

Abstract
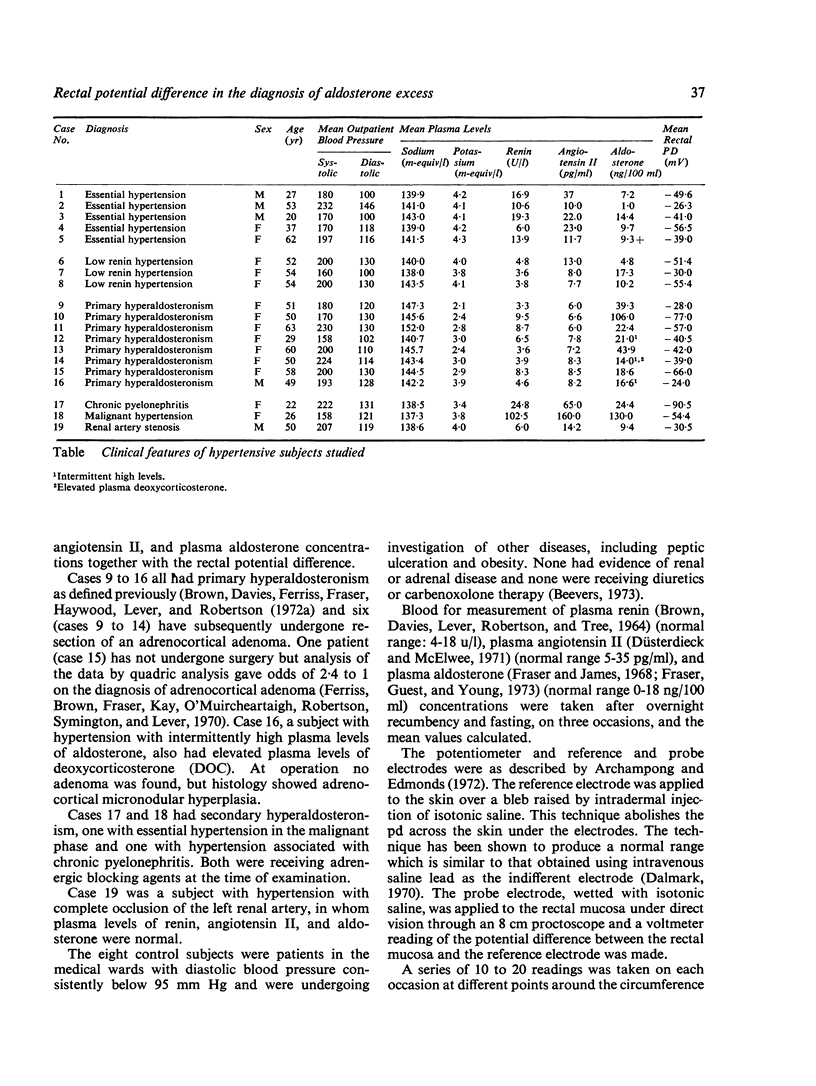
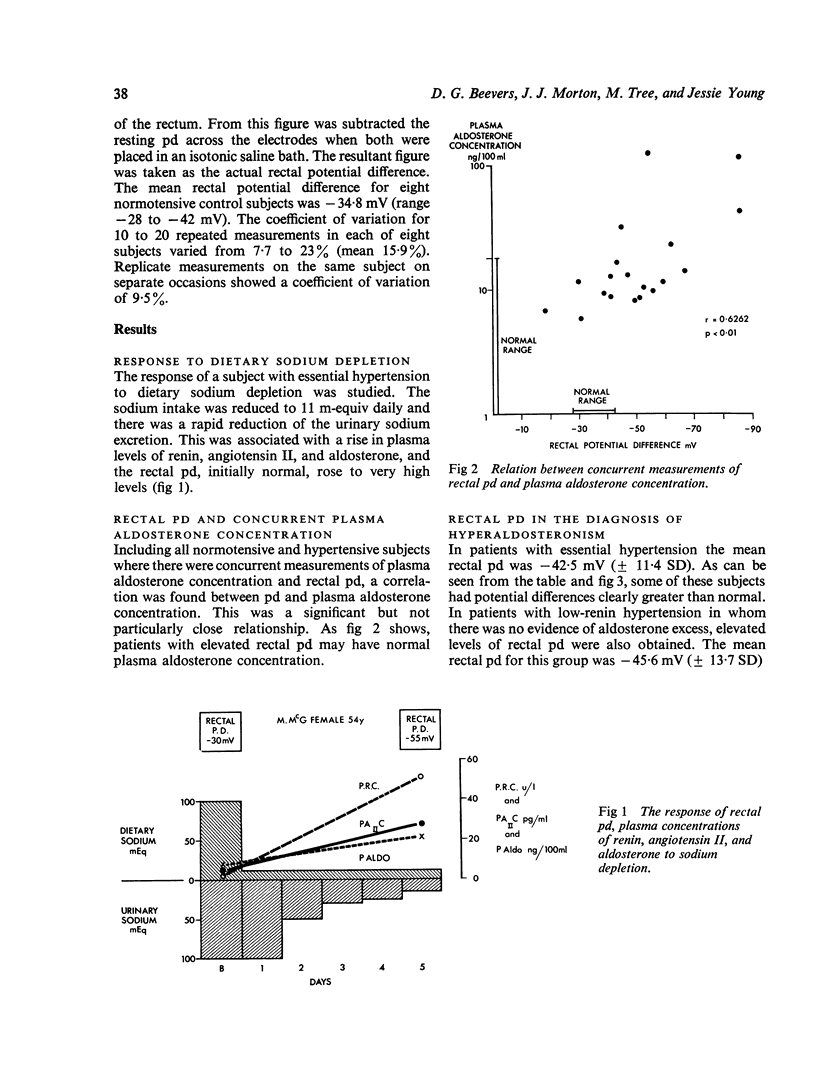
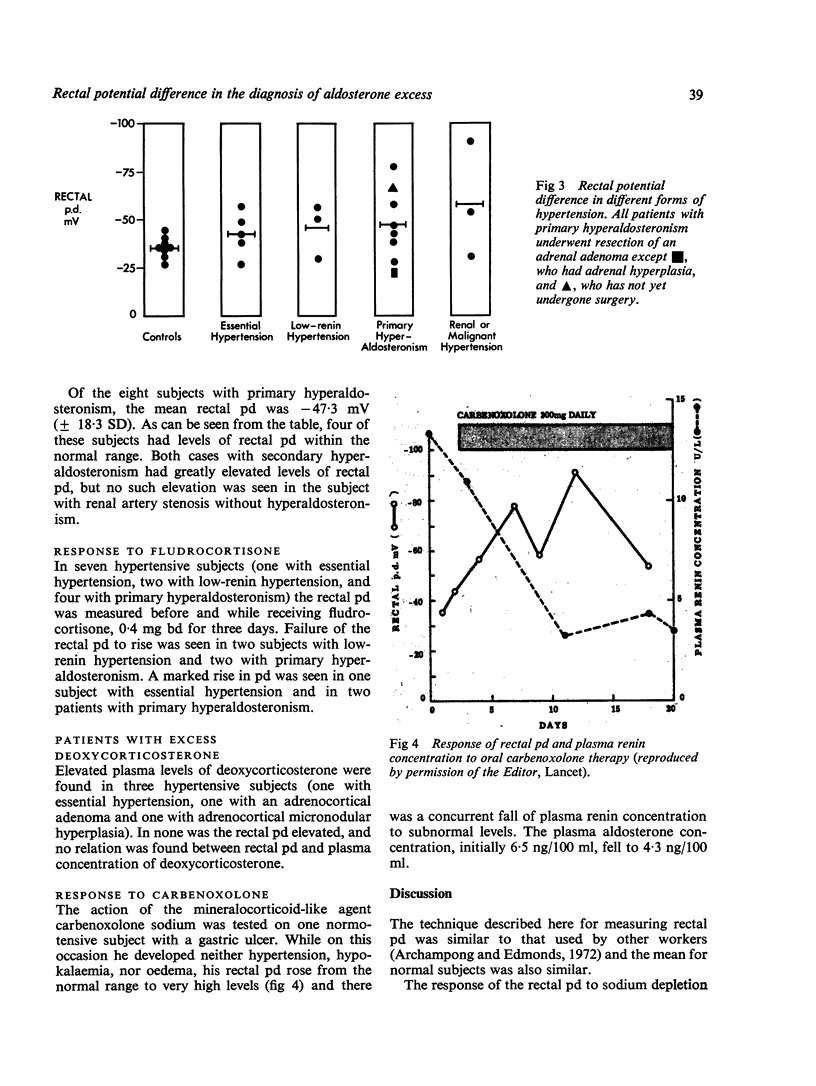
Rectal potential difference (pd) is directly related to the plasma aldosterone concentration, and rises when aldosterone is stimulated by sodium deprivation. However, when the measurement of rectal pd was tested at a screening test for hyperaldosteronism in 19 hypertensive subjects, four of the eight with primary hyperaldosteronism had a normal pd and four of the eight without aldosterone excess had an abnormally raised potential difference. The technique cannot therefore be recommended as a routine screening test for hyperaldosteronism. No relationship was found between rectal pd and hypertension associated with excess of deoxycorticosterone. Rectal pd rises in response to the mineralocorticoid-like agent carbenoxolone.
