

Abstract
Childhood sexual abuse (CSA) has been proposed to influence both women’s adult sexual risk behaviors and the quality of their intimate relationships. Among a household sample of women (n = 732), good fit was obtained for a model in which CSA predicted Wave 1 male partner sexual risk and aggression characteristics, resulting in lower relationship satisfaction, and ultimately in higher numbers of Wave 2 sexual partners. The model was generally replicated among women who entered new relationships at Waves 2 and 3. Partner sexual risk characteristics also were associated with women’s risk of sexually transmitted infection from current partner. Elevated sexual risk behaviors among CSA survivors reflect difficulty in establishing stable and safe relationships and may be reduced by interventions aimed at improving intimate relationships.
Keywords: childhood sexual abuse, sexual risk taking, relationship satisfaction, sexually transmitted diseases, sexual partners
Childhood sexual abuse (CSA) has been associated with a variety of risky sexual behaviors and indicators of sexual risk taking in adulthood, including multiple sexual partners and higher incidence of sexually transmitted infection (STI; see Heiman & Heard-Davison, 2004; Koenig & Clark, 2004, for reviews). CSA also has been associated with difficulties in adult interpersonal relationships, including involvement in intimate partner relationships marked by low satisfaction and high levels of conflict and violence (see Davis & Petretic-Jackson, 2000; DiLillo, 2001; Rumstein-McKean & Hunsley, 2001, for reviews). These two CSA sequelae—relationship difficulties and sexual risk taking—are likely to be linked. For example, women who desire a relationship while having difficulty forming lasting and satisfying partnerships are likely to have many short-term sexual relationships (Davis & Petretic-Jackson, 2000). Consequently, having “more sexual partnerships may say more about a woman’s relationship choices than [about] her sexual choices” (Heiman & Heard-Davison, 2004, p. 40). Despite the potential connection between relationship choices and sexual risk taking among CSA survivors, these outcomes typically have not been considered together. The current study attempted to bridge this gap by examining how a woman’s CSA experiences may shape the quality of her intimate partner relationships and ultimately her sexual risk.
CSA is commonly viewed as a traumatic experience, although no single symptom occurs universally among victims nor is there a single traumatizing process (Kendall-Tackett, Williams, & Finkelhor, 1993). Although several theoretical models have been proposed to explain survivor responses to CSA, Finkelhor and Browne’s (1985) model of traumagenic dynamics seems particularly relevant to understanding the interpersonal difficulties frequently reported among CSA survivors. According to this model, sexually abused children are rewarded for sexual behavior with attention and affection. This may contribute to the precocious sexual activity frequently observed among children and adolescents who have experienced CSA (see Beitchman, Zucker, Hood, DaCosta, & Akman, 1991; Kendall-Tackett et al., 1993, for reviews). According to Davis and Petretic-Jackson (2000), these patterns may continue into adulthood. For example, adult survivors tend to oversexualize relationships, feeling that they are obligated to provide sex or that sex can gain them affection. Further, the relationships of survivors may become sexual more quickly. CSA survivors typically report having more sexual partners compared with nonabused women (Cohen et al., 2000; National Institute of Mental Health Multisite HIV Prevention Trial, 2001; Parillo, Freeman, Collier, & Young, 2001).
Another of the traumagenic dynamics described by Finkelhor and Browne (1985) is betrayal, resulting in children feeling unable to trust adults, who they had expected to protect them. When these children reach adulthood, their sense of betrayal resulting from CSA may result in poor judgment about whom one can trust or lead to “a desperate search for a redeeming relationship” (Finkelhor & Browne, 1985, p. 535), resulting in a series of intense but short-lasting sexual relationships (Briere, 2004). CSA survivors have more difficulties in their adult relationships, reporting insecure attachment, lower levels of sexual and relationship satisfaction, and more marital dissolution (see DiLillo & Long, 1999; Rumstein-McKean & Hunsley, 2001, for reviews). As survivors leave their troubled relationships, they form new relationships, resulting in a series of short-term intimate partnerships. The higher numbers of sexual partners frequently reported by CSA survivors, typically viewed as indicative of women’s sexual risk taking, may alternatively be viewed as a by-product of survivors’ difficulty in establishing or maintaining lasting intimate relationships.
Survivors’ presumed difficulty in identifying safe partners may help explain growing evidence that women with CSA histories are more likely to form relationships with men who are physically and sexually aggressive than are women without CSA histories (Banyard, Arnold, & Smith, 2000; Cohen et al., 2000; DiLillo, Giuffre, Tremblay, & Peterson, 2001; El-Bassel et al., 1998). Men who perpetrate intimate partner violence are also more likely to have a history of multiple sex partners, unprotected anal sex, and sex with a drug-using partner (Beadnell, Baker, Morrison, & Knox, 2000; Cohen et al., 2000; El-Bassel et al., 2001; Raj, Silverman, & Amaro, 2004; Wu, El-Bassel, Witte, Gilbert, & Chang, 2003). Affiliation with aggressive and sexually risky partners has important implications for women’s sexual health. Women who experience partner violence are less likely to use condoms consistently (Gielen, McDonnell, & O’Campo, 2002; Hogben et al., 2000; Wingood & DiClemente, 1997; Wu et al., 2003) and more likely to report an STI (El-Bassel et al., 1998; Gilbert, El-Bassel, Schilling, Wada, & Bennet, 2000; Hogben et al., 2000; Wu et al., 2003). The most likely source of STI in a woman is her primary partner (Daker-White & Barlow, 1997; Hook et al., 1992), with partner sexual risk status playing a significant role. For example, STI in women is predicted by the number of sex partners their male partners have had (Ho, Bierman, Beardsley, Chang, & Burk, 1998; Kahn, Rosenthal, Succop, Ho, & Burk, 2002).
The tendency to affiliate with violent and sexually risky men is also likely to contribute to the relationship instability that has been observed in CSA survivors. Longitudinal studies show that relationship violence is associated with increased stress, dissatisfaction, and relationship dissolution among household samples (Heyman, O’Leary, & Jouriles, 1995; Testa & Leonard, 2001a, 2001b). Sexual infidelity also predicts relationship dissolution (Previti & Amato, 2004). Women who are unhappy in their relationships with violent and unfaithful men are likely to end these relationships in favor of new ones, resulting in the accumulation of additional sexual partners.
