

Abstract
A 25-year-old woman, pregnant for 38 weeks, was admitted to our clinic with dyspnea. Transthoracic echocardiography revealed a large cyst that originated from the left side of the interventricular septum, decreasing left ventricular volume and almost entirely obstructing the left ventricular outflow tract. Cardiac magnetic resonance imaging confirmed a grade 1 hydatid cyst, which measured 61 × 59 × 66 mm.
The cyst was excised after cesarean section. Extirpation required the creation of a small septal defect, which we closed without a patch, by suturing the septum directly to the left ventricular wall. The patient was discharged without symptoms.
The case reported here is of particular interest not only because a hydatid cyst is rarely seen in the interventricular septum, but because a giant hydatid cyst obstructing the left ventricular outflow tract is very rare in pregnancy. (Tex Heart Inst J 2002;29:333–5)
Key words: Adult; case report; echinococcosis/diagnosis; echinococcosis/surgery; echocardiography; female; heart septum/pathology; heart septum/surgery; magnetic resonance imaging; myocardial diseases/parasitology; pregnancy complications, parasitic
Cardiac hydatid cyst is a rare condition, and the location of a hydatid cyst in the interventricular septum is exceptional. 1 Echinococcosis (echinococcal hydatidosis) is an important health problem in some regions of the world. Although cases are found sporadically in western countries, most of those occur in immigrants from areas where echinococcosis is endemic. 2 We report the case of a 25-year-old woman, pregnant for 38 weeks, who had a giant cardiac hydatid cyst that originated from the interventricular septum and almost entirely obstructed the left ventricular outflow tract.
Case Report
In May 2001, a 25-year-old woman, pregnant for 38 weeks, was admitted to our clinic with dyspnea. The patient had no notable medical history, but her mother had undergone surgery for a hydatid cyst of the liver. On auscultation, there was a systolic murmur at the mesocardiac area. On electrocardiography, we saw no conduction disorder or ischemia. Transthoracic echocardiography (TTE), however, revealed a 50- × 60-mm round, cyst-like structure that originated from the left side of the interventricular septum, decreasing left ventricular volume and almost entirely obstructing the left ventricular outflow tract (Fig. 1). The patient also had slight mitral insufficiency, and the anterior leaflet of the mitral valve was in contact with the cyst. Slight aortic insufficiency (mean gradient, 35 mmHg) was also observed. Cardiac magnetic resonance imaging (MRI) confirmed a grade 1 hydatid cyst, which measured 61 × 59 × 66 mm. An abdominal MRI scan showed a 2nd hydatid cyst, in the right lobe of the liver, with dimensions of 109 × 93 × 81 mm. The laboratory findings and the chest radiograph were normal. Serologic tests were positive for hydatid cyst. At the 39th week of pregnancy, delivery was performed by cesarean section; 20 days later, the patient underwent operation for the cardiac hydatid cyst.
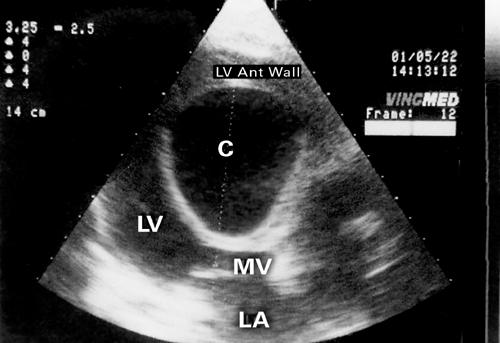
Fig. 1 This preoperative transthoracic echocardiogram reveals a 50- × 60-mm round, cyst-like structure (C) that originates from the left side of the interventricular septum, decreases left ventricular volume, and almost entirely obstructs the left ventricular outflow tract.
LA = left atrium; LV = left ventricle; LV ANT = left ventricular anterior; MV = mitral valve
After induction of general anesthesia and approach via a median sternotomy, standard cardiopulmonary bypass was initiated under mild hypothermia (28 °C), and the heart was arrested with isothermic blood cardioplegic solution. We reached the cyst by means of an incision through the upper part of the right ventricular outflow tract and interventricular septum, then sterilized it by injecting 20% hypertonic saline solution into the cystic cavity. After aspirating the cystic material, we enucleated the mass (Fig. 2) and washed the residual cavity with 20% hypertonic saline solution and 1% iodine solution.

