

Abstract
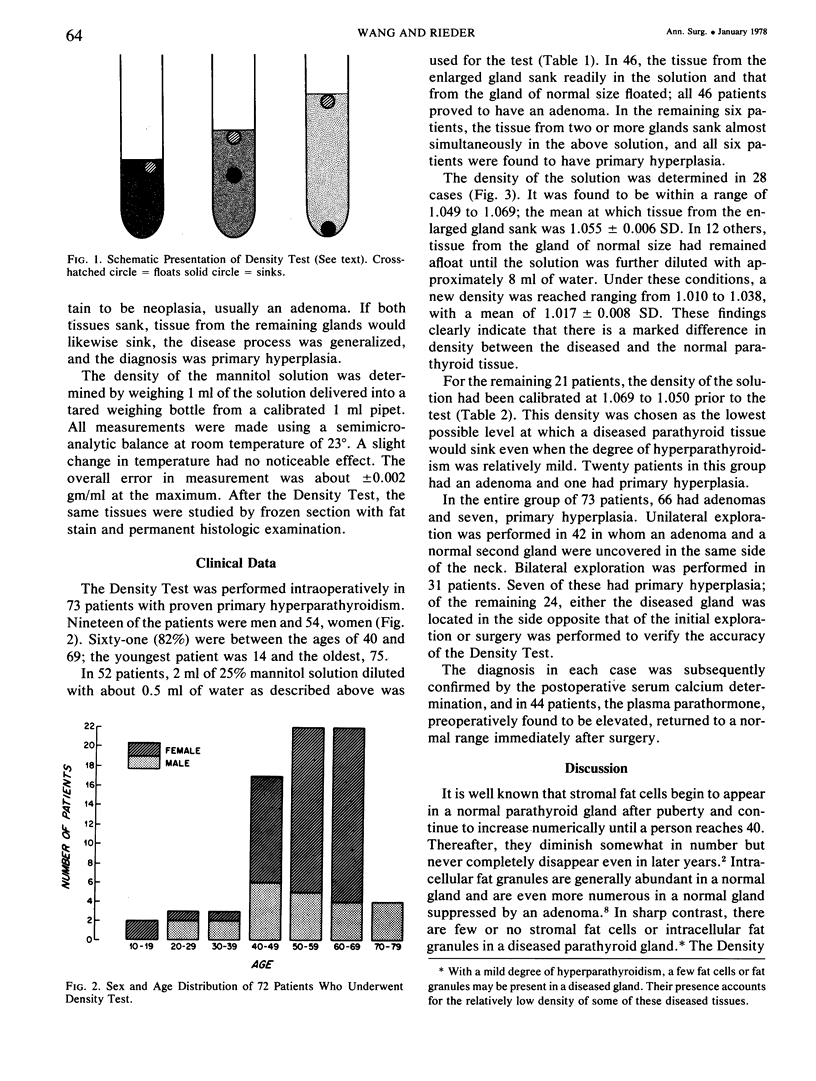
A simple, instant, and reliable test called the Density Test, based on the difference in density between the normal and the diseased parathyroid tissue, was performed intraoperatively in 73 patients with primary hyperparathyroidism. Whereas the normal parathyroid tissue floated, the diseased tissue invariably sank in a mannitol solution with a density range between 1.049 and 1.069. With the aid of this test, a diagnosis of adenoma was made in 66 patients and of primary hyperplasia in the remaining seven. In every case the diagnosis was subsequently confirmed. Forty-two of the 66 patients with an adenoma (64%) had a unilateral exploration of the neck. The Density Test saved these patients from an unnecessary contralateral exploration by the finding of an adenoma and a normal second gland in the same side of the neck. These data show that the Density Test is useful in the intraoperative diagnosis of a diseased from a normal parathyroid tissue. Tissue that sinks within the density range of 1.049 and 1.069 is without exception diseased and should therefore be either partially or completely excised even if the gland is of average size or only of slight enlargement. If it does not sink, it is virtually certain to be normal and should be spared. The Density Test provides a valuable clue in the differentiation of primary parathyroid hyperplasia from neoplasia.
