

Abstract
Theoretical models suggest that both HIV knowledge and HIV risk perception inform rational decision-making and, thus, predict safer sex motivation and behavior. However, the amount of variance explained by knowledge and risk perception is typically small. In this cross-sectional study, we investigated whether the predictive power of HIV knowledge and HIV risk perception on safer sex motivation is affected by trait anger. We hypothesized that anger may disrupt rational-decision making, distorting the effects of both HIV knowledge and risk perception on safer sex intentions. Data from 232 low-income, urban women at risk for HIV infection were used to test a path model with past sexual risk behavior, HIV knowledge, and HIV risk perception as predictors of safer sex intentions. Moderator effects of anger on safer sex intentions were tested by simultaneous group comparisons between high-anger and low-anger women (median-split). The theoretically expected “rational pattern” was found among low-anger women only, including (a) a positive effect of knowledge on safer sex intentions, and (b) buffer (inhibitor) effects of HIV knowledge and HIV risk perception on the negative path leading from past risk behavior to safer sex intentions. Among high-anger women, an “irrational pattern” emerged, with no effects of HIV knowledge and negative effects of both past risk behavior and HIV risk perception on safer sex intentions. In sum, the results suggest that rational knowledge and risk-based decisions regarding safer sex may be limited to low-anger women.
Keywords: HIV, knowledge, anger, safer sex, intention, risk perception
Anger as a Moderator of Safer Sex Motivation among Low Income Urban Women
Interventions and public campaigns against the HIV epidemic are usually guided by theoretical models that specify the social-cognitive components likely to promote rational decision making and self-protective action. In empirical investigations theoretical models have been moderately successful in explaining safer sex behavior. For example, two meta-analyses (Albarracin, Johnson, Fishbein, & Muellerleile, 2001; Godin & Kok, 1996) indicate that, on average, 30 to 42% of the variance in condom use can be explained by current models of health behavior, including the Theory of Planned Behavior (Ajzen, 1991), and its precursor, the Theory of Reasoned Action (Fishbein & Ajzen, 1975). Despite this success, models of health behavior leave much variance unexplained. It is likely that further, previously neglected factors moderate the rational processes that are assumed to explain self-protective action.
One shortcoming in models of health behavior may be the disregard of negative emotions as a potential source of apparently irrational actions (Kalichman & Weinhardt, 2001). Focusing on rational decision making, such models help to explain why people adopt health behaviors but they often fail to explain why people engage in self-defeating risk behavior (Cho, Keller, & Cooper, 1999).In these theories, negative emotions are considered only as anticipated consequences (costs) of behavior in a cognitive evaluation process, in which costs are weighed against the benefits (e.g., Ajzen, 1991; Bagozzi, 1992; Becker, 1974; Fisher & Fisher, 1996).
Recently, negative emotions such as anger have been suspected to establish barriers to safer sex behavior beyond rational decision-making. Research testing the effects of negative affective states on sexual risk behavior has provided mixed results. In a recent meta-analysis, integrating 23 different studies and 34 samples, Crepaz and Marks (2001) concluded that there is little evidence for a reliable connection between negative affective states and sexual risk behavior. The average effect size found for anger did not exceed r̄ = .10. Heterogeneity was strong with correlations ranging from -.41 to .55. However, these results should be interpreted with caution. In a critique of Crepaz and Marks' meta-analysis, Kalichman and Weinhardt (2001) summarized some of the shortcomings of the studies, pointing, for example, to the limitations of cross-sectional results linking measures of negative affect to retrospective reports of sexual risk behavior. Further, rather than showing direct effects on behavior, negative affect may interact with other factors in influencing risk behavior. For example, the effects of anger may be limited to specifically stressed populations (Kalichman, 1999; Kalichman, Greenberg, & Abel, 1997; Kelly et al., 1993; Nyamathi, Wayment, & Dunkel-Schetter, 1993). In sum, it would be premature to accept the results of Crepaz and Marks' meta-analysis as conclusive.
In light of these considerations, we investigated the role of anger in sexual risk taking and safer sex motivation. Based on an existing data set assessing sexual risk behavior among low-income urban women, we addressed an important but understudied topic, namely,moderator effects of anger on safer sex intentions. Previous research indicates that induced mood might affect the relationship between social-cognitive predictors and intentions to use condoms (Armitage, Conner, & Mark, 1999). Accordingly, we hypothesized that anger would interfere with rational decision-making and disrupt the link between rational insight and safer sex motivation.
Testing moderator effects of anger on safer sex motivation required the definition of “rational” and “irrational” patterns in the relationships between theoretical predictors and safer sex intentions. Therefore, in the following section, we discuss briefly theoretical predictor variables that are most likely to indicate irrational tendencies and, thus, appear most promising in testing moderator effects of anger.
Indicators of Irrational Decision Making: The Role of Knowledge and Perceived Risk
Various theoretical models suggest that health related cognitions involving HIV knowledge and/or HIV risk perception are needed to inform rational decision-making and self-protective action. Among them are the Health Belief Model (Becker, 1974), the Information—Motivation—Behavioral skills model (Fisher & Fisher, 1992, 1996), the AIDS Risk Reduction Model (Catania, Coates, & Kegeles, 1994), the Precaution Adoption Process Model (Weinstein, 1988), Protection Motivation Theory (Rogers & Prentice-Dunn, 1997), and the Health Action Process Approach (Schwarzer, 2002). These models imply that rational decision-making, based on information and/or risk awareness, is a key to the adoption of health behavior. However, studies on HIV risk behavior indicate that both HIV knowledge and HIV risk perception lack predictive power, specifically compared to social-cognitive predictors of behavior such as outlined in the TPB (Ajzen, 1991). These results raise questions regarding the role of these health-related cognitions and, more generally, rational information processing in the prediction of safer sex.
Among the various models of health behaviors, only Weinstein's (1988) Precaution Adoption Process Model takes irrational tendencies as potential barriers against self-protective behavior into account. According to this model, information, experience, or knowledge about potential risks is necessary to increase risk awareness and perceived threat. However, knowledge about the risks does not suffice. Health threats must be perceived as personally relevant in order to motivate precautionary behavior. Accordingly, HIV-related knowledge should be a distal, and risk perception a proximal, predictor of safer sex intentions. In Weinstein's model, irrational thinking may emerge in the form of an optimistic bias, which manifests in the belief that health risks may apply to other people but not to oneself. That is, if risk perception is averted by an optimistic bias, knowledge about risks may not translate into safer sex intentions.