The present study was designed to examine the association between CSA experiences and sexual risk among a community sample of young adult women. Consistent with prior research, we hypothesized that women with a history of CSA would report higher baseline levels of sexual risk, including more lifetime sexual partners and earlier age of sexual debut. However, the study is unique in considering how a woman’s sexual risk may be a function of the quality of her intimate relationships. Thus, the first goal of the study was to test a model in which CSA is hypothesized to predict the characteristics of the male partners with whom she affiliates (see Figure 1). Specifically, we hypothesized that the male partners of CSA survivors would be higher in sexual risk status (i.e., would have had more previous and concurrent sexual partners) and would perpetrate more psychological, physical, and sexual aggression against their partners compared with the partners of nonabused women. Based on prior research (e.g., Wu et al., 2003), we expected partner aggression and partner sexual risk to be correlated. As shown in Figure 1, we expected effects of CSA on partner characteristics to be at least partially mediated via the woman’s own baseline sexual risk status. We hypothesized that higher levels of partner aggression and partner sexual risk would result in lower relationship satisfaction. We did not hypothesize direct effects from CSA or from baseline sexual risk behaviors to relationship satisfaction; rather we expected these effects to be fully mediated via partner aggression and partner sexual risk. Finally, we expected a woman’s relationship satisfaction to be negatively related to the number of sex partners she reported prospectively, over the subsequent 12 months, reflecting the fact that women who are unhappy in their current relationships will initiate new relationships. To bolster confidence in the model, we tested it again among women who reported new relationships at Wave 2 and at Wave 3.
Figure 1.
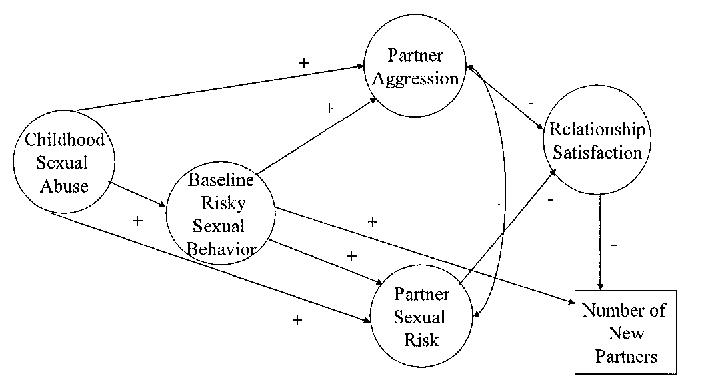
Hypothesized model of Wave 2 sexual partners as a function of childhood sexual abuse, Wave 1 partner characteristics, and Wave 1 relationship satisfaction. Arrows indicate structural paths, squares indicate observed variables, circles indicate latent factors, plus signs indicate expected positive relationships, and minus signs indicate expected negative relationships.
The second goal of the study was to examine how CSA experiences and partner characteristics may influence women’s relationship-specific STI. Many studies have demonstrated a positive relationship between CSA and history of STI (see Koenig & Clark, 2004, for a review). However, our study is unique in that we assessed STI attributable to one’s current partner, permitting examination of the effects of partner risk characteristics on women’s STI. We predicted that CSA survivors would be more likely to report STI attributable to their current partner than would women without abuse histories. However, consistent with the notion that CSA survivors are more likely to affiliate with sexually risky and aggressive partners, we hypothesized that the relationship between CSA and STI within the current relationship would be mediated via partner risk characteristics (see Figure 2). Thus, CSA survivors were expected to report higher rates of STI within their current relationships because of the elevated risk status of their intimate partners.
Figure 2.
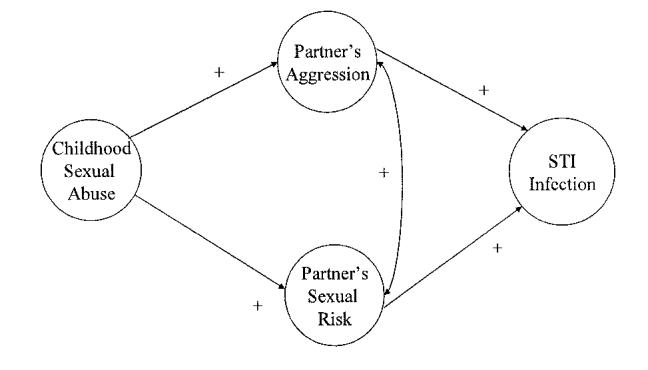
Hypothesized model of sexually transmitted infection (STI) in current relationship as a function of childhood sexual abuse and partner characteristics. Arrows indicate structural paths, circles indicate latent factors, and plus signs indicate expected positive relationships.
Method
Sample
Random digit dialing of households in Buffalo, New York, and its immediate suburbs in Erie County, New York, between May 2000 and April 2002, was used to identify women 18-30 years of age for a study of alcohol use, sexual behavior, and sexual victimization among young women. Women who completed the telephone screening were recruited to participate in a prospective study on women’s social experiences. In-person interviews were completed with 1,014 women, or 61% of eligible women identified. This completion rate is comparable to surveys conducted solely by telephone (e.g., Simon et al., 2001). The sample matched closely the characteristics of the local population. For example, 75.3% were White and 16.9% were African American, compared with 72% and 21%, respectively, for the geographic area from which the sample was drawn. There were very small percentages of Hispanic (3.2%), Asian (1.6%), Native American (0.7%), and women of mixed or other background (2.4%). Also consistent with local demographics, median annual household income for the sample was about $40,000, and 95% were high school graduates (compared with 89% of 18- to 34-year-old women in Erie County). At Time 1, average age was 23.76 (SD = 3.71) and most were unmarried (76% never married, 3% divorced or legally separated). Most were employed either full time (35.0%) or part time (43.8%), and a substantial percentage was currently enrolled in college (32.6%) or graduate school (7.2%).
Procedure
Eligible women were asked to participate in a longitudinal study of women’s social experiences, consisting of three waves of data collection, 12 months apart. Initial participation involved a 2-hr session conducted at the Research Institute on Addictions at University at Buffalo, State University of New York, for which participants were paid $50. They were told that the session would include computer-administered questionnaires and a face-to-face confidential interview involving personality, alcohol and drug use, and sexual experiences. When participants arrived at the Research Institute on Addictions, we explained study procedures to them and obtained informed consent. Wave 1 data reported in the current study were collected via a computer-assisted self-interview (CASI).
Waves 2 and 3 data were collected via paper-and-pencil questionnaires that were similar to Wave 1 CASI measures but focused on the previous 12 months. Mailed questionnaires were used to maximize response rate. Reports of sexual behaviors obtained via mailed questionnaires appeared to be comparable to those obtained via CASI at a central location but the return rate was much higher (Testa, Livingston, & VanZile-Tamsen, 2005). Wave 2 questionnaires were sent to participants’ homes 12 months after the initial interview and returned by postage-paid envelope. The same procedure was followed for Wave 3 questionnaires, 12 months later. Women were sent a $50 check upon receipt of each completed questionnaire. Of the original sample of 1,014 women, 972 (95.9%) completed Wave 2 and 937 (92.4%) completed Wave 3.
Because the goal of the study was to examine the association between women’s CSA experiences and adult intimate partner relationships, analyses were limited to women who were in a sexual relationship with a man. Of 1,014 women who completed the first wave of the study, 741 reported being in a current relationship with a man that included sexual intercourse. The remainder were in a relationship that did not include sexual intercourse (n = 20), in a lesbian relationship (n = 7), or not currently in a relationship (n = 246). Of these 741, 9 refused to answer one or more of the CSA items. Because we could not determine whether these women had experienced CSA, they were dropped from subsequent analyses, resulting in 732 included in Wave 1 analyses. Women who had a current partner and hence were included in Wave 1 analyses did not differ from women without current male sexual partners in race, income, education, employment, or CSA history and were retained in the study at equal rates. Women with current partners were significantly older and more likely to be married, however.