Full text
PDF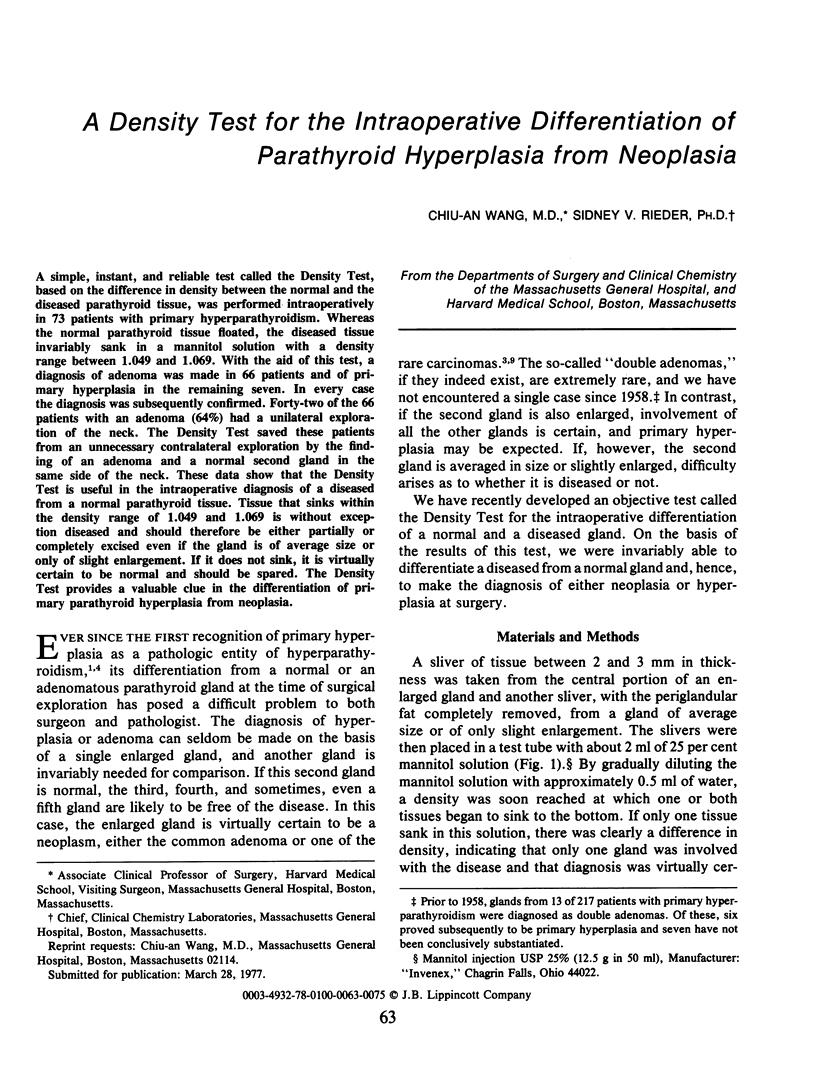



Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Castleman B., Mallory T. B. The Pathology of the Parathyroid Gland in Hyperparathyroidism: A Study of 25 Cases. Am J Pathol. 1935 Jan;11(1):1–72.17. [PMC free article] [PubMed] [Google Scholar]
- Cope O. The study of hyperparathyroidism at the Massachusetts General Hospital. N Engl J Med. 1966 May 26;274(21):1174–1182. doi: 10.1056/NEJM196605262742105. [DOI] [PubMed] [Google Scholar]
- Esselstyn C. B., Jr, Levin H. S., Eversman J. J., Schumacher O. P., Skillern P. G. Reappraisal of parathyroid pathology in hyperparathyroidism. Surg Clin North Am. 1974 Apr;54(2):443–447. doi: 10.1016/s0039-6109(16)40290-2. [DOI] [PubMed] [Google Scholar]
- Haff R. C., Ballinger W. F. Causes of recurrent hypercalcemia after parathyroidectomy for primary hyperparathyroidism. Ann Surg. 1971 Jun;173(6):884–891. doi: 10.1097/00000658-197106010-00005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Paloyan E., Lawrence A. M., Baker W. H., Straus F. H., 2nd Near-total parathyroidectomy. Surg Clin North Am. 1969 Feb;49(1):43–48. doi: 10.1016/s0039-6109(16)38733-3. [DOI] [PubMed] [Google Scholar]
- Roth S. I., Gallagher M. J. The rapid identification of "normal" parathyroid glands by the presence of intracellular fat. Am J Pathol. 1976 Sep;84(3):521–528. [PMC free article] [PubMed] [Google Scholar]