Although the optimistic bias describes only one potential mechanism of apparently irrational behavior, its role in Weinstein's model may point to a general “weakness” of both knowledge and risk perception in the prediction of safer sex intentions. That is, the impact of knowledge and risk perceptions on intentions and health behavior may be prone to disruptions by irrational thinking. This might explain why HIV knowledge and risk perception are less successful in predicting condom use and safer sex intentions than more general predictors of behavior such as attitudes, perceived social norms, and perceived behavioral control, as outlined in the TPB (Ajzen, 1991). Several recent meta-analysis provide evidence for the different predictive power displayed by variables of the TPB compared to health related cognitions including HIV knowledge and risk perception. In a recent meta-analysis focusing on predictors of the TPB, Albarracin et al. (2001) reported strong effect sizes for attitudes, social norm, and perceived behavioral control on safer sex intentions (r = .58, .39., and .45) and future behavior (r = .38, .25, and .25, respectively). Similarly, in a meta-analysis on predictors of safer sex intention, Sheeran and Taylor (1999) reported effect sizes of r= .45 for attitudes, .42 for subjective norms, and .35 for self-efficacy beliefs, but found only weak to moderate effect sizes of .21 for HIV knowledge and .14 for indicators of perceived risk. The same patterns emerged in yet another meta-analysis of Sheeran, Abraham, and Orbell (1999) on predictors of condom use. For TPB variables, effect sizes (weighted average correlations) varied between .25 and .32, whereas the effect sizes of HIV knowledge and risk perception approached zero.
One problem in interpreting this pattern of results is the overwhelming number of cross-sectional investigations that do not focus on behaviorchange but just on the prediction of behavior, often assessed in retrospect (Albarracin et al., 2001; Sheeran et al., 1999; Sheeran & Taylor, 1999). The strong effect sizes reported for attitudes, norms, and perceived behavior control can be assumed to reflect, in part, the impact of past behavior and habits; they are likely to fit into an apparently rational correlational pattern that, in fact, links past behavior and habits with intentions and future behavior (see, for example, Albarracin et al., 2001). The same cannot be assumed for knowledge and risk perception, which are common predictors in HIV risk reduction models. Within these models, knowledge and risk perception work as “catalysts” in the adoption of safer sex. Although both knowledge and risk perception may be, in part, affected by past engagement in sexual risk behavior, theoretical models still assume that they will correlate positively with safer sex intentions, and negatively with future risk behavior. However, in non-experimental, correlational investigations, it seems unlikely that these presumed “catalyst” effects of knowledge and risk perceptions on behavior change can be observed.
In sum, both knowledge and risk perception have been outlined in the literature as important factors in a rational decision-making process that involves the adoption of typically non-hedonistic, rational, health-promoting behavior. Both may be affected by past risk behavior but, in contrast to social-cognitive predictors as outlined in the TPB, their effects are more difficult to predict. They are likely to induce cognitive dissonance and, potentially, behavior change, and they are less likely to predict the perseverance of past behavioral tendencies in high-risk individuals.
Further, the effects of HIV knowledge and risk perception are presumed to be a result of rational insight in one's risks (Weinstein, 1988). Thus, they are most likely to be distorted by irrational tendencies caused by negative emotions such as anger. Rational insight and risk awareness may support safer sex intentions among low-anger women only but may fail to enhance safer sex motivation among high-anger women.
The Present Study
The present study sought to (a) examine the effects of anger on sexual risk taking and safer sex intentions, and (b) test moderator effects of anger on the relationship between past behavior, HIV risk awareness, HIV knowledge, and safer sex intentions. With regard to the moderator effects of anger, we hypothesized that low-anger individuals would be more likely than high-anger individuals to display a rational pattern. A rational pattern would be indicated by (a) a positive correlation between knowledge and safer sex intentions, (b) a positive correlation between past risk behavior and current risk awareness, and (c) “inhibitor” effect of risk awareness and HIV knowledge on the typically negative correlation between past risk behavior and safer sex intentions. Further, we hypothesized that low-anger individuals would be more inclined to take objective risks into account when evaluating their personal risks. However, the primary criteria for the identification of rational and irrational patterns were the effects of both HIV knowledge and HIV risk perception on safer sex intentions.
Method
Research Setting and Participants
The sample consisted of women who were screened for a randomized HIV prevention trial (Carey et al., 2000). Inclusion criteria for the present analyses included sexual activity status (any vaginal intercourse during the past 3 months), age (between 16 and 45 years), relationship status (single or divorced), and childbearing status (not pregnant and no births in the past 6 months).
Participants' (n = 232) mean age was 30 years (range 16-50,SD=7.6); 88% were African American, 7% European American, and 5% of other ethnic origin. The average income level was low with 95% reporting a monthly income lower than $1,200. Most of the women had at least one child (82%). The mean level of education was 11.6 years (range 6-17,SD=1.6). The women were either single (90%) or divorced (10%). Most women (78%) had been tested for HIV, and 2 (1%) reported being HIV positive (see Table 1).
Table 1.
Sample Characteristics (n = 232)
| low | anger | high | anger | t | p | |
|---|---|---|---|---|---|---|
| M |
SD |
M |
SD |
|||
| Age (range 16-50) | 30.1 | 7.4 | 29.1 | 7.8 | 1.03 | ns |
| Years of education (range 6-17) | 11.9 | 1.7 | 11.2 | 1.4 | 3.62 | .001 |
| N |
% |
N |
% |
Chi2 |
p |
|
| Monthly Income | ||||||
| $ 0 - 399 | 34 | 29.8 | 47 | 42.0 | 7.33 | ns |
| $ 400-599 | 37 | 32.5 | 39 | 34.8 | ||
| $ 600-799 | 22 | 19.3 | 14 | 12.5 | ||
| $ 800-1199 | 12 | 10.5 | 9 | 8.0 | ||
| $ >=1200 | 9 | 7.9 | 3 | 2.7 | ||
| Employed | ||||||
| No | 85 | 72.6 | 82 | 71.9 | 7.29 | .027 |
| Yes- Part-Time (1-30 hrs) | 17 | 14.5 | 27 | 23.7 | ||
| Yes- Full-Time | 15 | 12.8 | 5 | 4.4 | ||
| Ethnicity | ||||||
| African American | 201 | 87.8 | 102 | 88.7 | 3.07 | ns |
| White | 14 | 12.2 | 13 | 11.3 | ||
| Marital status | ||||||
| Single | 106 | 90.6 | 103 | 89.6 | 0.07 | ns |
| Divorced | 11 | 9.4 | 12 | 10.4 | ||
| Number of children | ||||||
| None | 16 | 13.7 | 27 | 11.6 | 3.80 | ns |
| 1-2 | 53 | 45.3 | 44 | 38.3 | ||
| 3-4 | 36 | 30.8 | 33 | 28.7 | ||
| > 4 | 12 | 10.3 | 11 | 9.6 | ||
| Living with partner | ||||||
| Yes | 47 | 40.9 | 34 | 31.2 | 2.88 | ns |
| No | 42 | 36.5 | 51 | 46.8 | ||
| Have no partner / spouse | 26 | 22.6 | 24 | 22.0 | ||
| Student | ||||||
| No | 85 | 73.3 | 88 | 77.2 | 0.57 | ns |
| Yes, high school or GED | 18 | 15.5 | 14 | 12.3 | ||
| Yes, college | 13 | 11.2 | 12 | 10.5 | ||
| Know someone with HIV/AIDS | ||||||
| No | 45 | 38.5 | 34 | 29.6 | 2.04 | ns |
| Yes | 72 | 61.5 | 81 | 70.4 | ||
| Tested for HIV | ||||||
| No | 24 | 20.5 | 28 | 24.3 | 0.49 | ns |
| Yes | 93 | 79.5 | 87 | 75.7 | ||
| HIV Status | ||||||
| Negative | 90 | 79.6 | 78 | 69.6 | 4.33 | ns |
| Positive | 0 | 0 | 2 | 1.8 | ||
| Don't know | 23 | 20.4 | 32 | 28.6 |
Note: GED =General Equivalency Degree; HIV = human immunodeficiency virus; ns = not significant.