Full text
PDF
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Archampong E. Q., Edmonds C. J. Effect of luminal ions on the transepithelial electrical potential difference of human rectum. Gut. 1972 Jul;13(7):559–565. doi: 10.1136/gut.13.7.559. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Beevers D. G., Brown J. J., Ferriss J. B., Fraser R., Lever A. F., Robertson J. I. The use of spironolactone in the diagnosis and the treatment of hypertension associated with mineralocorticoid excess. Am Heart J. 1973 Sep;86(3):404–414. doi: 10.1016/0002-8703(73)90051-3. [DOI] [PubMed] [Google Scholar]
- Beevers D. G. Mineralocorticoids and rectal potential difference. Lancet. 1973 Sep 22;2(7830):682–683. doi: 10.1016/s0140-6736(73)92525-7. [DOI] [PubMed] [Google Scholar]
- Biglieri E. G., Slaton P. E., Jr, Kronfield S. J., Deck J. B. Primary aldosteronism with unusual secretory pattern. J Clin Endocrinol Metab. 1967 May;27(5):715–721. doi: 10.1210/jcem-27-5-715. [DOI] [PubMed] [Google Scholar]
- Biglieri E. G., Slaton P. E., Schambelan M., Kronfield S. J. Hypermineralocorticoidism. Am J Med. 1968 Aug;45(2):170–175. doi: 10.1016/0002-9343(68)90035-1. [DOI] [PubMed] [Google Scholar]
- Biglieri E. G., Stockigt J. R., Schambelan M. A preliminary evaluation for primary aldosteronism. Arch Intern Med. 1970 Dec;126(6):1004–1007. [PubMed] [Google Scholar]
- Brown J. J., Davies D. L., Ferriss J. B., Fraser R., Haywood E., Lever A. F., Robertson J. I. Comparison of surgery and prolonged spironolactone therapy in patients with hypertension, aldosterone excess, and low plasma renin. Br Med J. 1972 Jun 24;2(5816):729–734. doi: 10.1136/bmj.2.5816.729. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Brown J. J., Davies D. L., Lever A. F., Robertson J. I., Tree M. The estimation of renin in human plasma. Biochem J. 1964 Dec;93(3):594–600. doi: 10.1042/bj0930594. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Brown J. J., Fraser R., Love D. R., Ferriss J. B., Lever A. F., Robertson J. I., Wilson A. Apparently isolated excess deoxycorticosterone in hypertension. A variant of the mineralocorticoid-excess syndrome. Lancet. 1972 Aug 5;2(7771):243–247. doi: 10.1016/s0140-6736(72)91685-6. [DOI] [PubMed] [Google Scholar]
- CONN J. W., COHEN E. L., ROVNER D. R., NESBIT R. M. NORMOKALEMIC PRIMARY ALDOSTERONISM. A DETECTABLE CAUSE OF CURABLE "ESSENTIAL" HYPERTENSION. JAMA. 1965 Jul 19;193:200–206. doi: 10.1001/jama.1965.03090030022005. [DOI] [PubMed] [Google Scholar]
- CONN J. W. Presidential address. I. Painting background. II. Primary aldosteronism, a new clinical syndrome. J Lab Clin Med. 1955 Jan;45(1):3–17. [PubMed] [Google Scholar]
- Charron R. C., Leme C. E., Wilson D. R., Ing T. S., Wrong O. M. The effect of adrenal steroids on stool composition, as revealed by in vivo dialysis of faeces. Clin Sci. 1969 Aug;37(1):151–167. [PubMed] [Google Scholar]
- Dalmark M. The transmucosal electrical potential difference of rectum in the unanesthetized man. Scand J Gastroenterol. 1970;5(4):277–282. [PubMed] [Google Scholar]
- Düsterdieck G., McElwee G. Estimation of angiotensin II concentration in human plasma by radioimmunoassay. Some applications to physiological and clinical states. Eur J Clin Invest. 1971 Nov;2(1):32–38. doi: 10.1111/j.1365-2362.1971.tb00565.x. [DOI] [PubMed] [Google Scholar]
