

To the Editor:
Since the inception of gastrointestinal cancer surgery, resection of the adjacent lymph nodes has been a standard part of the surgical approach. This is done to diminish the incidence of local-regional recurrence and also to improve survival. Without doubt, the resection of localized metastatic disease in lymph nodes is of benefit to patients. Also, in the 1970s, we learned that resection of liver metastases from colorectal cancer could be associated with cure of this condition. As larger number of patients were treated and the long-term survival rates evaluated, the selection criteria for hepatectomy for metastatic disease has evolved and has expanded. In my opinion, we are learning at the present time how to cure peritoneal surface dissemination (carcinomatosis) from gastrointestinal cancer. Pseudomyxoma peritonei (PMP) may be the paradigm by which to test a surgical management plan that establishes a curative outcome for peritoneal carcinomatosis.
I have pursued a curative approach to PMP since 1982. In my first publication, 5 of 14 patients with far advanced PMP were reported as disease-free between 2 and 4 years following cytoreductive surgery and intraperitoneal chemotherapy.1 Since then, I have treated about 800 appendiceal malignancy patients by a combined treatment.
The thesis of the article by Miner et al is that “absolute cure, defined as a prolonged disease-free state, is uncommon.” I am convinced that this conclusion offered by the group from Memorial Sloan-Kettering Cancer Center regarding their treatment of 97 patients over 22 years (management of approximate 2 patients per year) is a wrong conclusion.2 I am also convinced that their approach, which is serial debulking, is not beneficial to patients in the long term; rather, it makes combined treatment with cytoreductive surgery and intraperitoneal chemotherapy more difficult and sometimes impossible.
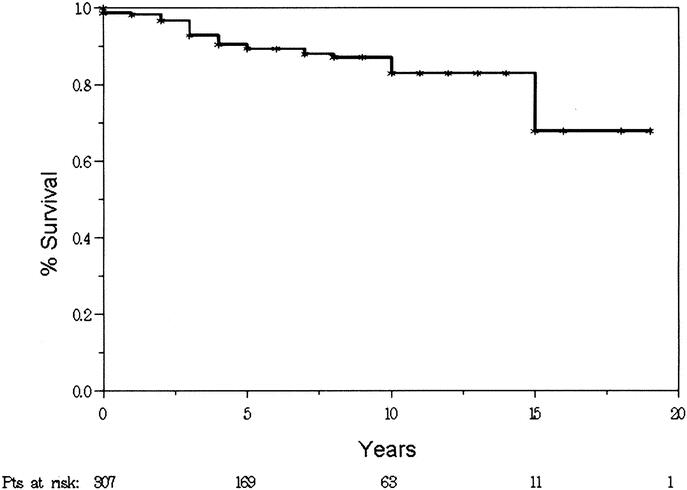
To test their thesis that cure was impossible in this disease, I selected from my database of PMP patients the most favorable group. These are patients with disseminated peritoneal adenomucinosis and a complete cytoreduction at the time of the first surgery here at the Washington Cancer Institute3 with a 70% 19-year survival of this group of patients (Fig. 1). At the Memorial Sloan-Kettering Cancer Center, patients had 2.2 operations per patient to remove gross disease without an effort to completely eradicate the disease process and with an absence of chemotherapy washing of the abdomen and pelvis. In my patients, there were 1.3 operations per patient utilizing cytoreductive surgery with peritonectomy. Perioperative intraperitoneal chemotherapy was used in all patients in an effort to eradicate residual microscopic disease.4,5
Figure.
Miner et al found 12 of 97 patients disease-free at the time this article was prepared. I would like to ask how many of their long-term survivors went to other peritoneal carcinomatosis treatment centers for definitive management using cytoreductive surgery and intraperitoneal. In reviewing our records, 7 patients previously treated at Memorial Sloan-Kettering Cancer Center came to the Washington Hospital Center with progressive PMP of appendiceal origin. It is possible that the Memorial Sloan-Kettering approach at serial debulking worked even more poorly than indicated in their Annals of Surgery article? Is it possible that all of their long-term survivors went to other treatment centers for a more definitive approach to this disease?