Measures
Participants completed a self-administered survey that measured demographics, personal predispositions (anger, perceived stress, partner dependency), HIV knowledge, safer sex intentions, and sexual risk behavior. To protect participant privacy and promote candid self-reporting, assessments were anonymous (traceable only by a personally generated identification code).
Anger
Anger was assessed with the 10-item state scale of the State-Trait Anger Inventory (STAI, Spielberger, Jacobs, Russel, &Crane, 1983). The STAI, a widely used and well-validated instrument, measured the intensity of angry feelings during the past two weeks. The STAI is assessing state and trait anger as well as anger expression. Data from normative samples indicate an excellent internal consistency of .93 (Spielberger et al., 1983). Typical items of the state anger scale are: “I felt furious,” “I felt like yelling at somebody,” “I felt like hitting someone.” Respondents rated their anger on four-point Likert scale fromnever (1) toa lot of the time (4). Cronbach's Alpha was .96 in the present sample.
HIV Knowledge
HIV knowledge was assessed with the brief 18-item HIV Knowledge Questionnaire (HIV-KQ-18; Carey & Schroder, 2002). This instrument was derived from a longer version, the HIV-KQ (Carey, Morrison-Beedy, & Johnson, 1997). Reliability and validity studies of the HIV-KQ indicated high internal consistency (a = .91), and stability over 1- (r = .83), 2- (r = .91), and 12-week (r = .90) intervals (Carey et al., 1997), as well as construct validity in treatment outcome analyses, expert-nonexpert comparison studies, and associations with related knowledge measures. Internal consistency and stability of the derived 18-item version have been adequate, witha ranging from .75 to .89, and with stability coefficients between .76 and .94 over 3- and 6-months intervals in three different samples. The correlations with the original 45-item version ranged between r = .93 and r = .97. Items address the acquisition of HIV (e.g., “A woman can get HIV if she has sex with a man”), protective factors (e.g., “A person can NOT get HIV if he or she is taking antibiotics”), preventive behavior (e.g., “There is a female condom that can help decrease a woman's chance of getting HIV”), and myths that may affect behavior and partner choice (e.g., “People who have been infected with HIV quickly show serious signs of being infected”). A percent knowledge score was computed from the number of correct responses. Cronbac's alpha was .78 in the present sample.
Past Sexual Risk Behavior
Four measures were used to assess sexual risk behavior. First, using open response formats, participants were asked to report retrospectively about the absolute frequencies of unprotected vaginal intercourse during the past three months; this time frame was used to optimize (a) the opportunity for sexual behavior to occur and (b) reliable assessment of inter-individual differences in sexual risk behavior. Second, participants were asked about the number of male sexual partners during the past three months. Third, participants were asked to report about the absolute frequencies of alcohol and drug use preceding sexual intercourse with two items, which were summed as an overall indicator of substance use before sex. Fourth, five items reflecting non-redundant indicators of HIV risk were used; these items referred to injection drug use of sexual partner(s), intercourse with bisexual or gay partners, the number of sexually transmitted diseases, the frequency of sex trading, and the frequency of the regular partner's sexual intercourse with other partners. All five items were dichotomized to indicate presence or absence of the respective risk factor, and then summed to indicate the number of risk factors accumulated during the past year (range = 0 to 5).
Risk Perception
HIV risk perception was assessed with two items referring to one's personal risk to acquire the HIV. The items were: “Based on your sexual behavior over the past year, how much do you think you are at risk for getting the AIDS virus?” “What is the chance that you will some day get AIDS?” Both items were presented with a 6-point response scale ranging from no risk at all (1) to extremely at risk (6). The average of both items was taken as indicator of overall perceived HIV risk.
Safer Sex Intention
A seven-item scale assessed readiness for safer sex using “I will” statements (e.g., “I will use a condom,” “I will do only safe sex behaviors”). Responses were assessed with 8-point scales ranging from definitely will not do (1) to definitely will do (8). The scale had been used previous research (Carey, Maisto et al., 1997), showing high internal consistencies. Cronbach's alpha was .90 in the present sample.
Data Preparation
Because of skewness of the behavioral count data, computing Pearson correlations required data transformations to approximate a normal distribution. The frequency of unprotected vaginal intercourse and the frequency of drug and alcohol use before sex were transformed by log10 (x + 1). The number of male sexual partners was square root transformed. The transformed scores were tested for extreme outliers, using z > 3.21 (p < .001) as criterion. The log-transformed variables required a single outlier reduction each.
For the path analysis on sexual risk behavior, the frequency of substance use before sex was recoded into a categorical scale. Both drug use and alcohol use before sex were dichotomized and summed, leading to a 3-category scale (0 = never, 1 = alcohol or drug use before sex, 2 = both alcohol and drug use before sex. This was done to test the effects of single and multiple substance use on sexual risk behavior with an indicator that did not yield a frequency measure of sexual risk behavior itself. Similarly, the number of male partners was recoded into a 3-category scale (1 = monogamous during the past three month, 2 = had two partners, or 3 = more than 2 partners). Again, the rationale behind this transformation was to derive a predictor of non-monogamy that did not itself already yield a frequency measure of intercourse.
Data Analyses
Analyses were performed with SPSS 12.0, StataTM version 8, and LISREL 8.50. Pearson product-moment correlations were calculated using normalized scores of skewed behavioral measures. Regression analyses were performed in order to test the effects of anger controlling for perceived stress and partner dependency. Linear regressions were applied to normally distributed variables only; negative binomial regressions were applied to the untreated skewed behavioral outcomes, requesting robust estimates.
