

Abstract
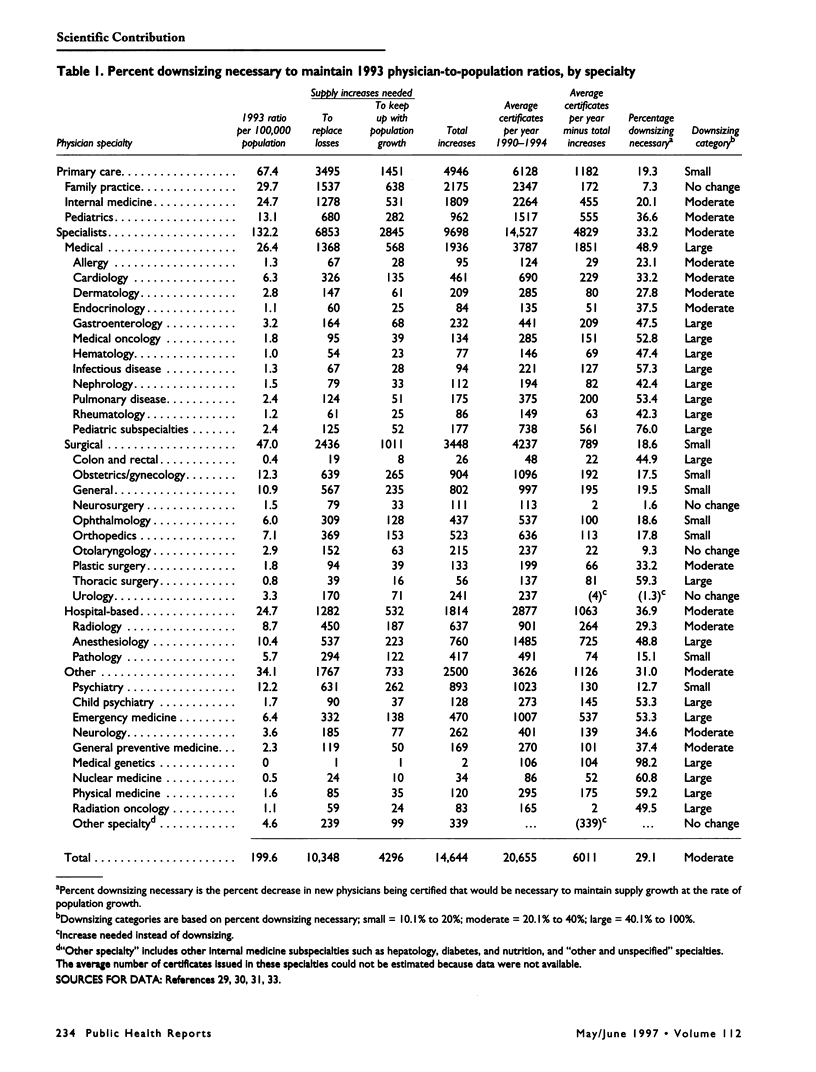
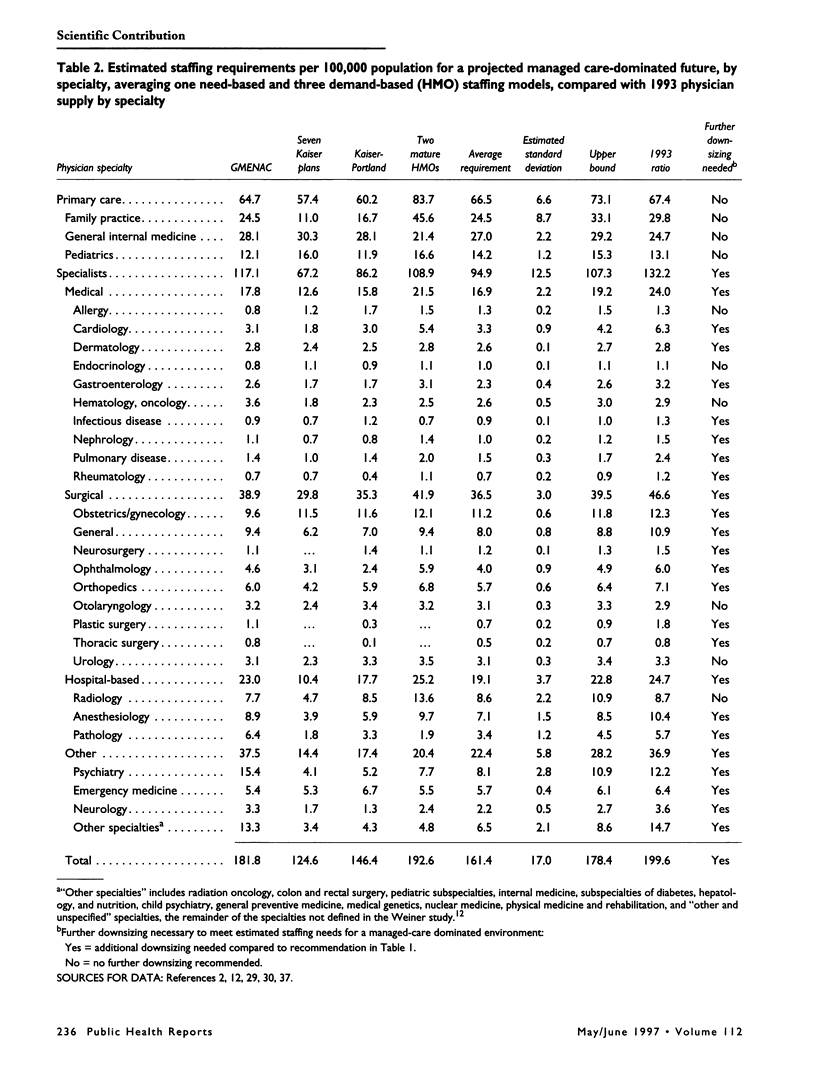
OBJECTIVE: To estimate the need for downsizing the physician workforce in a changing health care environment. METHODS: First assuming that 1993 physician-to-population ratios would be maintained, the authors derived downsizing estimates by determining the annual growth in the supply of specialists necessary to maintain these ratios (sum of losses from death and retirement plus increase necessary to parallel population growth) and compared them with an estimate of the number of new physicians being produced (average annual number of board certificates issued between 1990 and 1994). Then, assuming that workforce needs would change in a system increasingly dominated by managed care, the authors estimated specialty-specific downsizing needs for a managed care dominated environment using data from several sources. RESULTS: To maintain the 1993 199.6 active physicians per 100,000 population ratio, 14,644 new physicians would be needed each year. Given that an average of 20,655 physicians were certified each year between 1990 and 1994, at least 6011 fewer new physicians were needed annually to maintain 1993 levels. To maintain the 132.2 ratio of active non-primary care physicians per 100,000 population, the system needed to produce 9698 non-primary care physicians per year, because an average of 14,527 new non-primary care physicians entered the workforce between 1990 and 1994, downsizing by 4829, or 33%, was needed. To maintain the 66.8 active primary care physicians per 100,000 population ratio, 4946 new primary care physicians were needed per year, since primary care averaged 6128 new certifications per year, a downsizing of 1182, or 20% was indicated. Only family practice, neurosurgery, otolaryngology, and urology did not require downsizing. Seventeen medical and hospital-based specialties, including 7 of 10 internal medicine subspecialties, needed downsizing by at least 40%. Less downsizing in general was needed in the surgical specialties and in psychiatry. A managed care dominated-system would call for greater downsizing in most of the non-primary care specialties. CONCLUSION: These data support the need for downsizing the nation's physician supply, especially in the internal medicine subspecialties and hospital support specialties and to a lesser extent among surgeons and primary care physicians.
Full text
PDF



Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Bowman M. A., Katzoff J. M., Garrison L. P., Jr, Wills J. Estimates of physician requirements for 1990 for the specialties of neurology, anesthesiology, nuclear medicine, pathology, physical medicine and rehabilitation, and radiology. A further application of the GMENAC methodology. JAMA. 1983 Nov 18;250(19):2623–2627. [PubMed] [Google Scholar]
- Cooper R. A. Seeking a balanced physician workforce for the 21st century. JAMA. 1994 Sep 7;272(9):680–687. [PubMed] [Google Scholar]
- Ginzberg E. Physician supply policies and health reform. JAMA. 1992 Dec 2;268(21):3115–3118. [PubMed] [Google Scholar]
- Grumbach K., Lee P. R. How many physicians can we afford? JAMA. 1991 May 8;265(18):2369–2372. [PubMed] [Google Scholar]
- Hart L. G., Wagner E., Pirzada S., Nelson A. F., Rosenblatt R. A. Physician staffing ratios in staff-model HMOs: a cautionary tale. Health Aff (Millwood) 1997 Jan-Feb;16(1):55–70. doi: 10.1377/hlthaff.16.1.55. [DOI] [PubMed] [Google Scholar]
- Hussey D. H., Horton J. L., Mendenhall N. P., Munzenrider J. E., Rose C. M., Sunshine J. H. Manpower needs for radiation oncology: a preliminary report of the ASTRO Human Resources Committee. American Society for Therapeutic Radiology and Oncology. Int J Radiat Oncol Biol Phys. 1996 Jul 1;35(4):809–820. doi: 10.1016/0360-3016(96)00209-x. [DOI] [PubMed] [Google Scholar]
- Iglehart J. K. How many doctors do we need? The tenth annual Duke Private Sector Conference. JAMA. 1985 Oct 4;254(13):1785–1788. [PubMed] [Google Scholar]
- Jama J. W., Launer L. J., Witteman J. C., den Breeijen J. H., Breteler M. M., Grobbee D. E., Hofman A. Dietary antioxidants and cognitive function in a population-based sample of older persons. The Rotterdam Study. Am J Epidemiol. 1996 Aug 1;144(3):275–280. doi: 10.1093/oxfordjournals.aje.a008922. [DOI] [PubMed] [Google Scholar]
- Luft H. S., Arno P. Impact of increasing physician supply: a scenario for the future. Health Aff (Millwood) 1986 Winter;5(4):31–46. doi: 10.1377/hlthaff.5.4.31. [DOI] [PubMed] [Google Scholar]
- Meyer G. S., Jacoby I., Krakauer H., Powell D. W., Aurand J., McCardle P. Gastroenterology workforce modeling. JAMA. 1996 Sep 4;276(9):689–694. [PubMed] [Google Scholar]
- Miller R. S., Jonas H. S., Whitcomb M. E. The initial employment status of physicians completing training in 1994. JAMA. 1996 Mar 6;275(9):708–712. [PubMed] [Google Scholar]
