

Abstract
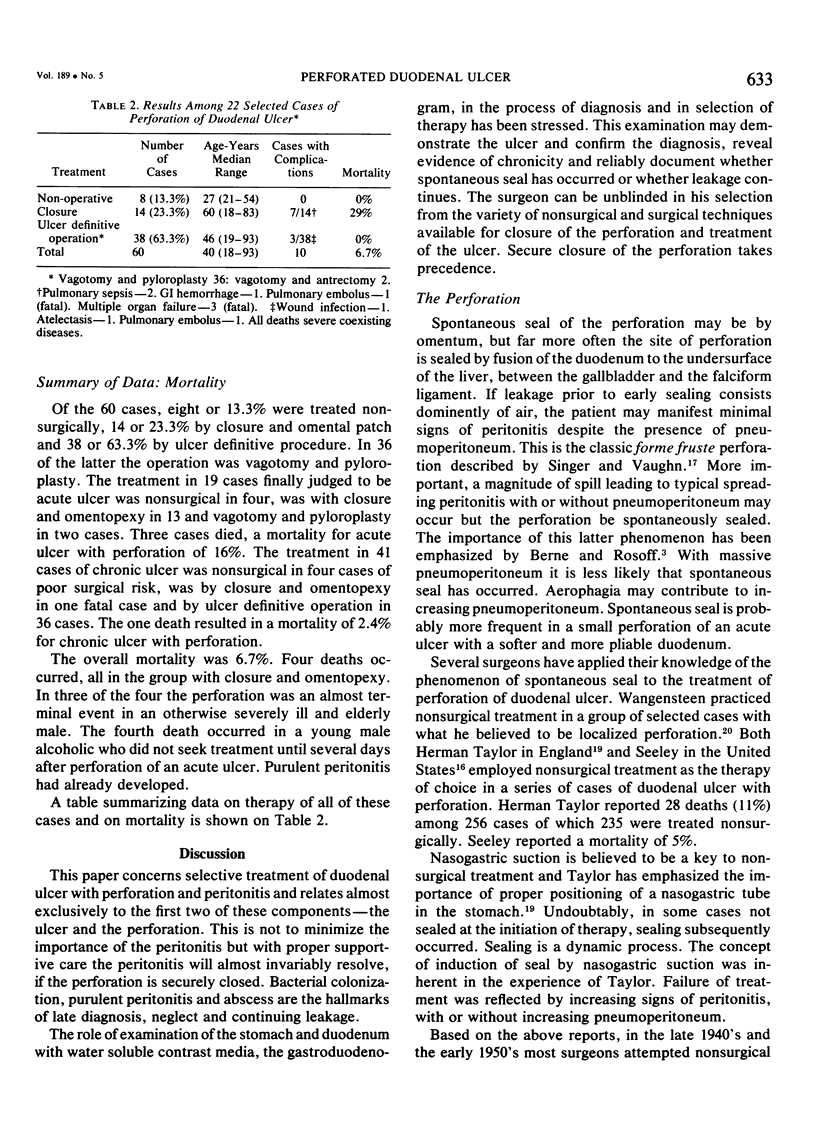
Selective treatment of duodenal ulcer with perforation has been based on several premises: 1) The natural history of the ulcer following closure of a perforation is generally favorable with an acute and unfavorable with a chronic ulcer. 2) An upper gastrointestinal series with water soluble contrast media can reliably document a spontaneously sealed perforation. 3) With a spontaneous seal, nonsurgical therapy is an acceptable option and is preferable for an acute ulcer or a chronic ulcer with poor surgical risk. 4) The treatment of choice for an unsealed perforation of an acute ulcer is simple surgical closure. 5) The treatment of choice of perforation of a chronic ulcer with acceptable surgical risk is an ulcer definitive operation. Sixty cases of perforation of duodenal ulcer have been treated. Nonsurgical therapy was employed without complication in eight cases with radiologically documented spontaneous seal. Truncal vagotomy and pyloroplasty in 36 cases and truncal vagotomy and antrectomy in two cases were each without mortality. Four fatalities occurred among 13 cases of closure and omental patch, each a case with severe associated disease. The mortality was 6.7% among the 60 cases; 2.4% for chronic ulcer and 16% for acute ulcer.
Full text
PDF
Images in this article
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- AMERSON J. R., HOWARD J. M., VOWLES K. D. The amylase concentration in serum and peritoneal fluid following acute perforation of gastroduodenal ulcers. Ann Surg. 1958 Feb;147(2):245–250. doi: 10.1097/00000658-195802000-00015. [DOI] [PMC free article] [PubMed] [Google Scholar]
- BERNE C. J., MIKKELSEN W. P. Management of perforated peptic ulcer. Surgery. 1958 Sep;44(3):591–603. [PubMed] [Google Scholar]
- Illingworth C. F., Scott L. D., Jamieson R. A. Progress after Perforated Peptic Ulcer. Br Med J. 1946 May 25;1(4455):787–790. [PMC free article] [PubMed] [Google Scholar]
- Jarrett F., Donaldson G. A. The ulcer diathesis in perforated duodenal ulcer disease. Experience with 252 patients during a twenty-five year period. Am J Surg. 1972 Apr;123(4):406–410. doi: 10.1016/0002-9610(72)90191-2. [DOI] [PubMed] [Google Scholar]
- Jordan G. L., Jr, DeBakey M. E., Duncan J. M., Jr Surgical management of perforated peptic ulcer. Ann Surg. 1974 May;179(5):628–633. doi: 10.1097/00000658-197405000-00015. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jordan P. H., Jr, Hendenstedt S., Korompai F. L., Lundquist G. Vagotomy of the fundic gland area of the stomach without drainage. A definitive treatment for perforated duodenal ulcer. Am J Surg. 1976 May;131(5):523–526. doi: 10.1016/0002-9610(76)90002-7. [DOI] [PubMed] [Google Scholar]
- Jordan P. H., Jr, Korompai F. L. Evolvement of a new treatment for perforated duodenal ulcer. Surg Gynecol Obstet. 1976 Mar;142(3):391–395. [PubMed] [Google Scholar]
- PIERANDOZZI J. S., HINSHAW D. B., STAFFORD C. E. Vagotomy and pyloroplasty for acute perforated duodenal ulcer. A report of seventy-five cases. Am J Surg. 1960 Aug;100:245–250. doi: 10.1016/0002-9610(60)90297-x. [DOI] [PubMed] [Google Scholar]
- Paster S. B., Brogdon B. G. Roentgenographic diagnosis of pneumoperitoneum. JAMA. 1976 Mar 22;235(12):1264–1267. [PubMed] [Google Scholar]
- SEELEY S. F., CAMPBELL D. Nonoperative treatment of perforated peptic ulcer; a further report. Surg Gynecol Obstet. 1956 May;102(5):435–446. [PubMed] [Google Scholar]
- Sawyers J. L., Herrington J. L., Jr Perforated duodenal ulcer managed by proximal gastric vagotomy and suture plication. Ann Surg. 1977 Jun;185(6):656–660. doi: 10.1097/00000658-197706000-00007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sisel R. J., Donovan A. J., Yellin A. E. Experimental fecal peritonitis. Influence of barium sulfate or water-soluble radiographic contrast material on survival. Arch Surg. 1972 Jun;104(6):765–768. doi: 10.1001/archsurg.1972.04180060015003. [DOI] [PubMed] [Google Scholar]
- TAYLOR H. Guest lecture: the nonsurgical treatment of perforated peptic ulcer. Gastroenterology. 1957 Sep;33(3):353–368. [PubMed] [Google Scholar]