

Abstract
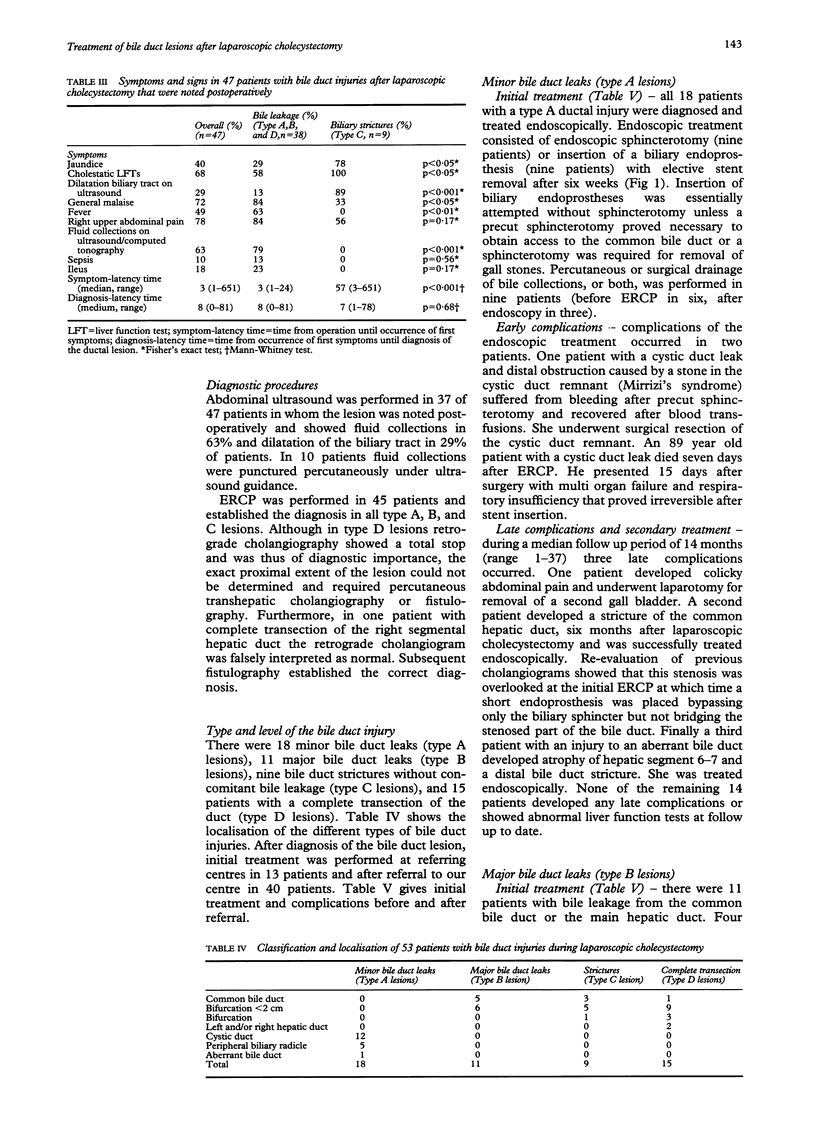
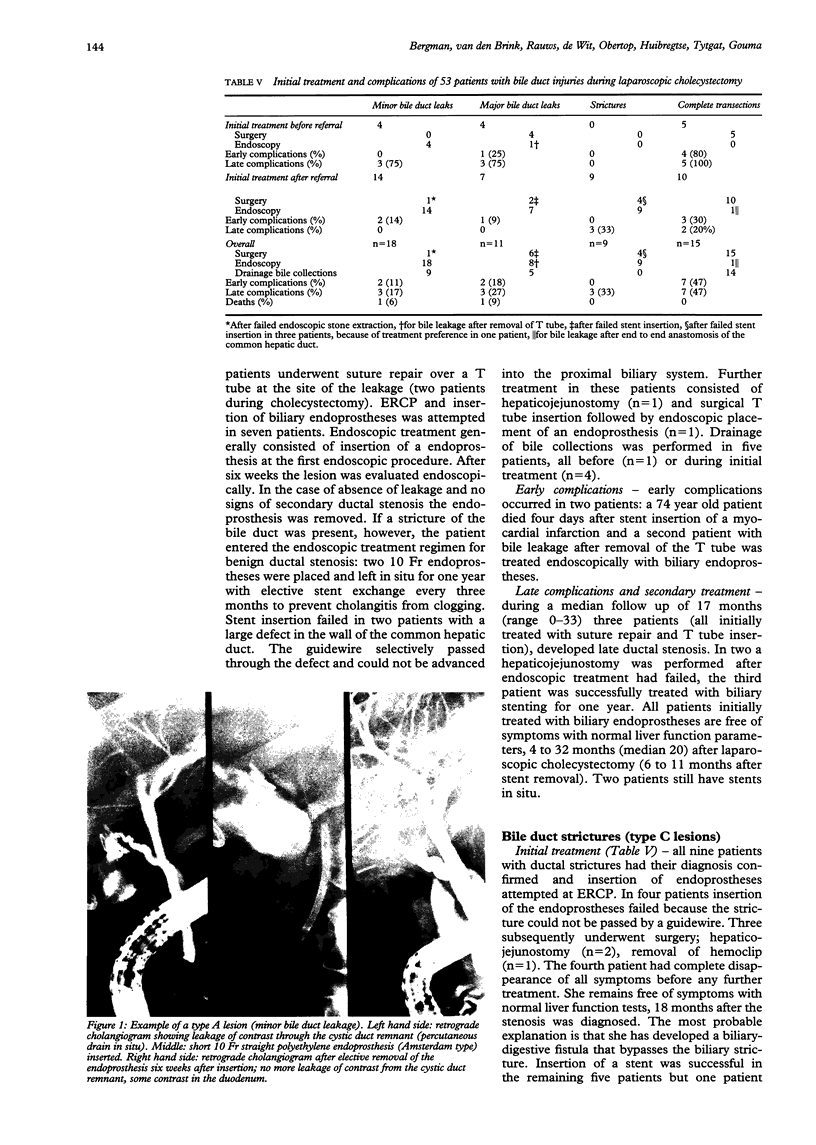
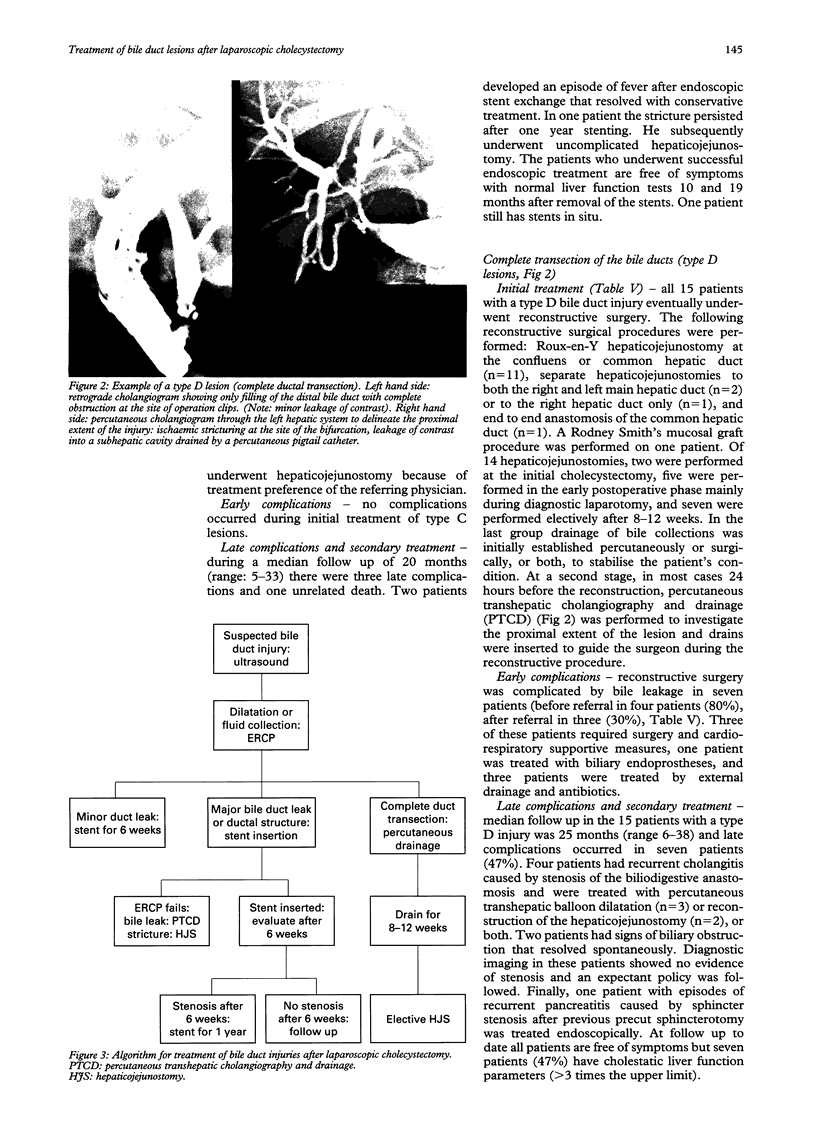
From January 1990 to June 1994, 53 patients who sustained bile duct injuries during laparoscopic cholecystectomy were treated at the Amsterdam Academic Medical Centre. There were 16 men and 37 women with a mean age of 47 years. Follow up was established in all patients for a median of 17 months. Four types of ductal injury were identified. Type A (18 patients) had leakage from cystic ducts or peripheral hepatic radicles, type B (11 patients) had major bile duct leakage, type C (nine patients) had an isolated ductal stricture, and type D (15 patients) had complete transection of the bile duct. Endoscopic retrograde cholangiopancreatography (ERCP) established the diagnosis in all type A, B, and