

Abstract
Few reported cases document injury to the circumflex coronary artery secondary to repair of the mitral valve annulus. This potentially life-threatening sequela must be considered during mitral valve repair. In an effort to increase awareness of this sequela, we present the case of a patient who experienced a perioperative myocardial infarction secondary to injury of the circumflex coronary artery after mitral valve repair.
Few reported cases document injury to the circumflex coronary artery secondary to repair of the mitral valve annulus.1–6 Danielson and coworkers6 were the first to report such a finding. This potentially life-threatening sequela must be considered during mitral valve repair. In an effort to increase awareness of this sequela, we present the case of a patient who experienced a perioperative myocardial infarction secondary to injury of the circumflex coronary artery after mitral valve repair.
Case Reports
In November 2004, a 27-year-old woman was admitted for elective aortic root repair. Six years earlier, she had been diagnosed with Marfan syndrome, and she had been monitored on a regular basis thereafter. Her mother had manifested Marfan syndrome, complicated by aortic dissection at an early age.
One month before this admission, our patient had been admitted with chest discomfort and left scapular pain. At that time, electrocardiography (ECG) demonstrated normal sinus rhythm, and cardiac enzyme testing ruled out myocardial infarction. An echocardiogram revealed a slightly dilated left ventricle with borderline concentric left ventricular hypertrophy, but normal wall motion. At that time, she was also found to have moderate mitral valve prolapse (4+ anteriorly directed mitral regurgitation) that was consistent with posterior leaflet disease. The sinotubular junction and sinus aorta measured 4.3 cm. The aortic annulus was not dilated. A computed tomographic scan showed an aortic root of 4.5 cm with no evidence of dissection. She had been discharged from the hospital and had experienced no further episodes of chest pain.
Intraoperative transesophageal echocardiography (TEE) confirmed 4+ mitral regurgitation with an anteriorly directed jet. After the aortotomy, the patient was found to have 4.5-cm aneurysmal dilatation of the sinuses of Valsalva with a normal annulus, for which we performed a valve-sparing aortic root replacement (Yacoub procedure) with a 24-mm Vascutek gel weave sinus of Valsalva graft (Sulzer Medica; Hamburg, Germany). Inspection of the mitral valve revealed a floppy, redundant P2 portion of the posterior leaflet. We performed a quadrangular resection of P2, with posterior annulus plication using the McGoon technique, and then implanted a 34-mm Cosgrove annuloplasty band (Edwards Lifesciences; Irvine, Calif). After the repair, TEE showed normal aortic valve function with no aortic insufficiency, a trace of mitral regurgitation, and a 3-mm transmitral gradient. The patient was weaned from cardiopulmonary bypass without incident and without the need for inotropic support. She was then transferred to the cardiovascular intensive care unit with stable vital signs, on nitroglycerin and propofol, and was extubated within 6 hours.
After 2 hours in the intensive care unit, the patient was noted to have ST elevation in the inferior leads. The MB isoenzyme of creatine kinase (CK-MB) was 133 ng/mL, and troponin I was 32.7 ng/mL. She remained hemodynamically stable and was continued on a nitroglycerin infusion. Her creatine phosphokinase level peaked at 4,707 U/L, CK-MB at 183 ng/mL, creatine kinase index at 4.2%, and troponin I at >50 ng/mL. On postoperative day 1, the ST changes had resolved, but the ECG showed a 1st-degree atrioventricular block. Low-dose β-blockers were added to her regimen. No Q-waves were seen. Repeat echocardiography revealed mild left ventricular hypertrophy, 1+ mitral regurgitation with a posterior jet, and a small area of inferior hypokinesis. Cardiac catheterization performed on postoperative day 1 revealed a left-dominant system with a left circumflex coronary artery (CCA) that was dynamically distorted (Figs. 1 and 2), displaying systolic occlusion and diastolic intermittent flow with some distal collaterals. Percutaneous intervention was attempted, and we were able to pass a wire though the lesion. Due to the acute angle, we could not pass a balloon angioplasty catheter through the lesion over the wire. The patient remained free of angina and was treated medically. The rest of her hospital stay was uneventful, with no further episodes of chest pain or ECG changes. She was discharged on postoperative day 10.
