

Abstract
Objective
To determine whether a low-bandwidth Internet connection can provide adequate image quality to support remote real-time surgical consultation.
Summary Background Data
Telemedicine has been used to support care at a distance through the use of expensive equipment and broadband communication links. In the past, the operating room has been an isolated environment that has been relatively inaccessible for real-time consultation. Recent technological advances have permitted videoconferencing over low-bandwidth, inexpensive Internet connections. If these connections are shown to provide adequate video quality for surgical applications, low-bandwidth telemedicine will open the operating room environment to remote real-time surgical consultation.
Methods
Surgeons performing a laparoscopic cholecystectomy in Ecuador or the Dominican Republic shared real-time laparoscopic images with a panel of surgeons at the parent university through a dial-up Internet account. The connection permitted video and audio teleconferencing to support real-time consultation as well as the transmission of real-time images and store-and-forward images for observation by the consultant panel. A total of six live consultations were analyzed. In addition, paired local and remote images were “grabbed” from the video feed during these laparoscopic cholecystectomies. Nine of these paired images were then placed into a Web-based tool designed to evaluate the effect of transmission on image quality.
Results
The authors showed for the first time the ability to identify critical anatomic structures in laparoscopy over a low-bandwidth connection via the Internet. The consultant panel of surgeons correctly remotely identified biliary and arterial anatomy during six laparoscopic cholecystectomies. Within the Web-based questionnaire, 15 surgeons could not blindly distinguish the quality of local and remote laparoscopic images.
Conclusions
Low-bandwidth, Internet-based telemedicine is inexpensive, effective, and almost ubiquitous. Use of these inexpensive, portable technologies will allow sharing of surgical procedures and decisions regardless of location. Internet telemedicine consistently supported real-time intraoperative consultation in laparoscopic surgery. The implications are broad with respect to quality improvement and diffusion of knowledge as well as for basic consultation.
Telemedicine has been used to support care at a distance through the use of expensive equipment and broadband communication links. In the past, the operating room has been an isolated environment that has been relatively inaccessible for real-time consultation. Recent technological advances have permitted videoconferencing over low-bandwidth, inexpensive Internet connections. If these connections are shown to provide adequate video quality for surgical applications, low-bandwidth telemedicine will revolutionize surgical practice by enabling remote real-time surgical consultation.
Many of the regions around the world that have the most need for advanced surgical mentoring can least afford it. Although expensive broadband network links such as integrated services digital network (ISDN), local area networks (LANs), and dedicated T-1 lines have provided ample throughput for acceptable video image quality in recent years, the Internet has opened new doors for inexpensive alternatives. Early work by NASA demonstrated the usefulness of the Internet for telemedicine applications. 1 Similar work was also conducted using plain old telephone system (POTS) from the jungles of Ecuador. 2 In both cases, low bandwidth proved to be very useful for telemedicine applications. Internet-2 has been shown to provide high-resolution images, 3 but Internet-2 is simply another broadband technology, which will not be broadly available in the foreseeable future in most regions of the world. By using the ordinary telephone and a dial-up account to a local or global Internet service provider (ISP), a reliable remote node network can be established easily and affordably. The Internet has been successfully shown to be a useful and effective tool in supporting telemedicine on an international scale. 4,5
Over low-bandwidth connections such as dial-up, many Internet applications such as e-mail or web browsing are completely adequate. However, transmitting video over this type of connection is more difficult because of the synchronous data transfer rate and high degrees of compression. A series of experiments were performed to determine whether the quality of video images transmitted over Internet protocol (IP) connections were adequate to support surgical applications.
METHODS
Several technologies and telecommunications connections were used in this project to connect distant operating rooms to our teleconferencing system at the Medical College of Virginia (MCV) campus of Virginia Commonwealth University (VCU).
Surgical procedures were performed in operating rooms in a mobile operating facility in Ecuador, a hospital in the Dominican Republic, and at MCV/VCU. Through a partnership with the Cinterandes Foundation in Ecuador, a truck was converted into a mobile operating room (Fig. 1). This mobile operating room and a small team of surgeons and nurses have the ability to travel to remote regions of Ecuador and to interact with surgeons located at distant sites. Through Operation Helping Hands, similar partnerships with the Hospital de Leopoldo Pou in Samana, Dominican Republic, and the Rotary Club of Samana were also established. In all of these locations, a rapidly deployable telemedicine unit (RDTU) was used to capture and route the video from both the laparoscopic and external cameras. The RDTU is a portable, self-contained telecommunications, computing, and medical peripheral system that can be used anywhere in the world. It supports multiple communication topologies, including satellite capability. The single carry-case is small enough to be an airline carry-on. A Java-based composite control module permits an intuitive interface to various medical devices and tools. The RDTU is completely standards-compliant and supports both store-and-forward and real-time telemedicine using ISDN and IP videoconferencing protocols. Standard laparoscopic equipment (Stryker Endoscopy, Santa Clara, CA) was used as the source for all laparoscopic images.