Model testing usually requires the application of structural equation modeling techniques. In order to test moderator effects of anger on the relationships between the social-cognitive predictors and safer sex intentions, dividing the sample into high- and low-anger women provided the most feasible approach (the alternative would require the inclusion of interaction terms, i.e., between anger and each of the cognitive predictors in the model, which would increase the likelihood of multicollinearity). For the path analyses, women were divided into two groups, based on a median split of the STAI. Matrices of polychoric and polyserial correlations were prepared by PRELIS2, separately for high-anger and low-anger women, using normalized scores of the skewed behavioral measures. Path analyses were performed with maximum likelihood estimates.
In a first step, a starting model was specified for the whole sample. In order to perform a stringent test on the role of HIV knowledge and risk perception, the development started with the specification of a mediator model, in which four indicators of past behavior (the frequency of unprotected intercourse, non-monogamous sexual relationships, substance use before sex, and the number of additional risk factors) were used as predictors, HIV knowledge and risk perception were specified as mediators, and safer sex intention served as the criterion. In addition, HIV knowledge was expected to contribute to HIV risk perception (see Figure 1). No a priori direct effects of past behavior on safer sex intentions were specified. Non-significant paths were removed and direct paths were freed if indicated to improve the fit to an acceptable level.
Figure 1.

Starting model for the model development in the full sample.
In a second step the model developed in the full sample was tested via simultaneous group comparisons, setting all parameters invariant. Subsequent simultaneous group comparisons tested for significant differences in single path coefficients; single structural paths were freed for separate estimation in the two groups, based on (a) theoretical relevance and (b) modification indices. Differences were determined as significant using the Δχ2 criterion. The difference in the χ2 statistic of two nested models assumes again a χ2 distribution, which can be tested for significance with Δdf(i.e., the number of parameters that are fixed in the nested comparison model only). Finally, a liberal model was tested, freeing all structural (beta and gamma) paths for separate estimation in the two groups. The χ2 of this model provided a lower limit to which the model improvement achieved with the theoretical model adjustments could be compared. Based on this most liberal model, a percentage improvement in fit due to the acceptance of the hypothesized group differences only was computed (i.e., [Δχ2maximum - Δχ2hypotheses] / Δχ2maximum *100).
Consistent with the use ofa priori hypotheses, the results are reported with one-sided significance levels.
Results
Table 2 presents descriptive statistics andt-test comparisons for high- and low-anger women as well as correlations between anger and the diverse indicators and predictors of sexual risk behavior. Anger was significantly related to unprotected intercourse during the past 3 months (r = .15,p < .05 / .01), alcohol and drug use before sex (r>= .31,p < .0001), the number of sexual partners during the past 3 months (r= .30,p < .0001), and the number of additional HIV risk factors (r = .31,p < .0001). Further, anger was positively related to HIV risk perception (r = .29,p < .0001), and negatively related to safer sex intentions (r= -.21,p < .002). The results did not indicate a stronger optimistic bias among high-anger women: They perceived themselves at higher risk than low-anger women and reported more risk behavior in the past, indicating an adequate evaluation of personal risk relative to the low-anger women.
Table 2.
Descriptive Statistics by Anger,t-tests, and Pearson Product-Moment Correlations with Anger
| Low anger |
High anger |
||||||
|---|---|---|---|---|---|---|---|
| Predictors (Range of Observed Scores) | M | SD | M | SD | t | p | r |
| Anger (10-40) | 17.0 | 2.7 | 28.0 | 5.1 | -20.4 | .001 | |
| Outcome Variables | |||||||
| Alcohol before sex (0-30)a | 1.7 | 3.9 | 4.3 | 6.8 | -4.14 | .001 | .31*** |
| Drug Use before sex (0-60)a | 1.3 | 4.1 | 4.1 | 8.0 | -4.77 | .001 | .30*** |
| Substance Use before sex (0-88)a | 3.0 | 7.3 | 8.2 | 12.9 | -5.13 | .001 | .34*** |
| Unprotected Vaginal Sex (0-270)a | 10.5 | 17.7 | 15.0 | 30.8 | -2.37 | .010 | .15* |
| Number of male partners (1-40)b | 1.4 | 1.6 | 2.8 | 4.9 | -3.78 | .001 | .30*** |
| Number of Risk Factors (0-5) | 0.5 | 0.8 | 1.0 | 1.2 | -4.21 | .001 | .31*** |
| HIV Risk Perception (1-4) | 1.8 | 0.8 | 2.4 | 1.1 | -4.57 | .001 | .29*** |
| HIV Knowledge (0-100%) | 73.2 | 18.6 | 74.5 | 19.3 | -0.55 | ns | .01 |
| Safer Sex Intentions (7-56) | 50.6 | 8.3 | 46.6 | 11.1 | 3.00 | .002 | -.21*** |
log10 (x+1) transformed scores were used for significance tests
square-root transformed scores were used for significance tests
p < .05
p < .01
p < .001
Further linear and negative binomial regressions were used to test unique effects of anger on past risk behavior and safer sex intentions, controlling for HIV knowledge and risk perception (not tabled). The regression coefficients for anger were significant in all analyses predicting safer sex intentions and past sexual risk behavior (p < .05). Anger contributed most strongly to the prediction of substance use before sex with B = .066,SE = .017,t = 3.85, and p < .001.
Subsequent analyses focused on moderator effects of anger on the relationships between past risk behaviors, knowledge, risk perceptions, and safer sex intentions. In a first step, a basic model was developed for the full sample, starting with the model outlined in Figure 1. The correlation matrix produced by PRELIS 2 for this analysis is shown in Table 3. The results are shown in Figure 2. Two direct negative paths from past risk behaviors (i.e., unprotected intercourse and number of sexual partners) on safer sex intentions were needed to improve the model fit to an acceptable level. Further, three non-significant paths were removed: Substance use before sex did not predict HIV risk perceptions, and HIV knowledge was unrelated to number of sexual partners and number of HIV risk factors but was predicted by substance use and unprotected intercourse only. This model had a good fit with χ2 = 4.50,df = 9,p=.88, Root Mean Square Error of Approximation (RSMEA) = .00, Root Mean Square Residual (RMR) = .016,Comparative Fit Index (CFI) = 1.00, Goodness of Fit (GFI) = .99, and an Adjusted GFI (AGFI) = .98. In this model, past risk behaviors were positively related to both HIV knowledge and risk perception; unprotected intercourse and number of partners displayed negative effects on safer sex intentions, and risk perception had negative effects on safer sex intentions as well. The only positive (but weak) predictor of safer sex intentions was HIV knowledge with a standardized path of .14 (t= 2.20,p < .05).
Table 3.
