

Abstract
1 Haemodynamic changes during the onset of the antihypertensive action of pindolol, 10 mg twice daily, and propranolol, 80 mg three times daily, were studied for 24 h in two groups of 10 patients with uncomplicated essential hypertension.
2 Baseline haemodynamics were not different between the two groups.
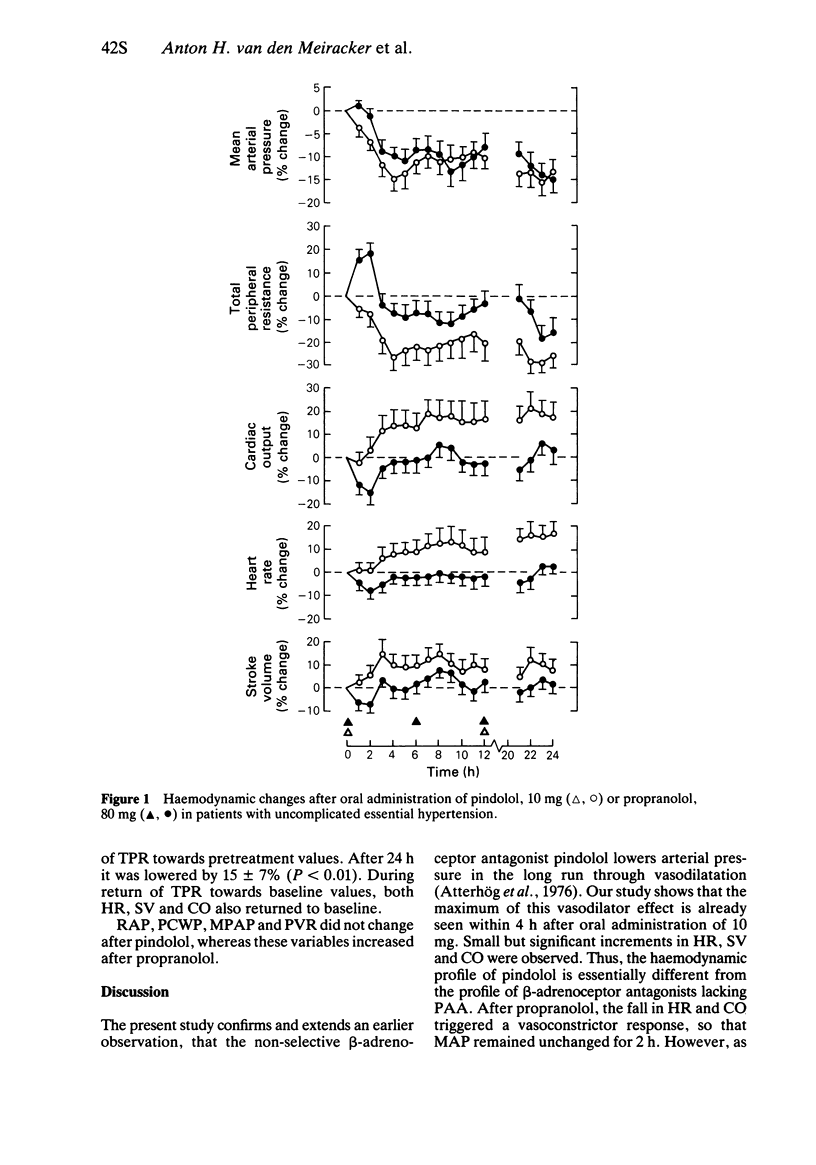
3 Pindolol, with considerable intrinsic sympathomimetic activity (ISA) exerted its maximal antihypertensive efficacy within 3-4 h after dosing (-15 ± 3%, mean ± s.e. mean, P < 0.001). This effect was maintained for 24 h.
4 After propranolol, which is devoid of ISA, arterial pressure fell more gradually, but after 24 h the two drugs shared an equal antihypertensive effect.
5 Cardiac output rose after pindolol by 16 ± 5% (P < 0.01). It decreased transiently by 16 ± 6% (P < 0.01) 1-4 h after propranolol. At that time vascular resistance had risen by 18 ± 5% (P < 0.001).