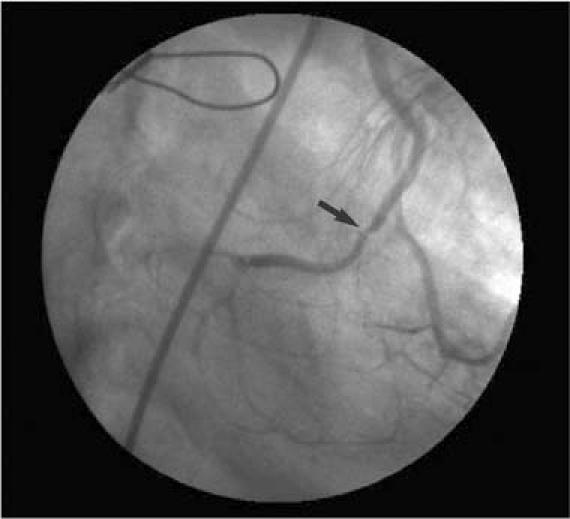
Fig. 1 Left main injection coronary angiogram during diastole. Partial occlusion of the left-dominant circumflex coronary artery is shown (arrow) in proximity to the mitral annulus repair. This occlusion is dynamic and becomes complete during systole.

Fig. 2. Left main injection coronary angiogram during systole. Complete occlusion of the left-dominant circumflex artery is shown (arrow).
Discussion
Due to its variable anatomy and proximity to the mitral valve annulus, the CCA is prone to injury during mitral valve repair or replacement. Anatomic studies2 have documented that the distance between the mitral valve annulus and the CCA can be as little as 1 mm. Tavilla and Pacini1 found that the risk of injury to the CCA is augmented in co-dominant or left-dominant anatomy. They suggested that preoperative angiography be mandatory in all patients before they undergo mitral valve repair, to evaluate the dominance of the coronary system and the course of the CCA.1 It has also been suggested that intraoperative TEE decreases mortality rates by identifying new wall-motion abnormalities.5,6
Unfortunately, the injury was not identified intraoperatively in our patient. In retrospect, we believe that a malpositioned suture used for reconstruction of a P2 quadrangular resection defect resulted in traction on tissue adjacent to the circumflex coronary artery, which produced dynamic occlusion.
Care must be taken to avoid damaging the CCA, not only by means of a thorough knowledge of the patient's anatomy, but also by meticulous technique. Awareness must be raised to prevent possible future occurrences of this potentially lethal sequela.
Footnotes
Address for reprints: Michael A. Wait, MD, Department of Cardiovascular and Thoracic Surgery, University of Texas Southwestern Medical Center, 5323 Harry Hines Boulevard, Dallas, TX 75390
E-mail: michael.wait@utsouthwestern.edu
Dr. Meursing is now at the Albert Einstein Medical Center, Philadelphia, Pennsylvania.
References
- 1.Tavilla G, Pacini D. Damage to the circumflex coronary artery during mitral valve repair with sliding leaflet technique. Ann Thorac Surg 1998;66:2091–3. [DOI] [PubMed]
- 2.Morin D, Fischer AP, Sohl BE, Sadeghi H. Iatrogenic myocardial infarction. A possible complication of mitral valve surgery related to anatomical variation of the circumflex coronary artery. Thorac Cardiovasc Surg 1982;30:176–9. [DOI] [PubMed]
- 3.Kaklikkaya I, Yeginoglu G. Damage to coronary arteries during mitral valve surgery. Heart Surg Forum 2003;6:E138–42. [PubMed]
- 4.Cornu E, Lacroix PH, Christides C, Laskar M. Coronary artery damage during mitral valve replacement. J Cardiovasc Surg (Torino) 1995;36:261–4. [PubMed]
- 5.Virmani R, Chun PK, Parker J, McAllister HA Jr. Suture obliteration of the circumflex coronary artery in three patients undergoing mitral valve operation. Role of left dominant or codominant coronary artery. J Thorac Cardiovasc Surg 1982;84:773–8. [PubMed]
- 6.Danielson GK, Cooper E, Tweedale DN. Circumflex coronary artery injury during mitral valve replacement. Ann Thorac Surg 1967;4:53–9.