Matrix of Polychoric and Polyserial Correlations Produced by PRELIS-2, Full Sample
| 1. | 2. | 3. | 4. | 5. | 6. | 7. | M | SD | |
|---|---|---|---|---|---|---|---|---|---|
| 1. Substance Use before Sex | .79 | .84 | |||||||
| 2. Unprotected Vaginal Sex | .24 | .74 | .58 | ||||||
| 3. Number of Partners | .59 | .00 | 1.27 | .64 | |||||
| 4. Number of Risk Factors | .42 | .02 | .65 | .76 | 1.04 | ||||
| 5. HIV Knowledge | .23 | .16 | .14 | .04 | 73.67 | 18.99 | |||
| 6. HIV Risk Perception | .41 | .20 | .48 | .52 | .19 | 2.10 | 1.03 | ||
| 7. Safer Sex Intention | -.27 | -.19 | -.36 | -.23 | .03 | -.32 | 48.82 | 10.02 |
Figure 2.

Path model fitting the data in the full sample.
This model was used as the starting point for simultaneous group comparisons between high- and low-anger women. The correlation matrices produced by PRELIS-2 for this and all subsequent group comparisons are shown in Table 4. In a first group comparison, all parameters were set invariant between the groups. The results of the model were used as a standard of comparison for subsequent hypotheses-relevant model adjustments. The invariant model deviated significantly from the data base with χ2 = 58.65,df = 37,p=.01,RSMEA = .066,RMR = .089,CFI = .93,GFI = .93.
Table 4.
Matrix of Polychoric and Polyserial Correlations Produced by PRELIS-2, by Anger Group
| 1. | 2. | 3. | 4. | 5. | 6. | 7. | M | SD | |
|---|---|---|---|---|---|---|---|---|---|
| 1. Substance Use before Sex | .20 | .53 | .48 | .15 | .30 | -.28 | 1.06 | .86 | |
| 2. Unprotected Vaginal Sex | .18 | -.06 | -.01 | .22 | .16 | -.24 | .83 | .56 | |
| 3. Number of Partners | .54 | -.07 | .68 | .11 | .37 | -.36 | 1.42 | .80 | |
| 4. Number of Risk Factors | .14 | -.01 | .49 | -.02 | .46 | -.30 | 1.03 | 1.16 | |
| 5. HIV Knowledge | .35 | .09 | .20 | .13 | .20 | -.09 | 74.58 | 19.48 | |
| 6. HIV Risk Perception | .37 | .12 | .54 | .50 | .19 | -.45 | 2.39 | 1.14 | |
| 7. Safer Sex Intention |
-.13 |
-.07 |
-.04 |
-.01 |
.22 |
.01 |
47.00 |
11.19 |
|
| M | .53 | .65 | 1.12 | .49 | 72.76 | 1.81 | 50.62 | ||
| SD | .74 | .59 | .82 | .82 | 18.54 | .82 | 8.37 |
Note: Lower diagonal: Low- anger group (anger = 0); upper diagonal: High-anger group (anger=1)
In subsequent steps, single paths were set free for separate estimation in the two groups, guided by (a) the study hypotheses, and (b) the modification indices provided by LISREL8.3. First, the beta path leading from risk perception to intentions was set free for separate estimation. This led to a significant improvement in model fit with Δχ2 = 14.96, Δdf = 1, p < .0001. Second, the beta path leading from HIV knowledge on intentions was set free for separate estimation in the two groups. Again, a significant improvement in model fit was observed in comparison to the previous step with δχ2 = 3.11, Δdf = 1, p < .05. Third, the path leading from number of sexual partners to risk perception was set free for separate estimation, leading to a significant improvement in fit of Δχ2 = 4.37, δdf = 1, p < .025. No furtherv hypotheses-relevant differences between the two groups were detected. The results of the model tests are summarized in Table 5. The fit of the third model adjustment was satisfying with χ2 = 36.21, df = 34, p=.37, RSMEA = .017, RMR = .059, CFI = .99, and GFI = .96 (see TMM-3 in Table 5). This model is displayed in Figure 3, focusing on the three significant path differences only. First, and most importantly, risk perception displayed negative effects on safer sex intention in the high-anger group only but was nonsignificant in the low-anger group. Second, HIV knowledge displayed positive effects on safer sex intentions in the low-anger group only but was non-significant in the high-anger group. Finally, the number of sexual partners in the past three months affected risk perceptions in the low-anger group only but was non-significant among high-anger women.
Table 5.
Summary of Simultaneous Group Comparisons via LISREL
| Model | χ2 | df | p | RMSEA | GFI | RMR | CFI | Δχ2 | Δdf | p(Δχ2) | Δχ2cum | df | pcum |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1. Base Model: All Model Parameter Invariant | 58.65 | 37 | .01 | .066 | .93 | .089 | .93 | ||||||
| 1.1 TMM-1: β risk perception on intention free | 43.69 | 36 | .18 | .038 | .95 | .061 | .98 | 14.96 | 1 | <.0001 | |||
| 1.2 TMM-2: β knowledge on intention free | 40.58 | 35 | .24 | .032 | .95 | .054 | .98 | 3.11 | 1 | <.05 | 18.07 | 2 | .0001 |
| 1.3 TMM-3: γ No. of partners on risk perception free |
36.21 |
34 |
.37 |
.017 |
.96 |
.059 |
.99 |
4.37 |
1 |
<.025 |
22.44 |
3 |
.0001 |
| 2. Comparison Model: AllStructural Paths (γ, β) free | 28.62 | 27 | .38 | .012 | .97 | .050 | 1.00 | 7.59 | 7 | n. s. | |||
| 3. Final model (TMM-3, sign. paths only, two φ free) | 25.82 | 35 | .87 | .000 | .97 | .056 | 1.00 |
Note: TMM = Theoretical Model Modification;RMSEA = Root Mean Square Error of Approximation;CFI = Comparative Fit Index;RMR = Root Mean Square Residual;GFI = Goodness of Fit Index;AGFI = Adjusted Goodness of Fit Index; %χ2 = % contribution of the high-anger group to the χ2 statistic; Δχ2 = Chi Square difference to the final model in the low-anger group;Δdf = degrees of freedom for Δχ2.
Figure 3.

Simultaneous group comparison between high- and low-anger women, highlighting the hypotheses-relevant paths set free for separate estimation in the two groups.
In order to determine the degree of improvement obtained by freeing these three paths only, a comparison model was tested in which all structural paths (gammas and betas) were set free for separate estimation between the groups. This model had a good fit with χ2 = 28.62,df = 27,p=.38,RSMEA = .012, RMR = .050,CFI = 1.00, and GFI = .93. However, compared to the model with three paths freed only, the improvement in fit was non-significant with Δχ2 = 7.59 and Δdf = 7. Further, the model provided a measure of Δχ2maximum that could be achieved by freeing all structural paths for separate estimation in comparison to the invariant model. Using this Δχ2maximum of 58.65 — 28.62 = 30.03, the percentage improvement obtained by freeing the three paths only (risk perception → intention, HIV knowledge → intention, no. of partners → risk perception) was determined as 75%.
