

Abstract
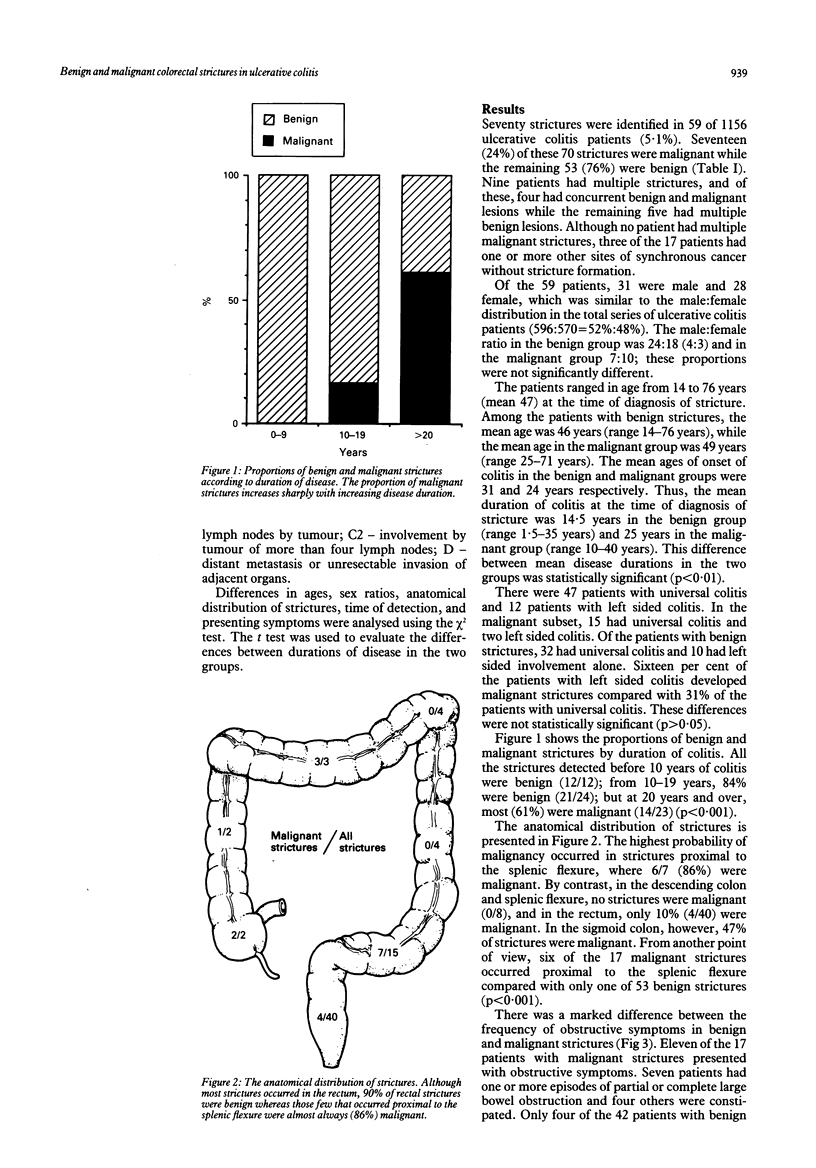
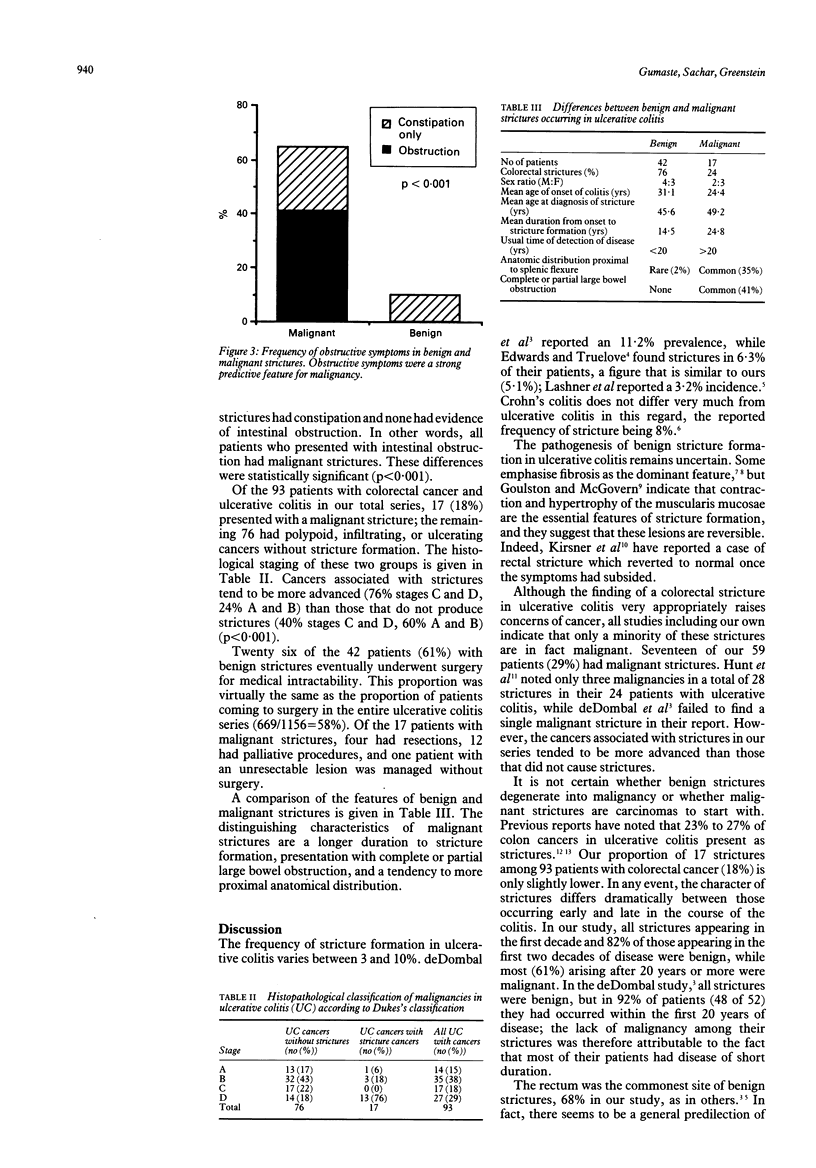
Colorectal strictures, either benign or malignant, are not uncommon in ulcerative colitis. Fifty nine of 1156 ulcerative colitis patients (5%) admitted to this hospital between 1959 and 1983 developed 70 separate colorectal strictures. Seventeen of the 70 strictures (24%) proved to be malignant and the other 53 benign. Nine patients developed more than one stricture. Three principal features distinguished the 17 malignant from the 53 benign strictures in this series: (1) appearance late in the course of ulcerative colitis (61% probability of malignancy in strictures that develop after 20 years of disease v 0% probability in those occurring before 10 years); (2) location proximal to the splenic flexure (86% probability of malignancy v 47% in sigmoid, 10% in rectum, and 0% in splenic flexure and descending colon); and (3) symptomatic large bowel obstruction (100% probability of malignancy v only 14% in the absence of obstruction or constipation). Moreover, cancer associated with strictures tends to be more advanced (76% stage D, 24% A and B) than that which does not produce strictures (18% stage D, 59% A and B).
Full text
PDF

Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- ASTLER V. B., COLLER F. A. The prognostic significance of direct extension of carcinoma of the colon and rectum. Ann Surg. 1954 Jun;139(6):846–852. doi: 10.1097/00000658-195406000-00015. [DOI] [PMC free article] [PubMed] [Google Scholar]
- De Dombal F. T., Watts J. M., Watkinson G., Goligher J. C. Local complications of ulcerative colitis: stricture, pseudopolyposis, and carcinoma of colon and rectum. Br Med J. 1966 Jun 11;1(5501):1442–1447. doi: 10.1136/bmj.1.5501.1442. [DOI] [PMC free article] [PubMed] [Google Scholar]