Fig. 2 Cystic material removed from the interventricular septum.
Because the interventricular septum between the cystic cavity and the left ventricular cavity was thin and was bulging towards the left ventricular outflow tract, we excised a small part of the septum in a manner that did not damage the conductive tissue, the papillary muscles, or the mitral or aortic valves. The resultant septal defect was closed without a patch, by suturing the right part of the septum (which was thick) directly to the left ventricular wall. Both the interventricular septum and the ventriculotomy were closed with polypropylene running suture.
The cystic material was examined histopathologically, which confirmed the surgical observation of hydatid cyst. The postoperative period was uneventful, and the patient was discharged from the hospital on the 8th postoperative day. We prescribed albendazole to prevent recurrence, and we scheduled the patient for excision of the hepatic hydatid cyst 6 weeks after discharge. In contrast with the preoperative echocardiographic finding, an echocardiographic evaluation 4 months after the operation revealed no gradient in the left ventricular outflow tract. Nor did we observe any other cardiac problems. Subsequent follow-up examinations have also been negative.
Discussion
Echinococcosis is a tissue infestation. In human beings, it is caused by the larva of Echinococcus granulosus. 2–6 Most often, the sheep is the intermediate host and the dog the definitive host, but man is a common accidental host. 7 Adult helminths mature in the intestinal mucosa of the final host, who ate the uncooked, cyst-containing meat from the intermediate host. Larvae usually reach the myocardium through the coronary circulation, although the intestinal lymphatic vessels, the thoracic duct, the upper and lower vena cavae, and the hemorrhoidal veins of the large intestine may also be pathways. Cardiac involvement through pulmonary veins has also been reported. 4
Cardiac echinococcosis is not frequent, accounting for only 0.5% to 2% of all hydatid infestations. 2–5 The distribution of echinococcosis in the heart depends, of course, on the blood supply to that part of the heart. The left ventricle, the part of the heart that has the most abundant blood supply, is involved most frequently (55%–60% of the time). 4,8 Involvement of the interventricular septum is reported in 5% to 9% of cardiac cases. The right atrium is involved in 3% to 4% of cases, and the right ventricle in 15%. Distribution in the left atrium, pulmonary artery, and pericardium occurs in 8%, 7%, and 8% of cardiac cases, respectively. 4
In the rare instances in which cardiac echinococcal cysts involve the interventricular septum, they can cause symptoms related to compression of the conduction pathway (atrioventricular block and syncopal attacks 7) and obstruction of the right or left ventricular outflow tract. 3 The case reported here is of particular interest not only because a hydatid cyst is rarely seen in the interventricular septum, but because a giant hydatid cyst obstructing the left ventricular outflow tract is very rare in pregnancy.
Other cardiovascular manifestations of cardiac echinococcosis are arrhythmia, angina, valvular dysfunction, pericardial reaction, pulmonary or systemic embolism, pulmonary hypertension, and anaphylactic reactions. 3 Patients who have a history of echinococcosis and who are admitted with these symptoms and signs must be evaluated for cardiac involvement. Because the condition can mimic a number of cardiac diseases (even when the septum alone is involved), the differential diagnosis includes all other cardiac tumors and cysts, mediastinal tumor, pericardial cyst, and ventricular aneurysm. 7 This last is the most common finding, but it is easily differentiated by angiography. 7
Although cardiac catheterization and angiography have long been held to provide the only definitive preoperative means of diagnosing cardiac hydatidosis, the procedure is invasive and yields little information that cannot be obtained by TTE when that result is confirmed by computed tomography or MRI. 7 Indeed, some authors now contend that TTE is the gold standard because it is noninvasive, easily performed, and has a high sensitivity in detecting intracardiac echinococcosis. 3 In our patient, we made the diagnosis by TTE, confirmed by MRI and serologic tests. Serologic tests are a helpful supplement, but false-negative results are possible.