A final model was developed, removing in each group the paths that were identified as non-significant. Further, two elements of the variance-covariance matrix of the four predictors (Φ) were set free for separate estimation, as there were differences between the groups in the correlations between number of risk factors and substance use before sex, and between the number of risk factors and the number of partners. These modifications improved the fit without affecting the prior results (see Table 5 and Figure 4). The results of this model are shown in Figure 4. The path of number of partners on safer sex intentions was non-significant in the low-anger group and could be removed.
Figure 4.
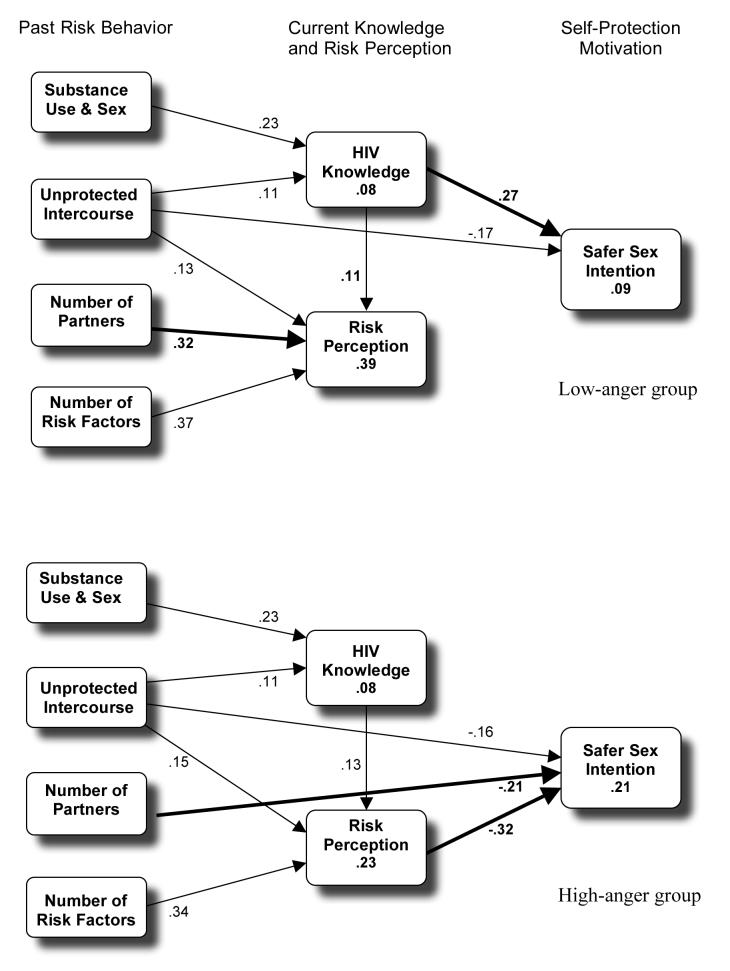
Final results: Path model fitting the data in both groups, with non-significant paths removed.
Overall, the results indicate that, in the high-anger group, safer sex intentions were predicted directly or indirectly by past engagement in risk behavior only (Figure 4a). In contrast, in the low-anger group, past risk behavior affected risk perception but displayed little effect on safer sex intentions. HIV risk knowledge appeared as the strongest predictor with positive effects on safer sex intentions. A single direct negative path from unprotected intercourse on intentions of -.17 was counteracted by an indirect effect of unprotected intercourse, mediated by HIV knowledge, of .03. Thus, in the low-anger group, the totaleffect of past unprotected intercourse on intentions was only -.14 (i.e., -.17 + [.11 * .27]) No further negative paths of past behavior on intentions were found within this group.
Discussion
The purpose of the current study was to extend the predictive utility of social-cognitive models of HIV risk behavior by testing the effects of anger on sexual risk behavior and its predictors, and by analyzing potential moderator effects of anger on safer sex intentions. In general, the role of negative emotion on risk behavior is not well understood, though many previous studies indicate an effect of negative mood such as depression and anger on risk behavior such as binge eating, substance use, and drunk-driving (e.g., Smith, 1992; Stice, Presnell, & Spangler, 2002) as well as health outcomes (e.g., Deffenbacher, Lynch, Filetti, Dahlen, & Oetting, 2003; Smith, 1992). The extant literature on the link between anger and sexual risk behavior is both inconclusive (Crepaz & Marks, 2001) and insufficient regarding more subtle, population-limited, and moderating effects of anger on safer sex behavior (Kalichman & Weinhardt, 2001). Our research adds to the literature on the predictive utility of anger and is, to our knowledge, the first study investigating moderator effects of anger in the theory-based modeling of safer sex intentions.
The results obtained with this sample of low-income urban women at risk for HIV were informative. Bivariate correlations between anger and sexual risk behaviors suggest that high-anger women are more likely to engage in sex with multiple partners, unprotected intercourse, and substance use before sex. These results add to the literature on anger and sexual risk taking. Contrary to Crepaz and Marks (Crepaz & Marks, 2001) who concluded that negative affect and sexual risk behavior are unrelated, we found that anger does correlate with more risky behavior. The coefficients exceed the average correlations reported by Crepaz and Marks, and support the conclusion that further research on the role of anger in sexual risk taking may lead to new insights in potential moderators of HIV risk behavior (Kalichman & Weinhardt, 2001).
Of specific interest for this study were moderator effects of anger on the relationships between past risk behavior, HIV knowledge, HIV risk perceptions and safer sex intentions, which have not been examined previously. A rational pattern, as outlined by models of health behavior change, was expected among low-anger women only. Moderator effects were tested by path analyses, based on a model with three assumptions: (a) past engagement in sexual risk behaviors has the tendency to persevere and display negative effects on safer sex intentions; (b) both HIV knowledge and risk perceptions are affected by prior engagement in risk behavior; and (c) rational information processing and rational decision-making imply that both HIV knowledge and personal risk perception should eliminate or lessen the effects of past behavior on future-oriented safer sex intentions, and potentially display positive effects on intentions. The pattern outlined in (c) was tested for moderator effects of anger, with the expectation that it may apply to low-anger women only. Further, we tested the hypothesis that past risk behavior might affect risk perception primarily among low-anger women, but may be disrupted by an optimistic bias among high-anger women.