C lesions. In type D lesions percutaneous cholangiography was required to delineate the proximal extent of the injury. Initial treatment (until resolution of symptoms and discharge from hospital) comprised endoscopy in 36 patients and surgery in 26 patients. Endoscopic treatment was possible and successful in 16 of 18 of type A lesions, five of seven of type B lesions, and three of nine of type C lesions. Most failures resulted from inability to pass strictures or leaks at the initial endoscopy. During initial treatment additional surgery was required in seven patients. Fourteen patients underwent percutaneous or surgical drainage of bile collections, or both. After endoscopic treatment early complications occurred in three patients, with a fatal outcome in two (not related to the endoscopic therapy). During follow up six patients developed late complications. All 15 patients with complete transection and four patients with major bile duct leakage were initially treated surgically. During initial treatment additional endoscopy was required in two patients. Early complications occurred in eight patients. During follow up seven patients developed stenosis of the anastomosis or bile duct. Reconstructive surgery in the early postoperative phase was associated with more complications than elective reconstructive surgery. Most type A and B bile duct injuries after laparoscopic cholecystectomy (80%) can be treated endoscopically. In patients with more severe ductal injury (type C and D) reconstructive surgery is eventually required in 70%. Multidisciplinary approach to these lesions is advocated and algorithms for treatment are proposed.