- EDWARDS F. C., TRUELOVE S. C. THE COURSE AND PROGNOSIS OF ULCERATIVE COLITIS. III. COMPLICATIONS. Gut. 1964 Feb;5:1–22. doi: 10.1136/gut.5.1.1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Goldberg H. I., Caruthers S. B., Jr, Nelson J. A., Singleton J. W. Radiographic findings of the National Cooperative Crohn's Disease Study. Gastroenterology. 1979 Oct;77(4 Pt 2):925–937. [PubMed] [Google Scholar]
- Goulston S. J., McGovern V. J. The nature of benign strictures in ulcerative colitis. N Engl J Med. 1969 Aug 7;281(6):290–295. doi: 10.1056/NEJM196908072810603. [DOI] [PubMed] [Google Scholar]
- Greenstein A. J., Sachar D. B., Smith H., Pucillo A., Papatestas A. E., Kreel I., Geller S. A., Janowitz H. D., Aufses A. H., Jr Cancer in universal and left-sided ulcerative colitis: factors determining risk. Gastroenterology. 1979 Aug;77(2):290–294. [PubMed] [Google Scholar]
- Hunt R. H., Teague R. H., Swarbrick E. T., Williams C. B. Colonoscopy in management of colonic strictures. Br Med J. 1975 Aug 9;3(5979):360–361. doi: 10.1136/bmj.3.5979.360. [DOI] [PMC free article] [PubMed] [Google Scholar]
- KIRSNER J. B., PALMER W. L., KLOTZ A. Reversibility in ulcerative colitis; clinical and roentgenologic observations. Radiology. 1951 Jul;57(1):1–14. doi: 10.1148/57.1.1. [DOI] [PubMed] [Google Scholar]
- LUMB G., PROTHEROE R. H. Ulcerative colitis; a pathologic study of 152 surgical specimens. Gastroenterology. 1958 Mar;34(3):381–407. [PubMed] [Google Scholar]
- LUMB G. Pathology of ulcerative colitis. Gastroenterology. 1961 Feb;40:290–298. [PubMed] [Google Scholar]
- Lashner B. A., Turner B. C., Bostwick D. G., Frank P. H., Hanauer S. B. Dysplasia and cancer complicating strictures in ulcerative colitis. Dig Dis Sci. 1990 Mar;35(3):349–352. doi: 10.1007/BF01537413. [DOI] [PubMed] [Google Scholar]