The results of the simultaneous group comparisons support the moderator hypothesis. A model fitting the sample as a whole was used, but setting all parameters to be invariant between the high- and low anger groups did not fit the data. The results suggested freeing the two most important hypotheses-relevant paths leading from both HIV risk perceptions and HIV knowledge to safer sex intentions. The change in the path coefficient indicated a rational pattern among low-anger women only: Past behavior had strong effects on HIV risk perceptions, which seemed to block most of the effects of past engagement in risk behaviors on intentions. HIV knowledge was affected by past behavior as well but displayed positive effects on intentions. In sum, past risk behavior displayed little effect on safer sex intentions, whereas knowledge improved safer sex motivation.
In contrast, in the high-anger group, an apparently irrational pattern appeared. Although past engagement in risk behavior was positively related to both risk perception and HIV knowledge, both risk knowledge and risk awareness did not prevent or lessen the negative effects of past risk behavior and habits on safer sex intentions. HIV knowledge was unrelated to intentions and risk perception was a strong negative predictor of intentions, findings contradicting theoretical models assuming that rational insight in one's risks should promote self-protection motivation (Fisher & Fisher, 1996; Rogers & Prentice-Dunn, 1997; Weinstein, 1988).
Additional group comparisons provided further support for the expected rational pattern in the low-anger group and the irrational pattern hypothesized for the high-anger group. The missing path between number of partners and risk perception among high-anger women suggests that they ignore or negate the fact that having sex with multiple partners increases their risk of HIV contraction. Instead, sex with multiple partners displayed a direct negative effect on safer sex intention. Assuming that high-anger women are as competent as low-anger women in evaluating objective risks, it seems likely that high-anger women who engage in high-risk behavior cope with cognitive dissonance by ignoring the risks involved in multiple sexual relationships. Among low-anger women, the opposite pattern appeared: Multiple partners in the past predicted risk perception but displayed neither direct nor indirect effects on safer sex intention, indicating that risk perception successfully disrupted the tendency to continue with past risk behavior.
In sum, the results of the present study add to the current discussion of emotions in rational decision-making and indicate that further research on moderator effects of anger is needed. Models of health behavior change rely heavily on rational insight and may not apply if rational thinking and self-management are undermined by negative emotions. To date, models of health behavior integrate emotions as part of the cost-benefit analysis only (see, for example, (Bryan, Aiken, & West, 1997). However, recent research and discussions indicate that behavior does not necessarily follow a rational pattern (Cho et al., 1999) and that negative emotions may have an impact beyond rational decision-making (Kalichman & Weinhardt, 2001; Lerner & Keltner, 2000, 2001). Particularly interesting are results of Lerner and Keltner (2000), 2001) indicating that anger (in contrast to fear) may elicit optimistic risk appraisals, thus reducing motivation to adopt health-protective behaviors (Weinstein, 1988; Weinstein & Klein, 1996). The present study supports these findings, indicating that high-anger women tend to ignore past risk behavior in evaluating their risk of HIV infection.
The present study seems to have further important implications. First, as long as theoretical models do not include negative affect and other irrational tendencies, their success in guiding health behavior interventions will likely be attenuated. Interestingly, several recent HIV/AIDS intervention trials integrated an anger management intervention as a treatment-control condition (Hovell et al., 2001; St. Lawrence, Crosby, Belcher, Yazdani, & Brasfield, 1999), implying that anger management may have independent effects on HIV risk reduction that should be controlled in order to evaluate the unique effects of an HIV-focused approach.
Second, the present study points to problems in cross-sectional model-testing research that are rarely discussed in the literature, despite the common critique of cross-sectional designs. Cross-sectional studies predicting safer sex intentions or retrospectively assessed risk behavior may find correlational patterns that do not seem to make sense, such as a negative impact of risk perceptions on safer sex intentions, or zero-correlations between HIV knowledge and safer sex (Sheeran et al., 1999; Sheeran & Taylor, 1999). We do not want to imply that cross-sectional data are useless in testing theoretical models. However, researchers should take into account that cross-sectional data may not provide correlational patterns exactly fitting the models developed for the prediction of behavior change. The impact of past behavior on the predictor measures is often overlooked, which appears particularly problematic if retrospectively assessed behavior is “predicted” by current knowledge, intentions, and risk perceptions. If models of health behavior change are tested in cross-sectional research, adaptations are necessary, taking into account that it is not behavior change that is predicted, but current behavioral tendencies and habits only.
Some limitations of the current study need to be mentioned. Our results may not generalize to other populations and health behaviors. The data set included women only, and the results may not be same in an equivalent sample of high-risk men. Further, the study was not initially designed to test the effects of anger, limiting the sample, measures, and analytic design to the data that were available in this data set. The study focused on a limited number of cognitive predictors only (i.e., feelings, and intentions of single participants), excluding other important cognitions (such as self-efficacy beliefs), and neglecting social influence, partner interaction, as well as environmental, cultural, and societal factors that might explain additional variance in sexual risk behavior. Given the multiple determinants of sexual behaviors, individual factors such as anger can explain only a limited part of the variance. Research needs to identify other important determinants of risk behavior.
Despite these limitations, the results of this study may stimulate the discussion of the assumptions, strategies, and modifications of HIV related model-testing research. Future studies should investigate more thoroughly the role of negative emotions as predictors and moderators of rational decision-making and treatment responsiveness.