Measures
Childhood sexual abuse. At Wave 1, women responded positively or negatively to a series of eight items describing unwanted or nonconsensual sexual experiences before age 14. These items, adapted from Whitmire, Harlow, Quina, and Morokoff (1999), included five contact items (“person kissed or hugged you in a sexual way”; “you touched or fondled another’s genitals at their request”; “person tried to touch you in a sexual way [e.g., breasts or genitals or rubbed genitals against you]”; “person touched you in a sexual way”); and three intercourse items (“person put finger or object into your vagina or anus”; “person tried to have oral, anal, or vaginal sexual intercourse”; or “person had oral, anal, or vaginal intercourse with you”). Women who reported at least one type of unwanted sexual experience before age 14 were considered to have experienced CSA. Additional questions included whether the experience occurred more than once and whether force was involved. We assessed subjective trauma by asking women how upset they were at the time of the event (or most upsetting event, if more than one) and how upset they are now (at Wave 1), using 6-point scales ranging from 1 (not at all) to 6 (extremely).
Women’s sexual history. At Wave 1, women indicated with how many people they had had sexual intercourse, even if only one time. The seven response options consisted of 0, 1, 2, 3, 4, 5-9, and 10 or more. At Waves 2 and 3 we asked this question again, specifying the number of sexual partners within the past 12 months. Women also indicated how old they were the first time they had consensual sexual intercourse and how soon they typically have sex with a new partner, with responses ranging from 1 (the first day we meet) to 6 (a year or more after meeting). Women were asked a series of questions regarding whether they had ever had chlamydia, gonorrhea, syphilis, genital warts, trichomoniasis, genital herpes, or hepatitis B. They were considered to have had an STI if they responded positively to any of these items.
Intimate partner relationships. At Wave 1, women were asked whether they were currently in a relationship with a man and, if so, to record his initials or nickname. They were then asked a series of questions specific to this man.
Relationship satisfaction was assessed with three questions. Women were asked to rate how emotionally satisfied they were with their relationship, how physically satisfied, and overall how satisfied, using 5-point scales ranging from 1 (not at all satisfied) to 5 (extremely satisfied), (M = 3.87, SD = 1.10).
To assess partner sexual risk, we asked women, “to the best of your knowledge, how many sexual partners has —had?” using a 5-point scale representing the following categories: just 1, 2-4, 5-10, 11-20, and more than 20. Women were also allowed to indicate I don’t know. Women were asked, “During your relationship, did your partner ever have sexual intercourse with anyone besides you?” Response options ranged from 1 (no, definitely not) to 4 (yes, definitely). Women were also asked, “Has your partner ever given you a sexually transmitted disease, such as chlamydia, herpes, HPV, or gonorrhea?” Response choices consisted of yes, no, and not sure, but possibly. Finally, for each identified sexual partner, women were asked to rate how frequently they used condoms when they had vaginal intercourse, using a 6-point scale ranging from 1 (never) to 6(every time).1
Women’s experiences of intimate partner aggression were assessed with the Physical Aggression (five minor and seven severe items) and Sexual Coercion subscales (three minor and four severe items) and the four severe psychological aggression items from the Conflict Tactics Scale—2 (CTS-2; Straus, Hamby, & Warren, 2003). Minor psychological aggression was not used because it is normative in intimate relationships. Examples of minor physical aggression include being grabbed, pushed, or slapped; severe aggression includes being punched, kicked, or slammed against a wall. Minor sexual coercion includes a partner insisting on sex when she didn’t want it; severe sexual coercion involves use or threats of force. Severe psychological aggression includes the partner calling her names. At Wave 1, women who indicated that they had a current male sexual partner were asked whether he had done any of the above behaviors during the course of their relationship. For Physical and Sexual Aggression subscales, women were assigned a score of 2 if any severe aggression items were endorsed, 1 if minor but not severe aggression items were endorsed, and 0 if no items were endorsed. Women were assigned a score of 1 if they reported severe psychological aggression and 0 if they did not.
At Waves 2 and 3, women were reminded of the partner they had indicated at the previous wave and asked if they were still with him. All women, regardless of whether their relationship was ongoing, were asked whether they had had a sexual relationship with anyone else. The questions on sexual behavior, partner sexual risk, partner aggression, and relationship satisfaction were repeated specific to intimate partner relationships within the past 12 months.
Results
Childhood Sexual Abuse Experiences
Of the 732 women included in Wave 1 analyses, 245 (33.5%) reported one or more unwanted sexual experiences before age 14. Of these, 51% reported unwanted contact as their most serious experience, whereas 49% reported intercourse or attempted intercourse. On average, women were 9.84 years old (SD = 3.05) at the time of the CSA experience or, if more than one experience, the one identified as most upsetting. Perpetrators included father/stepfather/mother’s partner (13.1%), other relatives (27.0%), other known adults (14.3%), nonrelated peers less than 5 years older (31.0%), strangers (2.9%), and others (8.6%); 3.3% refused to indicate relationship to perpetrator. Force or threat of force was reported in 25.3% of these incidents. Average trauma reported to have been felt at the time of the incident was 5.61 on a 7-point scale (SD = 1.71); average trauma reported to have been felt at the present time (at Wave 1) was 3.82 (SD = 2.28).
Although CSA experiences are heterogeneous, numerous studies indicate that women who have experienced any type of CSA differ from women without these experiences in a variety of domains (Oddone Paolucci, Genuis, & Violato, 2001). As a simple way of illustrating differences in sexual risk status according to CSA history, we compared women with and without these experiences (see Table 1). As hypothesized, women with a history of CSA reported higher levels of sexual risk on several variables, including greater numbers of sexual partners and greater likelihood of lifetime STI, as well as higher levels of partner sexual risk and partner aggression.
Table 1.