- Edmonds C. J., Cronquist A. A simple millivoltmeter and electrodes for measurement of rectal electrical potential in man. Med Biol Eng. 1970 Jul;8(4):409–410. doi: 10.1007/BF02477670. [DOI] [PubMed] [Google Scholar]
- Edmonds C. J., Godfrey R. C. Measurement of electrical potentials of the human rectum and pelvic colon in normal and aldosterone-treated patients. Gut. 1970 Apr;11(4):330–337. doi: 10.1136/gut.11.4.330. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Edmonds C. J., Richards P. Measurement of rectal electrical potential difference as an instant screening-test for hyperaldosteronism. Lancet. 1970 Sep 26;2(7674):624–627. doi: 10.1016/s0140-6736(70)91397-8. [DOI] [PubMed] [Google Scholar]
- Ferriss J. B., Brown J. J., Fraser R., Kay A. W., Neville A. M., O'Muircheartaigh I. G., Robertson J. I., Symington T., Lever A. F. Hypertension with aldosterone excess and low plasma-renin: preoperative distinction between patients with and without adrenocortical tumour. Lancet. 1970 Nov 14;2(7681):995–1000. doi: 10.1016/s0140-6736(70)92811-4. [DOI] [PubMed] [Google Scholar]
- Fraser R., Guest S., Young J. A comparison of double-isotope derivative and radioimmunological estimation of plasma aldosterone concentration in man. Clin Sci Mol Med. 1973 Sep;45(3):411–415. doi: 10.1042/cs0450411. [DOI] [PubMed] [Google Scholar]
- Fraser R., James V. H. Double isotope assay of aldosterone, corticosterone and cortisol in human peripheral plasma. J Endocrinol. 1968 Jan;40(1):59–72. doi: 10.1677/joe.0.0400059. [DOI] [PubMed] [Google Scholar]
- LEVITAN R., INGELFINGER F. J. EFFECT OF D-ALDOSTERONE ON SALT AND WATER ABSORPTION FROM THE INTACT HUMAN COLON. J Clin Invest. 1965 May;44:801–808. doi: 10.1172/JCI105192. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ledingham J. G., Bull M. B., Laragh J. H. The meaning of aldosteronism in hypertensive disease. Circ Res. 1967 Jul;21(1 Suppl):177+–177+. [PubMed] [Google Scholar]
- MCCONAHAY T. P., ROBINSON S., NEWTON J. L. D-ALDOSTERONE AND SWEAT ELECTROLYTES. J Appl Physiol. 1964 Jul;19:575–579. doi: 10.1152/jappl.1964.19.4.575. [DOI] [PubMed] [Google Scholar]
- Richards P. Clinical investigation of the effects of adrenal corticosteroid excess on the colon. Lancet. 1969 Mar 1;1(7592):437–442. doi: 10.1016/s0140-6736(69)91480-9. [DOI] [PubMed] [Google Scholar]
- Richards P., Jones M. B., Peart W. S. Periodic hypokalaemic paralysis, adrenal adenoma, and normal colonic transport of sodium and potassium. Gut. 1973 Jun;14(6):478–484. doi: 10.1136/gut.14.6.478. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Richards P. Letter: mineralocorticoids and rectal potential difference. Lancet. 1973 Oct 6;2(7832):798–799. doi: 10.1016/s0140-6736(73)91071-4. [DOI] [PubMed] [Google Scholar]
- WRONG O., METCALFE-GIBSON A., MORRISON R. B., NG S. T., HOWARD A. V. IN VIVO DIALYSIS OF FAECES AS A METHOD OF STOOL ANALYSIS. I. TECHNIQUE AND RESULTS IN NORMAL SUBJECTS. Clin Sci. 1965 Apr;28:357–375. [PubMed] [Google Scholar]
- Wotman S., Goodwin F. J., Mandel I. D., Laragh J. H. Changes in salivary electrolytes following treatment of primary aldosteronism. Arch Intern Med. 1969 Oct;124(4):477–480. [PubMed] [Google Scholar]