [PubMed] [Google Scholar]
- Lieberman D. A. Medical therapy for chronic reflux esophagitis. Long-term follow-up. Arch Intern Med. 1987 Oct;147(10):1717–1720. [PubMed] [Google Scholar]
- Maddern G. J., Kiroff G. K., Leppard P. I., Jamieson G. G. Domperidone, metoclopramide, and placebo. All give symptomatic improvement in gastroesophageal reflux. J Clin Gastroenterol. 1986 Apr;8(2):135–140. [PubMed] [Google Scholar]
- Pace F., Sangaletti O., Bianchi Porro G. Short and long-term effect of two different dosages of ranitidine in the therapy of reflux oesophagitis. Ital J Gastroenterol. 1990 Feb;22(1):28–32. [PubMed] [Google Scholar]
- Richter J. E., Castell D. O. Gastroesophageal reflux. Pathogenesis, diagnosis, and therapy. Ann Intern Med. 1982 Jul;97(1):93–103. doi: 10.7326/0003-4819-97-1-93. [DOI] [PubMed] [Google Scholar]
- Schindlbeck N. E., Heinrich C., König A., Dendorfer A., Pace F., Müller-Lissner S. A. Optimal thresholds, sensitivity, and specificity of long-term pH-metry for the detection of gastroesophageal reflux disease. Gastroenterology. 1987 Jul;93(1):85–90. doi: 10.1016/0016-5085(87)90318-0. [DOI] [PubMed] [Google Scholar]