References
- Ajzen I. The Theory of Planned Behavior. Organizational Behavior and Human Decision Processes. 1991;50:179–211. [Google Scholar]
- Albarracin D, Johnson BT, Fishbein M, Muellerleile PA. Theories of Reasoned Action and Planned Behavior as models of condom use: A meta-analysis. Psychological Bulletin. 2001;127:142–161. doi: 10.1037/0033-2909.127.1.142. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Armitage CJ, Conner M, Mark NP. Differential effects of mood on information processing: Evidence from the theories of reasoned action and planned behaviour. European Journal of Social Psychology. 1999;29(4):419–433. [Google Scholar]
- Bagozzi RP. The self-regulation of attitudes, intentions, and behavior. Social Psychology Quarterly Special Issue: Theoretical advances in social psychology. 1992;55(2):178–204. [Google Scholar]
- Becker HM. The Health Belief Model and personal health behavior. Slack; Thorofare, NJ: 1974. [Google Scholar]
- Bryan AD, Aiken LS, West SG. Young women's condom use: the influence of acceptance of sexuality, control over the sexual encounter, and perceived susceptibility to common STDs. Health Psychology. 1997;16(5):468–479. doi: 10.1037//0278-6133.16.5.468. [DOI] [PubMed] [Google Scholar]
- Carey MP, Maisto SA, Kalichman SC, Forsyth AD, Wright EM, Johnson BT. Enhancing motivation to reduce the risk of HIV infection for economically disadvantaged urban women. Journal of Consulting and Clinical Psychology. 1997;65(4):531–541. doi: 10.1037//0022-006x.65.4.531. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Carey MP, Morrison-Beedy D, Johnson BT. The HIV-Knowledge Questionnaire: development and evaluation of a reliable, valid, and practical self-administered questionnaire. AIDS and Behavior. 1997;1:61–74. [Google Scholar]
- Carey MP, Schroder KEE. Development and psychometric evaluation of the brief HIV Knowledge Questionnaire. AIDS Education and Prevention. 2002;14(2):172–182. doi: 10.1521/aeap.14.2.172.23902. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Catania JA, Coates TJ, Kegeles S. A test of the AIDS risk reduction model: Psychosocial correlates of condom use in the AMEN cohort survey. Health Psychology. 1994;13(6):548–555. doi: 10.1037//0278-6133.13.6.548. [DOI] [PubMed] [Google Scholar]
- Cho Y-H, Keller LR, Cooper ML. Applying decision-making approaches to health risk-taking behaviors: Progress and remaining challenges. Journal of Mathematical Psychology. 1999;43(2):261–285. doi: 10.1006/jmps.1999.1258. [DOI] [PubMed] [Google Scholar]
- Crepaz N, Marks G. Are negative affective states associated with HIV sexual risk behaviors? A meta-analytic review. Health Psychology. 2001;20(4):291–299. doi: 10.1037//0278-6133.20.4.291. [DOI] [PubMed] [Google Scholar]
- Deffenbacher JL, Lynch RS, Filetti LB, Dahlen ER, Oetting ER. Anger, aggression, risky behavior, and crash-related outcomes in three groups of drivers. Behavior Research and Therapy. 2003;41(3):333–349. doi: 10.1016/s0005-7967(02)00014-1. [DOI] [PubMed] [Google Scholar]
- Fishbein M, Ajzen I. Belief, attitude, intention and behavior: An introduction to theory and research. Addison-Wesley; Reading, Mass.: 1975. [Google Scholar]
- Fisher JD, Fisher WA. Changing AIDS-risk behavior. Psychological Bulletin. 1992;111(3):455–474. doi: 10.1037/0033-2909.111.3.455. [DOI] [PubMed] [Google Scholar]
- Fisher JD, Fisher WA. The Information-Motivation-Behavioral Skills Model of AIDS risk behavior change: Empirical support and application. In: Oskamp S, Thompson SC, editors. Understanding and preventing HIV risk behavior. Sage; Thousand Oaks: 1996. pp. 100–127. [Google Scholar]
- Godin G, Kok G. The Theory of Planned Behavior: A review of its applications to health-related behaviors. American Journal of Health Promotion. 1996;11(2):87–98. doi: 10.4278/0890-1171-11.2.87. [DOI] [PubMed] [Google Scholar]
- Hovell MF, Blumberg EJ, Liles S, Powell L, Morrison TC, Duran G, Sipan CL, Burkham S, Kelley N. Training AIDS and anger prevention social skills in at-risk adolescents. Journal of Counseling and Development. 2001;79(3):347–355. [Google Scholar]
- Kalichman SC. Psychological and social correlates of high-risk sexual behaviour among men and women living with HIV/AIDS. AIDS Care. 1999;11(4):415–428. doi: 10.1080/09540129947794. [DOI] [PubMed] [Google Scholar]
- Kalichman SC, Greenberg J, Abel G. Sexual compulsivity among HIV-positive men who engage in high-risk sexual behaviour with multiple partners: An exploratory study. AIDS Care. 1997;2:441–450. doi: 10.1080/09540129750124984. [DOI] [PubMed] [Google Scholar]
- Kalichman SC, Weinhardt L. Negative affect and sexual risk behavior. Comment on Crepaz and Marks (2001) Health Psychology. 2001;20(4):300–301. [PubMed] [Google Scholar]
- Kelly JA, Murphy DA, Bahr GR, Koob JJ, Morgan MG, Kalichman SC, Stevenson LY, Brasfield TL, Bernstein BM, St. Lawrence JS. Factors associated with severity of depression and high-risk sexual behavior among persons diagnosed with human immunodeficiency virus (HIV) infection. Health Psychology. 1993;12:215–219. doi: 10.1037//0278-6133.12.3.215. [DOI] [PubMed] [Google Scholar]
- Lerner JS, Keltner D. Beyond valence: Toward a model of emotion-specific influences on judgment and choice. Cognition and Emotion. 2000;14(4):473–493. [Google Scholar]
- Lerner JS, Keltner D. Fear, anger, and risk. Journal of Personality and Social Psychology. 2001;81(1):146–159. doi: 10.1037//0022-3514.81.1.146. [DOI] [PubMed] [Google Scholar]
- Nyamathi A, Waymenty HA, Dunkel-Schetter C. Psychosocial correlates of emotional distress and risk behavior in African-American women at risk for HIV infection. Anxiety, Stress, and Coping. 1993;6:133–148. [Google Scholar]
- Rogers RW, Prentice-Dunn S. Protection motivation theory. In: Gochman D, editor. Handbook of health behavior research: Vol. 1. Determinants of health behavior: Personal and social. Plenum; New York, NY: 1997. pp. 113–132. [Google Scholar]
- http://userpage.fu-berlin.de/~health/hapa.htm Modeling Health Behavior Change: The Health Action Process Approach (HAPA)
- Sheeran P, Abraham C, Orbell S. Psychosocial correlates of heterosexual condom use: A meta-analysis. Psychological Bulletin. 1999;125:90–132. doi: 10.1037/0033-2909.125.1.90. [DOI] [PubMed] [Google Scholar]
- Sheeran P, Taylor S. Predicting intentions to use condoms: A meta-analysis and comparison of the Theories of Reasoned Action and Planned Behavior. Journal of Applied Social Psychology. 1999;29:1624–1675. [Google Scholar]
- Smith TW. Hostility and health: Current status of a psychosomatic hypothesis. Health Psychology. 1992;11(3):139–150. doi: 10.1037//0278-6133.11.3.139. [DOI] [PubMed] [Google Scholar]
- St. Lawrence JS, Crosby RA, Belcher L, Yazdani N, Brasfield TL. Sexual risk reduction and anger management interventions for incarcerated male adolescents: A randomized controlled trial of two interventions. Journal of Sex Education and Therapy. 1999;24(12):9–17. [Google Scholar]
- Stice E, Presnell K, Spangler D. Risk factors for binge eating onset in adolescent girls: A 2-year prospective investigation. Health Psychology. 2002;21(2):131–138. [PubMed] [Google Scholar]
- Weinstein ND. The precaution adoption process. Health Psychology. 1988;7:355–386. doi: 10.1037//0278-6133.7.4.355. [DOI] [PubMed] [Google Scholar]
- Weinstein ND, Klein WM. Unrealistic optimism: Present and future. Journal of Social and Clinical Psychology. 1996;15:1–8. [Google Scholar]