Bivariate Comparisons of CSA Survivors Versus Participants th No History of CSA: Wave 1
| Variable | CSA survivors (n = 245) | Other participants (n = 487) | t or χ2 | Effect size (d or M) |
|---|---|---|---|---|
| Woman’s Sexual Behavior | ||||
| Lifetime STI (%) | 39.3% | 20.3% | 29.90*** | .20 |
| STI from Wave 1 partner (%) | 5.4% | 2.7% | 3.46b | .07 |
| Lifetime Partners a | ||||
| M | 6.62 | 5.29 | 5.03*** | .40 |
| SD | 3.37 | 3.35 | ||
| Age of first consensual intercourse | ||||
| M | 16.41 | 16.92 | 3.64*** | .19 |
| SD | 2.78 | 2.47 | ||
| How soon intercourseb | ||||
| M | 3.03 | 2.88 | 1.93# | .16 |
| SD | 0.90 | 0.93 | ||
| Partner Aggression | ||||
| Physical aggression | ||||
| M | 0.46 | 0.35 | 1.94# | .16 |
| SD | 0.73 | 0.66 | ||
| Sexual aggression | ||||
| M | 0.30 | 0.18 | 3.29# | .25 |
| SD | 0.54 | 0.42 | ||
| Psychological aggression | ||||
| M | 0.25 | 0.20 | 1.38 | .12 |
| SD | 0.43 | 0.40 | ||
| Partner Sexual Risk Partner lifetime partnersa,c | ||||
| M | 6.80 | 5.57 | 2.78** | .22 |
| SD | 5.90 | 5.07 | ||
| Partner infidelity | ||||
| M | 1.82 | 1.54 | 3.15** | .26 |
| SD | 1.13 | 1.01 |
Note. CSA = childhood sexual abuse.
For display purposes, categorical response categories were replaced with approximations of the actual number of partners, that is, the category representing 5-10 partners was recoded as 7.5 partners.
Recoded so that higher values indicate having sex sooner in the relationship.
“I don’t know” responses were recoded as the sample mean.
p < .06.
p < .01.
p < .001.
CSA and Affiliation With Risky Sexual Partners
We proposed a model in which women’s CSA experiences are associated with affiliation with sexually risky and aggressive partners at Wave 1, resulting in lower Wave 1 relationship satisfaction and, ultimately, in greater numbers of sexual partners at Wave 2 (see Figure 1). The structural model of hypothesized relationships was tested with AMOS software (Arbuckle, 2003) with maximum likelihood estimation. Models were viewed as empirically adequate if they resulted in fit indices of .95 or greater (Chou & Bentler, 1995), a root-mean-square error of approximation (RMSEA) less than .08, and medium (.13 to .25) or large (greater than .25) effect sizes as measured by R2 (Hu & Bentler, 1998).
Before testing the predictive model, we used confirmatory factor analysis to test the measurement model. Confirmatory factor analysis tests whether indicators load on specific latent variables as proposed. Five latent variables were included in the model: Childhood Sexual Abuse, Risky Sexual Behavior, Partner Aggression, Partner Sexual Risk, and Relationship Satisfaction. Because the effects of CSA on later sexual behavior may be more apparent following more severe experiences, such as penetration and repeated victimization (Beitchman et al., 1991; Kendall-Tackett et al., 1993), we used as indicators for CSA three variables that assessed the severity of the CSA experienced.
First, women were given a mutually exclusive CSA score in which no abuse was coded 0, contact was coded 1, and intercourse or attempted intercourse was coded 2. Second, women were categorized according to how many times they had been victimized, 0, 1, or 2, with the highest number indicating more than one experience. Finally, the subjective ratings of degree of trauma at the time of the abuse and currently were averaged to form the third indicator. A dichotomously coded measure of whether force was used did not correlate highly with the other indicators and was not included. Risky Sexual Behavior was composed of age of first consensual sex, number of lifetime partners at Wave 1, and typical amount of time before intercourse with a new partner. Partner Aggression consisted of CTS psychological aggression, physical aggression, and sexual coercion from the current partner. Partner Sexual Risk was composed of the woman’s estimate of her partner’s number of lifetime sexual partners and his infidelity. Relationship satisfaction included ratings of overall relationship satisfaction, emotional satisfaction, and physical satisfaction. The magnitude of the loadings taken with the indices of fit—χ2(67, N = 732) = 200.90, p < .001, normal fit index (NFI) = .96, comparative fit index (CFI) = .98, RMSEA = .052 (confidence interval [CI] = .044-.061)—suggests that the measurement model represents an appropriate fit to the data (see Table 2).
Table 2.
Factor Loadings for Wave 1 Structural Equation Model
| Latent factor and indicator | Loading |
|---|---|
| Childhood Sexual Abuse | |
| Severitya | 0.96 |
| Multiple Experiences | 0.97*** |
| Subjective Trauma Ratings | 0.92*** |
| Risky Sexual Behavior | |
| Lifetime Partnersa | 0.96 |
| First Consensual Sexb | 0.48*** |
| How Soonc | 0.54*** |
| Partner’s Aggression | |
| Sexual Aggressiona | 0.44 |
| Physical Aggression | 0.78*** |
| Psychological Aggression | 0.75*** |
| Partner’s Sexual Risk | |
| Infidelitya | 0.57 |
| Lifetime Partners | 0.46*** |
| Relationship Satisfaction | |
| Overall Satisfactiona | 0.93 |
| Emotional Satisfaction | 0.92*** |
| Physical Satisfaction | 0.61** |
Statistical significance of loading was not tested because it was fixed at 1.00.
Because lower scores on age of first consensual intercourse are considered more risky, the variable was conceptualized as the number of years before age 20 that the woman was sexually active. Women who first had consensual sex at age 20 or later received a 0.
How soon was recoded so that higher scores indicate higher risk (i.e., having sex sooner).
p < .01.
p < .001.
Figure 3 shows results of the analysis predicting number of Wave 2 sexual partners as a function of Wave 1 relationship quality. The model showed good fit to the data—χ2(78, N = 732) = 235.25, p < .001, NFI = .96, CFI = .97, RMSEA = .053 (CI = .045-.060). Explained variance (R2) in relationship satisfaction was .30; R2 for prediction of Wave 2 partners was .13. As expected, increasing severity of CSA was associated with affiliation with sexually risky and aggressive intimate partners at Wave 1, an effect that was partially mediated via women’s higher levels of baseline sexual risk. Partner aggression and sexual risk characteristics were negatively associated with Wave 1 relationship satisfaction, which was negatively associated with number of Wave 2 sexual partners. Consistent with our notion that the effects of CSA on relationship satisfaction are mediated via partner characteristics, the direct effects from CSA and risky sexual behavior to relationship satisfaction were very small and nonsignificant.2
Figure 3.
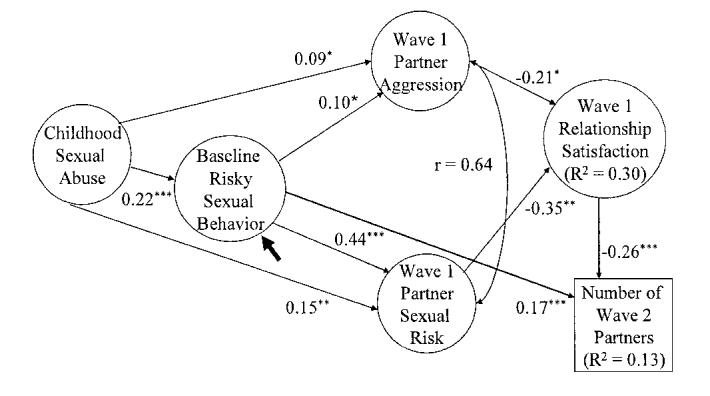
Wave 2 sexual partners as a function of childhood sexual abuse, Wave 1 partner characteristics, and Wave 1 relationship satisfaction. Arrows indicate structural paths, squares indicate observed variables, and circles indicate latent factors. *p < .05. **p < .01. ***p < .001.