Full text
PDF


Images in this article
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Adams D. B., Borowicz M. R., Wootton F. T., 3rd, Cunningham J. T. Bile duct complications after laparoscopic cholecystectomy. Surg Endosc. 1993 Mar-Apr;7(2):79–83. doi: 10.1007/BF00704382. [DOI] [PubMed] [Google Scholar]
- Branum G., Schmitt C., Baillie J., Suhocki P., Baker M., Davidoff A., Branch S., Chari R., Cucchiaro G., Murray E. Management of major biliary complications after laparoscopic cholecystectomy. Ann Surg. 1993 May;217(5):532–541. doi: 10.1097/00000658-199305010-00014. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cotton P. B., Lehman G., Vennes J., Geenen J. E., Russell R. C., Meyers W. C., Liguory C., Nickl N. Endoscopic sphincterotomy complications and their management: an attempt at consensus. Gastrointest Endosc. 1991 May-Jun;37(3):383–393. doi: 10.1016/s0016-5107(91)70740-2. [DOI] [PubMed] [Google Scholar]
- Cuschieri A., Dubois F., Mouiel J., Mouret P., Becker H., Buess G., Trede M., Troidl H. The European experience with laparoscopic cholecystectomy. Am J Surg. 1991 Mar;161(3):385–387. doi: 10.1016/0002-9610(91)90603-b. [DOI] [PubMed] [Google Scholar]
- Davidoff A. M., Pappas T. N., Murray E. A., Hilleren D. J., Johnson R. D., Baker M. E., Newman G. E., Cotton P. B., Meyers W. C. Mechanisms of major biliary injury during laparoscopic cholecystectomy. Ann Surg. 1992 Mar;215(3):196–202. doi: 10.1097/00000658-199203000-00002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Davids P. H., Ringers J., Rauws E. A., de Wit L. T., Huibregtse K., van der Heyde M. N., Tytgat G. N. Bile duct injury after laparoscopic cholecystectomy: the value of endoscopic retrograde cholangiopancreatography. Gut. 1993 Sep;34(9):1250–1254. doi: 10.1136/gut.34.9.1250. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Davids P. H., Tanka A. K., Rauws E. A., van Gulik T. M., van Leeuwen D. J., de Wit L. T., Verbeek P. C., Huibregtse K., van der Heyde M. N., Tytgat G. N. Benign biliary strictures. Surgery or endoscopy? Ann Surg. 1993 Mar;217(3):237–243. doi: 10.1097/00000658-199303000-00004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Go P. M., Schol F., Gouma D. J. Laparoscopic cholecystectomy in The Netherlands. Br J Surg. 1993 Sep;80(9):1180–1183. doi: 10.1002/bjs.1800800938. [DOI] [PubMed] [Google Scholar]
- Gouma D. J., Go P. M. Bile duct injury during laparoscopic and conventional cholecystectomy. J Am Coll Surg. 1994 Mar;178(3):229–233. [PubMed] [Google Scholar]
- Hawes R. H., Cotton P. B., Vallon A. G. Follow-up 6 to 11 years after duodenoscopic sphincterotomy for stones in patients with prior cholecystectomy. Gastroenterology. 1990 Apr;98(4):1008–1012. doi: 10.1016/0016-5085(90)90026-w. [DOI] [PubMed] [Google Scholar]
- Kozarek R. A., Ball T. J., Patterson D. J., Brandabur J. J., Raltz S., Traverso L. W. Endoscopic treatment of biliary injury in the era of laparoscopic cholecystectomy. Gastrointest Endosc. 1994 Jan-Feb;40(1):10–16. doi: 10.1016/s0016-5107(94)70003-6. [DOI] [PubMed] [Google Scholar]
- Kozarek R. A., Traverso L. W. Endoscopic stent placement for cystic duct leak after laparoscopic cholecystectomy. Gastrointest Endosc. 1991 Jan-Feb;37(1):71–73. doi: 10.1016/s0016-5107(91)70628-7. [DOI] [PubMed] [Google Scholar]