Figure 1. Cinterandes’ mobile surgical facility.
In Ecuador, we used existing POTS lines (33.6K bps) to establish telecommunications connections. In the Dominican Republic, we used both POTS lines and an Inmarsat M4 satellite phone (maximum connection speed 64K bps). In Richmond, we used the existing 10/100 Ethernet LAN (10M bps) for transmission of video and voice within the university.
The central site in all cases was the teleconferencing laboratory at the Medical Informatics and Technology Applications Consortium (MITAC) at VCU. MITAC standard desktop computers running Windows operating systems were used, as well as a 20-square-foot projection screen to accommodate larger audiences.
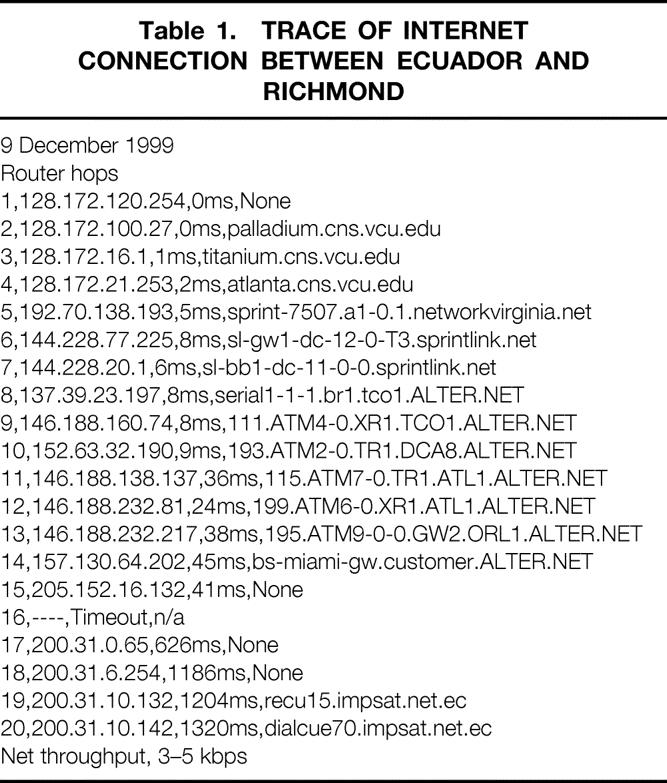
In Ecuador, the mobile surgical facility surgeons and nurses traveled 10 hours to Sucua, approximately 150 km east of Cuenca, over mountainous terrain and washed-out dirt roads. The mobile surgical facility was linked to the small medical center in Sucua by two phone lines. One line was connected to the RDTU equipped with a 56K modem; the second line was connected to a speakerphone for audio backup. Using a local dial-up Internet account, surgeons in Sucua connected to an Intel Teamstation in the MITAC telemedicine laboratory at MCV/VCU. The Internet connection was traced for line quality, router hops, and net throughput (Table 1).
Table 1. TRACE OF INTERNET CONNECTION BETWEEN ECUADOR AND RICHMOND
While the connection was in place, a surgeon located in the mobile surgical facility performed a laparoscopic cholecystectomy. Video was transmitted to VCU in real time. Video transmission alternated between an exterior view and a laparoscopic view using the s-video interface on a Nogatech Card directly out of the back of the Sony laparoscopic monitor. Surgeons at VCU were asked to identify anatomic structures over this low-bandwidth Internet connection. Images were projected onto a 20-square-foot screen in the MITAC telemedicine laboratory at VCU using a Sanyo MT1035+ liquid crystal display projector (Fig. 2). Still images were also transferred over the Internet connection via file transfer protocol (FTP) during the operation to confirm identification of fine anatomic structures obscured as a result of the extremely high compression of H.323 video over POTS (Fig. 3). In all instances, fully credentialed surgical faculty were in the field and on the panel. The work in Ecuador and the Dominican Republic was fully sanctioned by the Ministers of Health of Ecuador and the Dominican Republic. U.S. surgeons augmented fully trained and credentialed surgical teams in the field. Patients gave written consent for photography and surgical procedures.