To increase confidence in the model, we sought to replicate it using Wave 2 relationship data to predict Wave 3 sexual partners. We expected that CSA would be associated with a continued tendency to affiliate with more aggressive and sexually riskier partners, which would again result in lower relationship satisfaction and increased number of subsequent sexual partners. To appropriately test the hypothesized relationship between CSA and partner characteristics, we limited the analysis to women who reported being in a current relationship at Wave 2 with a man other than the Wave 1 partner (n = 188). Not surprisingly given the modest sample size, fit was not as high as for Wave 1 data—χ2(81, N = 188) = 159.26, p < .001; NFI = .87, CFI = .93, RMSEA = .072 (CI = .055-.088).3 Nonetheless, the model explained a substantial amount of variance in relationship satisfaction (R2 = .69) and Wave 3 partners (R2 = .15) and provided partial support for hypotheses (see Figure 4). Again, CSA predicted partner sexual risk, via the woman’s baseline sexual risk. Partner sexual risk predicted relationship satisfaction, which predicted number of Wave 3 sexual partners. Paths involving partner aggression were in the expected direction but did not attain statistical significance.
Figure 4.
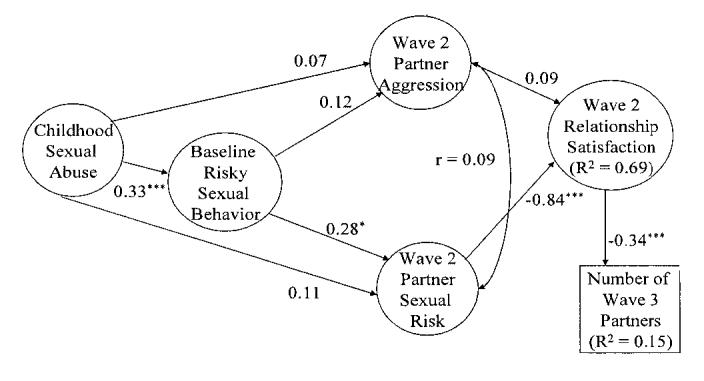
Wave 3 sexual partners as a function of childhood sexual abuse, Wave 2 partner characteristics, and Wave 2 relationship satisfaction. Arrows indicate structural paths, squares indicate observed variables, and circles indicate latent factors. *p < .05. ***p < .001.
Finally, we sought to replicate the model again using those women who reported a new partner at Wave 3 (n = 156). We were unable to examine the link between Wave 3 satisfaction and subsequent number of new partners because we had only three waves of data; however we could still examine the proposed links between CSA, partner characteristics, and relationship satisfaction. Despite the small sample size, the model explained a substantial amount of variance in relationship satisfaction, R2 = .54, although fit was only fair—χ2(72, N = 156) = 143.76, p < .001, NFI = .88, CFI = .93, RMSEA = .080 (CI = .061-.099). As shown in Figure 5, paths were similar to those observed at Wave 2, except that at Wave 3 the expected relationship between CSA and partner aggression attained statistical significance. Thus, across three different partner relationships, we found support for the hypothesized association between CSA and affiliation with sexually risky and more aggressive partners, resulting in lower relationship satisfaction. Moreover, at Waves 1 and 2, lower relationship satisfaction prospectively predicted higher number of sexual partners.
Figure 5.
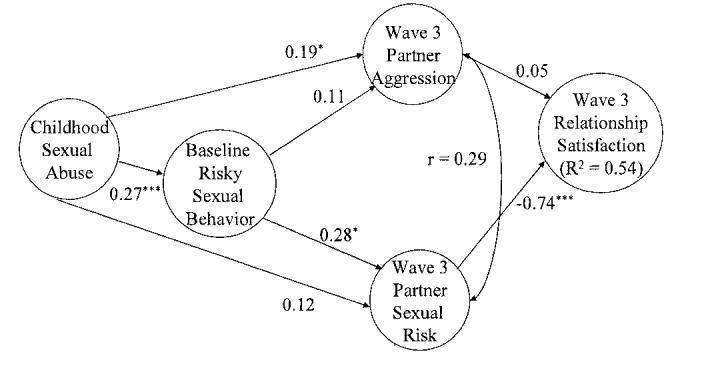
Wave 3 relationship satisfaction as a function of childhood sexual abuse and Wave 3 partner characteristics. Arrows indicate structural paths, and circles indicate latent factors. *p < .05. ***p < .001.
STI
We hypothesized that the tendency of CSA survivors to affiliate with more aggressive and more sexually risky men would result in higher incidence of STI attributable to current partner. As expected, at Wave 1, CSA survivors were more likely to indicate that they had contracted an STI from their current partner (5.4%) than were women without CSA histories (2.7%), a difference that was marginally significant, odds ratio (OR) = 2.11 (CI = 0.96-4.63), p = .06. As demonstrated in the structural models (see Figure 2), CSA was associated with affiliation with partners higher in sexual risk and aggression. To test the hypothesis that the relationship between CSA and STI is mediated via these partner characteristics, we used logistic regression to examine the impact of partner aggression and partner sexual risk on STI after controlling for CSA. The three partner aggression variables (physical aggression, sexual coercion, and psychological aggression) and two sexual risk variables (partner’s partners and infidelity) were modestly inter-correlated (range = .15-.59). Number of partner’s partners, OR = 1.47 (1.01-2.13), p < .05, and partner infidelity, OR = 1.74 (CI = 1.22-2.48), p < .01, both predicted odds of STI from partner, although none of the three partner aggression variables did. After we controlled for partner variables, the association between CSA and STI was reduced to nonsignificance (OR = 1.51 (CI = 0.65-3.50), p = .34) suggesting mediation. To more rigorously test mediation, we performed separate Sobel tests (Sobel, 1982): the first testing mediation of CSA to STI via partner’s partners and the second testing mediation of CSA to STI via partner infidelity. Both tests were significant, indicating that there are significant mediated effects of CSA on STI in current relationship via partner’s partners (Z = 2.26, p < .02), and via partner infidelity (Z = 2.76, p < .01)4
We were unable to repeat the STI analyses using reported infection from new Wave 2 and Wave 3 partners because few women reported being infected by these partners (6 at Wave 2 and 3 at Wave 3). These low rates are not surprising given that the average length of Wave 2 and Wave 3 relationships was only about 6 months.
Discussion
Numerous studies have demonstrated an association between CSA and adult sexual risk behaviors among women. This study is no exception. However, the current study is unique in suggesting that the elevated sexual risk status of adult survivors, including higher numbers of sexual partners and higher rates of STI, can be at least partially explained by the quality of women’s intimate relationships. Across three relationships, CSA was associated with affiliation with more aggressive and more sexually risky partners. One consequence of the tendency to affiliate with riskier partners was higher rates of STI resulting from the current relationship. Another consequence was lower relationship satisfaction, which prospectively predicted entering new sexual relationships.