A similar outcome was reported in another natural history article written on PMP from the Mayo Clinic.6 Long-term survival was recorded, but few if any patients were cured. In this article, serial debulking was used in a majority of patients. However, a few received definitive local-regional treatments such as intraperitoneal 5-fluorouracil or intraperitoneal P32. In the patients treated with surgery plus a definitive intraperitoneal adjuvant, the survival (although not statistically significantly) was improved. A third natural history study reporting the long-term results with serial debulking was reported by Misdraji et al from the Massachusetts General Hospital.7
Recently, I reviewed the literature regarding cytoreductive surgery plus perioperative intraperitoneal chemotherapy from 7 institutions (Table 1). From these results, it seemed clear that this approach was being pursued at many institutions around the world.8–14 Has it become the standard of practice for this disease despite the lack of prospective and randomized trials? In my own mind, cytoreductive surgery plus intraperitoneal chemotherapy is a superior treatment that is associated with a 20% morbidity and 2% mortality. A curative approach to appendiceal malignancy with peritoneal dissemination may have implications to other gastrointestinal malignancies that develop carcinomatosis.15
TABLE 1. Literature Review of Cytoreductive Surgery and Perioperative Intraperitoneal Chemotherapy as a Treatment for Mucinous Appendiceal Tumors With Peritoneal Dissemination

Paul H. Sugarbaker, MD, FACS, FRCS
Program in Peritoneal Surface Malignancy
Washington, DC
paul.sugarbaker@medstar.net
REFERENCES
- 1.Sugarbaker PH, Kern K, Lack E. Malignant pseudomyxoma of colonic origin: natural history and presentation of a curative approach to treatment. Dis Colon Rectum. 1987;30:772–779. [DOI] [PubMed] [Google Scholar]
- 2.Miner TJ, Shida J, Jacques DP, et al. Long-term survival following treatment of pseudomyxoma peritonei: an analysis of surgical therapy. Ann Surg. 2005;241:300–308. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Sugarbaker PH, Ronnett BM, Archer A, et al. Pseudomyxoma peritonei syndrome. Adv Surg. 1996;30:233–280. [PubMed] [Google Scholar]
- 4.Sugarbaker PH. Peritonectomy procedures. Ann Surg. 1995;221:29–42. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Sugarbaker PH. Management of Peritoneal Surface Malignancy Using Intraperitoneal Chemotherapy and Cytoreductive Surgery: A Manual for Physicians and Nurses, 3rd ed. Grand Rapids, MI: Ludann, 1998. [Google Scholar]
- 6.Gough DB, Donohue JH, Schutt AJ, et al. Pseudomyxoma peritonei: long-term patient survival with an aggressive regional approach. Ann Surg. 1994;219:112–119. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Misdraji J, Yantiss RK, Graeme-Cook FM, et al. Appendiceal mucinous neoplasms: a clinicopathologic analysis of 107 cases. Am J Surg Pathol. 2003;27:1089–1103. [DOI] [PubMed] [Google Scholar]
- 8.Sugarbaker PH, Chang D. Results of treatment of 385 patients with peritoneal surface spread of appendiceal malignancy. Ann Surg Oncol. 1999;6:727–731. [DOI] [PubMed] [Google Scholar]
- 9.Witkamp AJ, Bree E, Kaag MM, et al. Extensive surgical cytoreduction and intraoperative hyperthermic intraperitoneal chemotherapy in patients with pseudomyxoma peritonei. Br J Surg. 2001;88:458–463. [DOI] [PubMed] [Google Scholar]
- 10.Piso P, Bektas H, Werner U, et al. Improved prognosis following peritonectomy procedures and hyperthermic intraperitoneal chemotherapy for peritoneal carcinomatosis from appendiceal carcinoma. Eur J Surg Oncol. 2001;27:286–290. [DOI] [PubMed] [Google Scholar]
- 11.Shen P, Levine EA, Hall J, et al. Factors predicting survival after intraperitoneal hyperthermic chemotherapy with mitomycin C after cytoreductive surgery for patients with peritoneal carcinomatosis. Arch Surg. 2003;138:26–33. [DOI] [PubMed] [Google Scholar]
- 12.Deraco M, Baratti D, Inglese MG, et al. Peritonectomy and intraperitoneal hyperthermic perfusion (IPHP): a strategy that has confirmed it efficacy in patients with pseudomyxoma peritonei. Ann Surg Oncol. 2004;11:393–398. [DOI] [PubMed] [Google Scholar]
- 13.Guner Z, Schmidt U, Dahlke MH, et al. Cytoreductive surgery and intraperitoneal chemotherapy for pseudomyxoma peritonei. Int J Colorectal Dis. 2004;20:155–160. [DOI] [PubMed] [Google Scholar]
- 14.Loungnarath R, Causeret S, Bossard N, et al. Cytoreductive surgery with intraperitoneal chemohyperthermia for the treatment of pseudomyxoma peritonei: a prospective study. In press. [DOI] [PubMed]
- 15.Glehen O, Kwiatkowski F, Sugarbaker PH, et al. Cytoreductive surgery combined with perioperative intraperitoneal chemotherapy for the management of peritoneal carcinomatosis from colorectal cancer: a multi-institutional study. J Clin Oncol. 2004;22:3284–3292. [DOI] [PubMed] [Google Scholar]