- Kozarek R., Gannan R., Baerg R., Wagonfeld J., Ball T. Bile leak after laparoscopic cholecystectomy. Diagnostic and therapeutic application of endoscopic retrograde cholangiopancreatography. Arch Intern Med. 1992 May;152(5):1040–1043. doi: 10.1001/archinte.152.5.1040. [DOI] [PubMed] [Google Scholar]
- McMahon A. J., Russell I. T., Baxter J. N., Ross S., Anderson J. R., Morran C. G., Sunderland G., Galloway D., Ramsay G., O'Dwyer P. J. Laparoscopic versus minilaparotomy cholecystectomy: a randomised trial. Lancet. 1994 Jan 15;343(8890):135–138. doi: 10.1016/s0140-6736(94)90932-6. [DOI] [PubMed] [Google Scholar]
- Mueller P. R., Ferrucci J. T., Jr, Simeone J. F., Cronan J. J., Wittenberg J., Neff C. C., vanSonnenberg E. Detection and drainage of bilomas: special considerations. AJR Am J Roentgenol. 1983 Apr;140(4):715–720. doi: 10.2214/ajr.140.4.715. [DOI] [PubMed] [Google Scholar]
- Orlando R., 3rd, Russell J. C., Lynch J., Mattie A. Laparoscopic cholecystectomy. A statewide experience. The Connecticut Laparoscopic Cholecystectomy Registry. Arch Surg. 1993 May;128(5):494–499. doi: 10.1001/archsurg.1993.01420170024002. [DOI] [PubMed] [Google Scholar]
- Ress A. M., Sarr M. G., Nagorney D. M., Farnell M. B., Donohue J. H., McIlrath D. C. Spectrum and management of major complications of laparoscopic cholecystectomy. Am J Surg. 1993 Jun;165(6):655–662. doi: 10.1016/s0002-9610(05)80783-4. [DOI] [PubMed] [Google Scholar]
- Rosato E. F., Berkowitz H. D., Roberts B. Bile ascites. Surg Gynecol Obstet. 1970 Mar;130(3):494–496. [PubMed] [Google Scholar]
- Rossi R. L., Schirmer W. J., Braasch J. W., Sanders L. B., Munson J. L. Laparoscopic bile duct injuries. Risk factors, recognition, and repair. Arch Surg. 1992 May;127(5):596–602. doi: 10.1001/archsurg.1992.01420050124016. [DOI] [PubMed] [Google Scholar]
- Traverso L. W., Kozarek R. A., Ball T. J., Brandabur J. J., Hunter J. A., Jolly P. C., Patterson D. J., Ryan J. A., Thirlby R. C., Wechter D. G. Endoscopic retrograde cholangiopancreatography after laparoscopic cholecystectomy. Am J Surg. 1993 May;165(5):581–586. doi: 10.1016/s0002-9610(05)80439-8. [DOI] [PubMed] [Google Scholar]
- Trerotola S. O., Savader S. J., Lund G. B., Venbrux A. C., Sostre S., Lillemoe K. D., Cameron J. L., Osterman F. A., Jr Biliary tract complications following laparoscopic cholecystectomy: imaging and intervention. Radiology. 1992 Jul;184(1):195–200. doi: 10.1148/radiology.184.1.1535161. [DOI] [PubMed] [Google Scholar]
- Walker A. T., Brooks D. C., Tumeh S. S., Braver J. M. Bile duct disruption after laparoscopic cholecystectomy. Semin Ultrasound CT MR. 1993 Oct;14(5):346–355. doi: 10.1016/s0887-2171(05)80054-x. [DOI] [PubMed] [Google Scholar]
- Woods M. S., Traverso L. W., Kozarek R. A., Tsao J., Rossi R. L., Gough D., Donohue J. H. Characteristics of biliary tract complications during laparoscopic cholecystectomy: a multi-institutional study. Am J Surg. 1994 Jan;167(1):27–34. doi: 10.1016/0002-9610(94)90050-7. [DOI] [PubMed] [Google Scholar]
- vanSonnenberg E., Casola G., Wittich G. R., Christensen R., Varney R. R., Neff C. C., D'Agostino H. B., Moossa A. R. The role of interventional radiology for complications of cholecystectomy. Surgery. 1990 Jun;107(6):632–638. [PubMed] [Google Scholar]