Our model lends insight into the frequently observed association between CSA and adult relationship satisfaction. Although it has been suggested that low relationship satisfaction reflects survivors’ hostility toward men or their difficulties with intimacy, communication, or trust (see DiLillo, 2001, for a review), we did not observe a direct relationship between CSA and relationship satisfaction. Rather, in three replications of the model, with three different relationships, we consistently found that the relationship between CSA and satisfaction was mediated via the characteristics of the men with whom CSA survivors affiliate. It is not surprising that satisfaction is lower among women who affiliate with more aggressive and more sexually risky men. Given the quality of these relationships, dissatisfaction and dissolution should not be viewed as necessarily bad outcomes. However, the pattern of unhappy relationships contributes to the accumulation of more sexual partners over time, a risk factor for both STI (e.g., Hogben et al., 2000) and sexual victimization (e.g., Gidcyz, Hanson, & Layman, 1995).
The present study cannot completely explain why or how CSA survivors come to affiliate with higher risk men, although it can lend some insight. The tendency for CSA experiences to predict affiliation with higher risk men was partially mediated via the woman’s tendency toward higher levels of baseline sexual risk, such as early age of first intercourse and higher numbers of previous sexual partners. Thus, affiliation with high risk men may reflect attraction between similar others (e.g., D. Byrne, 1971) or a tendency for people to meet similar others as a result of engaging in common activities, such as going to bars or parties in an attempt to meet new people. Similarly, CSA has been associated among adolescents with antisocial behavior (Bergen, Martin, Richardson, Allison, & Roeger, 2004), delinquency (Herrera & McCloskey, 2003), and affiliation with deviant peer groups (Fergusson & Horwood, 1999). Young women who engage in these behaviors are likely to meet partners within these social circles who are prone to antisocial behavior, such as violence and infidelity. Finally, although not examined in this study, it is also possible that survivors’ interpersonal difficulties (see DiLillo, 2001, for a review) influence their partner choices.
The use of a large representative community sample and replication of our model across time periods are strengths of the current study, facilitating generalization. Nonetheless, we acknowledge several limitations. First, reports of CSA were made retrospectively, at one point in time. These reports may not be stable over time, with the most well-adjusted adults most likely to fail to report abuse (Hardt & Rutter, 2004). This would have the effect of inflating the effects attributable to CSA. Further, we did not assess or control for childhood physical abuse, although results were unchanged after controlling for family disruptions and parental education. Reports of partner behavior were based solely on the woman’s reports and may have been inaccurate or biased by their own behavior, possibly accounting for the strong association between a woman’s baseline sexual risk and that of her partner. Nonetheless, among a subsample of the current sample, we found high concordance between the woman’s estimates of her partner’s partners and his own reports (see Footnote 1), bolstering confidence in the accuracy of women’s reports of their partners’ sexual behavior.
In general, model testing provided support for hypotheses and explained a large amount of variance in relationship satisfaction and a moderate amount in number of sexual partners. Nonetheless, other potential mechanisms and pathways that we did not or could not test might also have been at work. For example, although our results support the notion that a woman’s sexual risk reflects her difficulties in establishing intimate relationships, we cannot rule out the possibility that survivors are motivated to engage in sex with multiple partners, perhaps as a form of tension reduction or experiential avoidance arising from posttraumatic stress disorder (e.g., Polusny & Follette, 1995). It is possible that both mechanisms influence women’s sexual behavior. Further, we recognize that CSA survivors are a diverse group, representing a range of functioning. Although as a group women with CSA histories are more likely to experience troubled relationships, there are some survivors who are able to achieve satisfying and stable relationships and others who avoid intimate relationships altogether (Davis & Petretic-Jackson, 2000). Hence, the pattern of relationship difficulties leading to partner change and affiliation with high risk partners does not necessarily fit the experience of all women with histories of CSA.
These findings are important and novel in suggesting that the link between CSA and women’s sexual risk may reflect women’s difficulties in intimate relationships. However, additional research is necessary to fully understand this process. For example, the role of CSA in evaluating potential romantic partners has, to our knowledge, not been explored. Research is needed to understand whether women who have experienced CSA fail to recognize potential risk in a partner or whether CSA survivors recognize a man’s risk potential but are still willing to pursue a relationship, perhaps because of a more compelling desire for intimacy. Alternatively, research is necessary to better understand how higher levels of substance use, antisocial behavior, and sexual activity associated with CSA may influence the type of men that survivors are likely to meet (National Institute of Mental Health Multisite HIV Prevention Trial, 2001). The study suggests that the higher levels of sexual risk behaviors and negative sexual outcomes observed among CSA survivors may be ameliorated by addressing women’s difficulties in establishing and maintaining safe and stable relationships. This is likely to involve addressing the issues of trust and communication that may hamper relationship functioning and dispelling the notion that one needs a partner. On the other hand, addressing HIV risk reduction in CSA survivors, for example, through increasing sexual assertiveness (see Briere, 2004), may improve relationship quality and help women to be more discriminating in deciding to enter a new relationship. The model that we have suggested is complex and findings are preliminary, necessitating replication before warranting changes in clinical practice. However, we believe that the model that we have suggested may prove heuristic both in conceptualizing the long-term implications of CSA for women’s intimate relationships and in suggesting an alternative way of viewing women’s sexual risk behaviors.
Footnotes
This research was supported by National Institute on Alcohol Abuse and Alcoholism and National Institutes of Health Director’s Office of Research on Women’s Health Grant R01 AA12013 and National Institute on Alcohol Abuse and Alcoholism Grant K02 AA00284 awarded to Maria Testa.
Recognizing the limitations of collecting data on men’s sexual behavior from their female partners, at Wave 3 we collected from a subsample of male partners (n = 172) self-report data on their own sexual behaviors. We found excellent agreement between women and their partners on number of man’s sex partners (r = .67), frequency of condom use (r = .85), the man’s infidelity (85% agreement), and the woman’s contraction of STI from her partner (90% agreement).
Some studies suggest that the apparent effects of CSA are reduced or eliminated after controlling for the effects of family background (see Muehlenhard, Highby, Lee, Bryan, & Dodrill, 1998). At Wave 3, we collected data on parents’ education and childhood disruptions (e.g., parental death or divorce). The models were rerun controlling for these variables throughout; the results were unchanged. We also performed a two-group analysis with the Wave 1 model to test its equivalence for married versus unmarried women. The direction of all relationships was identical for the two groups, suggesting that the model is appropriate for both married and unmarried women. The only difference in paths between the two groups was that there was a significant negative relationship between Wave 1 relationship satisfaction and Wave 2 partners for single women (-.27, p < .001); however, this relationship did not attain statistical significance for married women (-.12, p < .09).