- Mullan F. Iconoclasm and physician workforce research. Health Aff (Millwood) 1997 Jan-Feb;16(1):87–89. doi: 10.1377/hlthaff.16.1.87. [DOI] [PubMed] [Google Scholar]
- Mullan F., Politzer R. M., Davis C. H. Medical migration and the physician workforce. International medical graduates and American medicine. JAMA. 1995 May 17;273(19):1521–1527. doi: 10.1001/jama.1995.03520430057039. [DOI] [PubMed] [Google Scholar]
- Mullan F., Politzer R. M., Gamliel S., Rivo M. L. Balance and limits: modeling graduate medical education reform based on recommendations of the Council on Graduate Medical Education. Milbank Q. 1994;72(3):385–398. [PubMed] [Google Scholar]
- Politzer R. M., Gamliel S. R., Cultice J. M., Bazell C. M., Rivo M. L., Mullan F. Matching physician supply and requirements: testing policy recommendations. Inquiry. 1996 Summer;33(2):181–194. [PubMed] [Google Scholar]
- Rivo M. L., Mays H. L., Katzoff J., Kindig D. A. Managed health care. Implications for the physician workforce and medical education. Council on Graduate Medical Education. JAMA. 1995 Sep 6;274(9):712–715. doi: 10.1001/jama.274.9.712. [DOI] [PubMed] [Google Scholar]
- Schroeder S. A. The latest forecast. Managed care collides with physician supply. JAMA. 1994 Jul 20;272(3):239–240. doi: 10.1001/jama.272.3.239. [DOI] [PubMed] [Google Scholar]
- Tarlov A. R. HMO enrollment growth and physicians: the third compartment. Health Aff (Millwood) 1986 Spring;5(1):23–35. doi: 10.1377/hlthaff.5.1.23. [DOI] [PubMed] [Google Scholar]
- Traxler H. Physician supply modelling in the United States of America and its uses in assisting policy making. World Health Stat Q. 1994;47(3-4):118–125. [PubMed] [Google Scholar]
- Weiner J. P. Forecasting the effects of health reform on US physician workforce requirement. Evidence from HMO staffing patterns. JAMA. 1994 Jul 20;272(3):222–230. [PubMed] [Google Scholar]
- Wennberg J. E., Goodman D. C., Nease R. F., Keller R. B. Finding equilibrium in U.S. physician supply. Health Aff (Millwood) 1993 Summer;12(2):89–103. doi: 10.1377/hlthaff.12.2.89. [DOI] [PubMed] [Google Scholar]
- Whitcomb M. E. A cross-national comparison of generalist physician workforce data. Evidence for US supply adequacy. JAMA. 1995 Sep 6;274(9):692–695. [PubMed] [Google Scholar]
- Ylitalo K., Jama L., Raatikainen P., Peuhkurinen K. Adaptation to myocardial ischemia during repeated dynamic exercise in relation to findings at cardiac catheterization. Am Heart J. 1996 Apr;131(4):689–697. doi: 10.1016/s0002-8703(96)90272-0. [DOI] [PubMed] [Google Scholar]