

Abstract
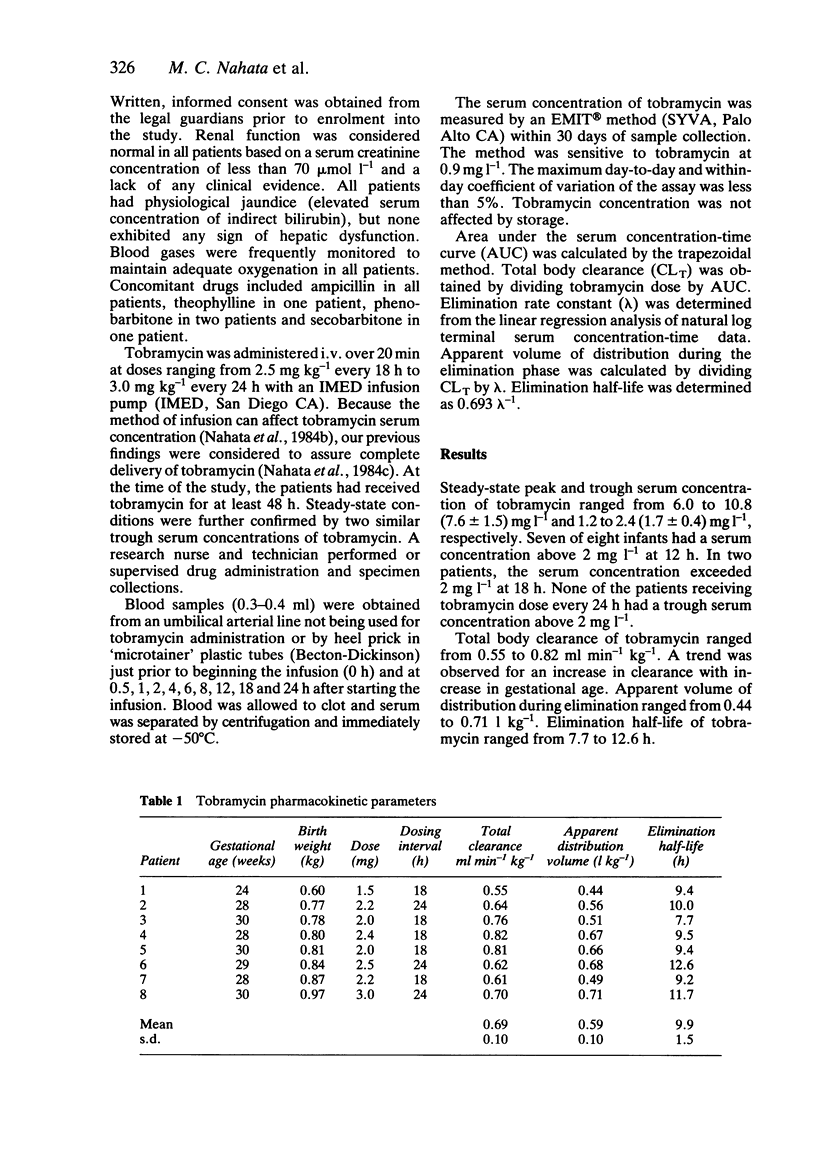
Tobramycin is commonly used at a dose of 2.5 mg kg-1 12h-1, but this regimen often results in trough serum concentrations exceeding 2 mg l-1. Because of limited data in infants weighing less than 1,000 g at birth, we studied eight newborn infants (gestational age 24-30 weeks; postnatal age 3 X 4 days; birth weight 0.60-0.97 kg) at a modified dosing regimen of 2.5 mg kg-1 18 h-1 or 3.0 mg kg-1 24 h-1. Tobramycin peak and trough serum concentrations ranged from 6.0-10.8 (7.8 +/- 1.5) mg l-1 and 1.2-2.4 (1.7 +/- 0.4) mg l-1, respectively. Serum concentration exceeded 2 mg l-1 in seven of eight patients at 12 h and two of eight at 18 h; none had a trough serum concentration above 2 mg l-1 at 24 h. Total body clearance ranged from 0.55 to 0.82 (0.69 +/- 0.10) ml min-1 kg-1; apparent volume of distribution ranged from 0.44 to 0.71 (0.59 +/- 0.10) 1 kg-1; and elimination half-life ranged from 7.7 to 12.6 (9.9 +/- 1.5) h. These data indicate that the modified dosage regimen of 2.5 mg kg-1 18 h-1 or 3.0 mg kg-1 24 h-1 appears to be more acceptable than the current regimen in achieving effective and safe peak and trough serum concentration of tobramycin in newborn infants weighing less than 1 kg at birth.
Full text
PDF
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Arant B. S., Jr Developmental patterns of renal functional maturation compared in the human neonate. J Pediatr. 1978 May;92(5):705–712. doi: 10.1016/s0022-3476(78)80133-4. [DOI] [PubMed] [Google Scholar]
- Dahlgren J. G., Anderson E. T., Hewitt W. L. Gentamicin blood levels: a guide to nephrotoxicity. Antimicrob Agents Chemother. 1975 Jul;8(1):58–62. doi: 10.1128/aac.8.1.58. [DOI] [PMC free article] [PubMed] [Google Scholar]
- McCormick M. C. The contribution of low birth weight to infant mortality and childhood morbidity. N Engl J Med. 1985 Jan 10;312(2):82–90. doi: 10.1056/NEJM198501103120204. [DOI] [PubMed] [Google Scholar]
- Nahata M. C., Powell D. A., Durrell D. E., Miller M. A., Glazer J. P. Effect of infusion methods on tobramycin serum concentrations in newborn infants. J Pediatr. 1984 Jan;104(1):136–138. doi: 10.1016/s0022-3476(84)80612-5. [DOI] [PubMed] [Google Scholar]
- Nahata M. C., Powell D. A., Durrell D. E., Miller M. C., Glazer J. P. Effect of gestational age and birth weight on tobramycin kinetics in newborn infants. J Antimicrob Chemother. 1984 Jul;14(1):59–65. doi: 10.1093/jac/14.1.59. [DOI] [PubMed] [Google Scholar]
- Nahata M. C., Powell D. A., Durrell D., Glazer J. P. Delivery of tobramycin by three infusion systems. Chemotherapy. 1984;30(2):84–87. doi: 10.1159/000238251. [DOI] [PubMed] [Google Scholar]