Degrees of freedom differ across the three models because, in the models for Waves 2 and 3, the variance of the error term for number of lifetime partners had to be fixed at a low positive value (1.00) for the model to converge (B. M. Byrne, 1994). In addition, for the Wave 2 analysis to converge, both the variance of the disturbance of relationship satisfaction and the error variance of psychological aggression were also fixed to low positive values (0.25 and 0.05, respectively). For the Wave 3 analysis, the error variances of sexual coercion, physical aggression, and overall satisfaction were fixed at low positive numbers (0.05, 0.05, and 0.01, respectively) as was the variance of the disturbance of partner’s sexual risk (0.50).
Because number of sexual partners is a well-established risk factor for STI (e.g., Hogben et al., 2000) and is strongly related to CSA, we repeated the analysis, using women’s number of Wave 1 partners, rather than CSA, to predict STI attributable to current (Wave 1) partner. As expected, there was a direct relationship between women’s number of Wave 1 partners and STI from current partner, OR = 1.5 (CI = 1.11-2.02), p < .01. This relationship became nonsignificant after partner characteristics were entered into the equation, OR = 1.26 (CI = 0.93-1.70), p = .14. In this analysis, partner infidelity was the only significant predictor of STI, OR = 1.72 (CI = 1.21-2.44), p < .01. Sobel test revealed a statistically significant mediational effect of partner infidelity, Z = 3.21, p < .01, in the relationship between women’s number of sexual partners and STI from current partner.
References
- Arbuckle JL. AMOS (Version 5.0) [Computer software] SmallWaters Corporation; Chicago: 2003. [Google Scholar]
- Banyard VL, Arnold S, Smith J. Childhood sexual abuse and dating experiences of undergraduate women. Child Maltreatment. 2000;5:39–48. doi: 10.1177/1077559500005001005. [DOI] [PubMed] [Google Scholar]
- Beadnell B, Baker SA, Morrison DM, Knox K. HIV/STD risk factors for women with violent male partners. Sex Roles. 2000;42:661–689. [Google Scholar]
- Beitchman JH, Zucker KJ, Hood JE, DaCosta GA, Akman D. A review of the short-term effects of child sexual abuse. Child Abuse & Neglect. 1991;15:537–556. doi: 10.1016/0145-2134(91)90038-f. [DOI] [PubMed] [Google Scholar]
- Bergen HE, Martin G, Richardson AS, Allison S, Roeger L. Sexual abuse, antisocial behaviour and substance use: Gender differences in young community adolescents. Australian & New Zealand Journal of Psychiatry. 2004;38:34–41. doi: 10.1111/j.1440-1614.2004.01295.x. [DOI] [PubMed] [Google Scholar]
- Briere J. Integrating HIV/AIDS prevention activities into psychotherapy for child sexual abuse survivors. In: Koenig LJ, Doll LS, O’Leary A, Pequegnat W, editors. From child sexual abuse to adult sexual risk: Trauma, revictimization, and intervention. American Psychological Association; Washington, DC: 2004. pp. 219–232. [Google Scholar]
- Byrne BM. Structural equation modeling with EQS and EQS/Windows. Sage; Thousand Oaks, CA: 1994. [Google Scholar]
- Byrne D. The attraction paradigm. Academic Press; New York: 1971. [Google Scholar]
- Chou C-P, Bentler PM. Estimates and tests in structural equation modeling. In: Hoyle RH, editor. Structural equation modeling: Concepts, issues, and applications. Sage; Thousands Oaks, CA: 1995. pp. 37–55. [Google Scholar]
- Cohen M, Deamant C, Barkan S, Richardson J, Young M, Holman S, et al. Domestic violence and childhood sexual abuse in HIV-infected women and women at risk for HIV. American Journal of Public Health. 2000;90:560–565. doi: 10.2105/ajph.90.4.560. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Daker-White G, Barlow D. Heterosexual gonorrhoea at St Thomas’. II: Sexual behaviour and sources of infection. International Journal of STD & AIDS. 1997;8:102–108. doi: 10.1258/0956462971919642. [DOI] [PubMed] [Google Scholar]
- Davis JL, Petretic-Jackson PA. The impact of child sexual abuse on adult interpersonal functioning: A review and synthesis of the empirical literature. Aggression and Violent Behavior. 2000;5:291–328. [Google Scholar]
- DiLillo D. Interpersonal functioning among women reporting a history of childhood sexual abuse: Empirical findings and methodological issues. Clinical Psychology Review. 2001;21:553–576. doi: 10.1016/s0272-7358(99)00072-0. [DOI] [PubMed] [Google Scholar]
- DiLillo D, Giuffre D, Tremblay GC, Peterson L. A closer look at the nature of intimate partner violence reported by women with a history of child sexual abuse. Journal of Interpersonal Violence. 2001;16:116–132. [Google Scholar]
- DiLillo D, Long PJ. Perceptions of couple functioning among female survivors of child sexual abuse. Journal of Child Sexual Abuse. 1999;7:59–76. [Google Scholar]
- El-Bassel N, Fondevila J, Gilbert L, Voisin D, Richman BL, Pitchell P. HIV risks of men in methadone maintenance treatment programs who abuse their intimate partners: A forgotten issue. Journal of Substance Abuse. 2001;13:29–43. doi: 10.1016/s0899-3289(01)00068-2. [DOI] [PubMed] [Google Scholar]
- El-Bassel N, Gilbert L, Krishnan S, Schilling RF, Gaeta T, Purpura S, Witte SS. Partner violence and sexual HIV-risk behaviors among women in an inner-city emergency department. Violence and Victims. 1998;13:377–392. [PubMed] [Google Scholar]
- Fergusson DM, Horwood LJ. Prospective childhood predictors of deviant peer affiliations in adolescence. Journal of Child Psychology and Psychiatry. 1999;40:581–592. [PubMed] [Google Scholar]
- Finkelhor D, Browne A. The traumatic impact of child sexual abuse: A conceptualization. American Journal of Orthopsychiatry. 1985;55:530–541. doi: 10.1111/j.1939-0025.1985.tb02703.x. [DOI] [PubMed] [Google Scholar]
- Gidcyz CA, Hanson K, Layman MJ. A prospective analysis of the relationship among sexual assault experiences. Psychology of Women Quarterly. 1995;19:5–19. [Google Scholar]
- Gielen AC, McDonnell KA, O’Campo PJ. Intimate partner violence, HIV status, and sexual risk reduction. AIDS and Behavior. 2002;6:107–116. [Google Scholar]
- Gilbert L, El-Bassel N, Schilling RF, Wada T, Bennet B. Partner violence and sexual HIV risk behaviors among women in methadone treatment. AIDS and Behavior. 2000;4:261–269. [Google Scholar]
- Hardt J, Rutter M. Validity of adult retrospective reports of adverse childhood experiences: Review of the evidence. Journal of Child Psychology and Psychiatry. 2004;45:260–273. doi: 10.1111/j.1469-7610.2004.00218.x. [DOI] [PubMed] [Google Scholar]