6 The onset of the antihypertensive action of the two drugs was associated with reductions in vascular resistance. Since reflex vasoconstriction did not occur after pindolol, vascular resistance was always lower on this drug than on propranolol (-29 ± 4%, P < 0.001 vs -15 ± 5%, P < 0.01).
7 Cardiac filling pressures, pulmonary artery pressure and pulmonary vascular resistance did not change after pindolol but they rose after propranolol.
8 During the onset of the vasodilator and antihypertensive effects of the two β-adrenoceptor blockers heart rate, stroke volume and cardiac output rose, despite cardiac β-adrenoceptor blockade, suggesting a reduction of parasympathetic tone and an increase in venous return.
9 Thus, haemodynamic changes after administration of β-adrenoceptor blockers are much more complex, than would be expected from their ancillary properties and the effects of cardiac β-adrenoceptor blockade.
Keywords: β-adrenoceptor blockers, cardiac output, vascular resistance, hypertension, pindolol, propranolol
Full text
PDF
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Anavekar S. N., Louis W. J., Morgan T. O., Doyle A. E., Johnston C. I. The relationship of plasma levels of pindolol in hypertensive patients to effects on blood pressure, plasma renin and plasma noradrenaline levels. Clin Exp Pharmacol Physiol. 1975 May-Jun;2(3):203–212. doi: 10.1111/j.1440-1681.1975.tb03026.x. [DOI] [PubMed] [Google Scholar]
- Atterhög J. H., Dunér H., Pernow B. Experience with pindolol, a betareceptor blocker, in the treatment of hypertension. Am J Med. 1976 May 31;60(6):872–876. doi: 10.1016/0002-9343(76)90907-4. [DOI] [PubMed] [Google Scholar]
- Bevan A. T., Honour A. J., Stott F. H. Direct arterial pressure recording in unrestricted man. Clin Sci. 1969 Apr;36(2):329–344. [PubMed] [Google Scholar]
- Colfer H. T., Cottier C., Sanchez R., Julius S. Role of cardiac factors in the initial hypotensive action by beta-adrenoreceptor blocking agents. Hypertension. 1984 Mar-Apr;6(2 Pt 1):145–151. [PubMed] [Google Scholar]
- Man in 't Veld A. J., Schalekamp M. A. Effects of 10 different beta-adrenoceptor antagonists on hemodynamics, plasma renin activity, and plasma norepinephrine in hypertension: the key role of vascular resistance changes in relation to partial agonist activity. J Cardiovasc Pharmacol. 1983;5 (Suppl 1):S30–S45. doi: 10.1097/00005344-198300051-00006. [DOI] [PubMed] [Google Scholar]
- Man in 't Veld A. J., Schalekamp M. A. Haemodynamic consequences of intrinsic sympathomimetic activity and cardioselectivity in beta-blocker therapy for hypertension. Eur Heart J. 1983 Jul;4 (Suppl 500):31–41. doi: 10.1093/eurheartj/4.suppl_d.31. [DOI] [PubMed] [Google Scholar]
- Man in 't Veld A. J., Schalekamp M. A. How intrinsic sympathomimetic activity modulates the haemodynamic responses to beta-adrenoceptor antagonists. A clue to the nature of their antihypertensive mechanism. Br J Clin Pharmacol. 1982;13(Suppl 2):245S–257S. doi: 10.1111/j.1365-2125.1982.tb01922.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Simon G., Franciosa J. A., Gimenez H. J., Cohn J. N. Short-term systemic hemodynamic adaptation to beta-adrenergic inhibition with atenolol in hypertensive patients. Hypertension. 1981 Mar-Apr;3(2):262–268. doi: 10.1161/01.hyp.3.2.262. [DOI] [PubMed] [Google Scholar]
- Svendsen T. L., Hartling O., Trap-Jensen J. Immediate haemodynamic effects of propranolol, practolol, pindolol, atenolol and ICI 89,406 in healthy volunteers. Eur J Clin Pharmacol. 1979 May 21;15(4):223–228. doi: 10.1007/BF00618509. [DOI] [PubMed] [Google Scholar]
- Tarazi R. C., Dustan H. P. Beta adrenergic blockade in hypertension. Practical and theoretical implications of long-term hemodynamic variations. Am J Cardiol. 1972 May;29(5):633–640. doi: 10.1016/0002-9149(72)90164-6. [DOI] [PubMed] [Google Scholar]