Because there is still no medical treatment for cardiac cysts, surgical excision remains the only remedy. Fortunately, cystectomy is associated with a high rate of complete recovery. 7 When a hydatid cyst is going to be removed, it should be sterilized before enucleation by injection or instillation of a helminthicide: 2% formalin, 0.5% silver nitrate solution, 20% hypertonic saline solution, 1% iodine solution, or 5% cetrimonium bromide solution. 3 The use of substances toxic to the patient (such as formalin and absolute alcohol) should be reserved for application in areas where they cannot enter the bloodstream. 7 We injected 20% hypertonic saline solution. Pads soaked in an aqueous sodium chloride solution can also be used to good effect in protecting the surgical field. 7
It is best, of course, to avoid creating a septal defect in treating septal cysts, but in our patient the interventricular septum between the cystic cavity and the left ventricular cavity was thin and was bulging into the left ventricular outflow tract. We excised a small amount of septum without damage to the conductive tissue, the papillary muscles, or the mitral or aortic valves. Because the right part of the septum was thick, we were able to include the remnant of the cystic cavity with the left ventricular cavity, without use of a patch.
Supplemental medical treatment, other than with albendazole, is not widespread in the treatment of cardiac echinococcosis. 3 We used albendazole to prevent recurrence, but some instances of recurrence have been reported in patients treated with albendazole. 9 In conclusion, the treatment of hydatid cyst disease is surgical and should not be delayed. Gentle manipulation of the heart minimizes the risk of lethal complications, such as rupture and embolization. The patient should of course be examined for other cystic involvement.
Footnotes
Address for reprints: Omer Tetik, MD, Department of Cardiovascular Surgery, Ataturk Education and Research Hospital, 35360 Yesilyurt, Izmir, Turkey
References
- 1.Kammoun S, Frikha I, Fourati K, Fendri S, Benyoussef S, Sahnoun Y, et al. Hydatid cyst of the heart located in the interventricular septum. Can J Cardol 2000;16:921–4. [PubMed]
- 2.Matossian RM, Rickard MD, Smyth JD. Hydatidosis: a global problem of increasing importance. Bull World Health Organ 1977;55:499–507. [PMC free article] [PubMed]
- 3.Maroto LC, Carrascal Y, Lopez MJ, Forteza A, Perez A, Zavanella C. Hydatid cyst of the interventricular septum in a 3.5-year-old child. Ann Thorac Surg 1998;66:2110–1. [DOI] [PubMed]
- 4.Kaplan M, Demirtas M, Cimen S, Ozler A. Cardiac hydatid cysts with intracavitary expansion. Ann Thorac Surg 2001;71:1587–90. [DOI] [PubMed]
- 5.De Paulis R, Seddio F, Colagrande L, Polisca P, Chiariello L. Cardiac echinococcosis causing coronary artery disease. Ann Thorac Surg 1999;67:1791–3. [DOI] [PubMed]
- 6.Bennis A, Darif A, Mehadji BE, Chraibi N. Cardiac hydatid cyst revealed by complete heart block. Heart Vessels 2000;15:46–8. [DOI] [PubMed]
- 7.Eren EE, Aykut S, Kayihan A, Aydogan H, Dagsali S. Echinococcal cyst of the interventricular septum with right ventricular protrusion. Tex Heart Inst J 1989;16:292–5. [PMC free article] [PubMed]
- 8.Miralles A, Bracamonte L, Pavie A, Bors V, Rabago G, Gandjbakhch I, Cabrol C. Cardiac echinococcosis. Surgical treatment and results. J Thorac Cardiovasc Surg 1994;107:184–90. [PubMed]
- 9.Birincioglu CL, Bardakci H, Kucuker SA, Ulus AT, Arda K, Yamak B, Tasdemir O. A clinical dilemma: cardiac and pericardiac echinococcosis. Ann Thorac Surg 1999;68:1290–4. Comment in: Ozyazicioglu A, Kocak H, Becit N. Cardiac and pericardiac echinococcosis [letter]. Ann Thorac Surg 2000;70:1002–4. [DOI] [PubMed]