- Heiman JR, Heard-Davison AR. Child sexual abuse and adult sexual relationships: Review and perspective. In: Koenig LJ, Doll LS, O’Leary A, Pequegnat W, editors. From child sexual abuse to adult sexual risk: Trauma, revictimization, and intervention. American Psychological Association; Washington, DC: 2004. pp. 13–47. [Google Scholar]
- Herrera VM, McCloskey LA. Sexual abuse, family violence, and female delinquency: Findings from a longitudinal study. Journal of Interpersonal Violence. 2003;18:319–334. doi: 10.1891/vivi.2003.18.3.319. [DOI] [PubMed] [Google Scholar]
- Heyman RE, O’Leary KD, Jouriles EN. Alcohol and aggressive personality styles: Potentiators of serious physical aggression against wives? Journal of Family Psychology. 1995;9:44–57. [Google Scholar]
- Ho GY, Bierman R, Beardsley L, Chang CJ, Burk RD. Natural history of cervicovaginal papillomavirus infection in young women. New England Journal of Medicine. 1998;338:423–428. doi: 10.1056/NEJM199802123380703. [DOI] [PubMed] [Google Scholar]
- Hogben M, Gange SJ, Watts DH, Robison E, Young M, Richardson J, et al. The effect of sexual and physical violence on risky sexual behavior and STDs among a cohort of HIV seropositive women. AIDS & Behavior. 2000;4:353–361. [Google Scholar]
- Hook EW, Reichart CA, Upchurch DM, Ray P, Celentano D, Quinn TC. Comparative behavioral epidemiology of gonococcal and chlamydial infections among patients attending a Baltimore sexually transmitted disease clinic. American Journal of Epidemiology. 1992;136:662–672. doi: 10.1093/oxfordjournals.aje.a116546. [DOI] [PubMed] [Google Scholar]
- Hu L, Bentler PM. Fit indices in covariance structure modeling: Sensitivity to underparameterized model misspecification. Psychological Methods. 1998;3:424–453. [Google Scholar]
- Kahn JA, Rosenthal SL, Succop PA, Ho GY, Burk RD. Mediators of the association between age of first sexual intercourse and subsequent human papillomavirus infection. Pediatrics. 2002;109:E5. doi: 10.1542/peds.109.1.e5. [DOI] [PubMed] [Google Scholar]
- Kendall-Tackett KA, Williams LM, Finkelhor D. Impact of sexual abuse on children: A review and synthesis of recent empirical studies. Psychological Bulletin. 1993;113:164–180. doi: 10.1037/0033-2909.113.1.164. [DOI] [PubMed] [Google Scholar]
- Koenig LJ, Clark H. Sexual abuse of girls and HIV infection among women: Are they related? In: Koenig LJ, Doll LS, O’Leary A, Pequegnat W, editors. From child sexual abuse to adult sexual risk: Trauma, revictimization, and intervention. American Psychological Association; Washington, DC: 2004. pp. 69–92. [Google Scholar]
- Muehlenhard CL, Highby BJ, Lee RS, Bryan TS, Dodrill WA. The sexual revictimization of women and men sexually abused as children: A review of the literature. Annual Review of Sex Research. 1998;9:1–47. [PubMed] [Google Scholar]
- National Institute of Mental Health Multisite HIV Prevention Trial A test of factors mediating the relationship between unwanted sexual activity during childhood and risky sexual practices among women enrolled in the NIMH Multisite HIV Prevention Trial. Women & Health. 2001;33:163–180. doi: 10.1300/j013v33n01_10. [DOI] [PubMed] [Google Scholar]
- Oddone Paolucci E, Genuis ML, Violato C. A meta-analysis of the published research on the effects of child sexual abuse. Journal of Psychology. 2001;135:17–36. doi: 10.1080/00223980109603677. [DOI] [PubMed] [Google Scholar]
- Parillo KM, Freeman RC, Collier K, Young P. Association between early sexual abuse and adult HIV-risky sexual behaviors among community-recruited women. Child Abuse & Neglect. 2001;25:335–346. doi: 10.1016/s0145-2134(00)00253-2. [DOI] [PubMed] [Google Scholar]
- Polusny MA, Follette VM. Long-term correlates of child sexual abuse: Theory and review of the empirical literature. Applied and Preventive Psychology. 1995;4:143–166. [Google Scholar]
- Previti D, Amato PR. Is infidelity a cause or a consequence of poor marital quality? Journal of Social and Personal Relationships. 2004;21:217–230. [Google Scholar]
- Raj A, Silverman JG, Amaro H. Abused women report greater male partner risk and gender-based risk for HIV: Findings from a community-based study with Hispanic women. AIDS Care. 2004;16:519–529. doi: 10.1080/09540120410001683448. [DOI] [PubMed] [Google Scholar]
- Rumstein-McKean O, Hunsley J. Interpersonal and family functioning of female survivors of childhood sexual abuse. Clinical Psychology Review. 2001;21:471–490. doi: 10.1016/s0272-7358(99)00069-0. [DOI] [PubMed] [Google Scholar]
- Simon TR, Anderson M, Thompson MP, Crosby AE, Shelley G, Sacks JJ. Attitudinal acceptance of intimate partner violence among U. S. adults. Violence and Victims. 2001;16:115–126. [PubMed] [Google Scholar]
- Sobel ME. Asymptotic confidence intervals for indirect effects in structural equation models. In: Leinhardt S, editor. Sociological methodology 1982. American Sociological Association; Washington, DC: 1982. pp. 290–312. [Google Scholar]
- Straus MA, Hamby SL, Warren WL. The Conflict Tactics Scales handbook. Western Psychological Services; Los Angeles: 2003. [Google Scholar]
- Testa M, Leonard KE. The impact of husband physical aggression and alcohol use on marital functioning: Does alcohol “excuse” the violence. Violence and Victims. 2001a;16:507–516. [PubMed] [Google Scholar]
- Testa M, Leonard KE. The impact of marital aggression on women’s psychological and marital functioning in a newlywed sample. Journal of Family Violence. 2001b;16:115–130. [Google Scholar]
- Testa M, Livingston JA, VanZile-Tamsen C. The impact of questionnaire administration mode on response rate and reporting of consensual and non-consensual sexual behavior. Psychology of Women Quarterly. 2005;29:345–352. [Google Scholar]
- Whitmire LE, Harlow LL, Quina K, Morokoff PJ. Childhood trauma and HIV. Brunner/Mazel; Philadelphia: 1999. [Google Scholar]
- Wingood GM, DiClemente RJ. The effects of an abusive primary partner on the condom use and sexual negotiation practices of African-American women. American Journal of Public Health. 1997;87:1016–1018. doi: 10.2105/ajph.87.6.1016. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wu E, El-Bassel N, Witte SS, Gilbert L, Chang M. Intimate partner violence and HIV risk among urban minority women in primary health care settings. AIDS and Behavior. 2003;7:291–301. doi: 10.1023/a:1025447820399. [DOI] [PubMed] [Google Scholar]