Figure 2. Intel Teamstation in the MITAC telemedicine laboratory.
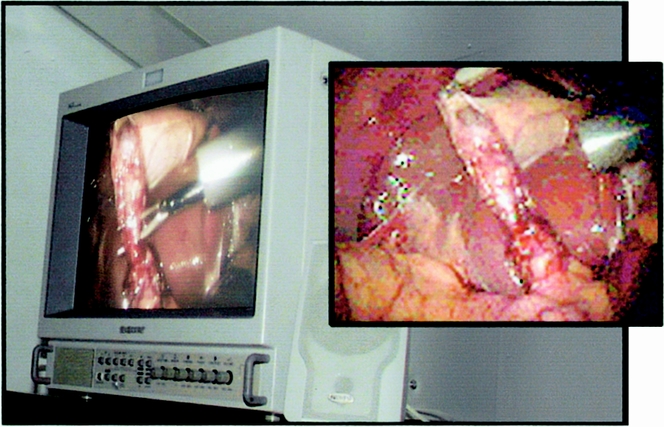
Figure 3. Local on laparoscopic monitor with matching images sent by FTP from Ecuador to MCV-VCU.
Through an affiliation with Operation Helping Hands, the feasibility of remote proctoring of laparoscopic procedures was further evaluated. Five laparoscopic cholecystectomies were performed by VCU surgeons in the Hospital de Leopoldo Pou in Samana, Dominican Republic. Remote surgeons at VCU were consulted to confirm critical information via an IP video connection. To evaluate further the effect of transmitting laparoscopic video images, five paired local and remote digital still images were “grabbed” from the video feed. The local and remote images were captured using a simple “copy/paste” command from Microsoft’s NetMeeting to Paint Shop Pro. In addition to the paired images obtained from the Dominican Republic using POTS or satellite connections, four additional image pairs were obtained during a laparoscopic gastric bypass performed at MCV/VCU and remotely viewed via the university LAN. Both series of captures used IP and H.323.
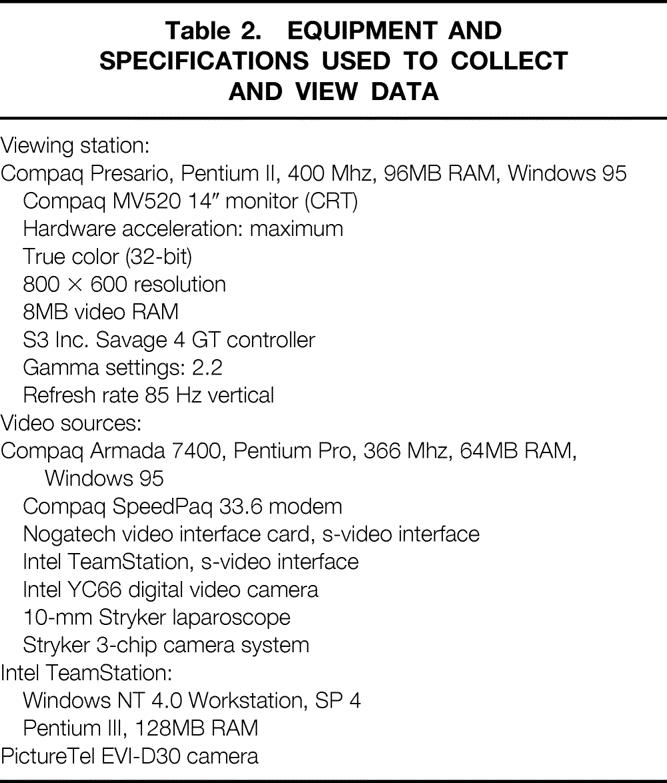
Nine of these paired images were then placed into a Web-based interface, back-ended by a Microsoft Access database designed to evaluate the effect of transmission on image quality. On this Web page (http://www.meditac.com/visualtest), the images were presented in a blinded fashion and surgeons were asked to evaluate the images with regard to their ability to identify captured images, the quality of the images (scale 1 [poor] to 10 [excellent]), and whether surgeons would feel comfortable in using these images to perform or remotely proctor surgery. A single image pair from the Web-based questionnaire is illustrated in Figure 4. Table 2 highlights the equipment used to accomplish the tasks.
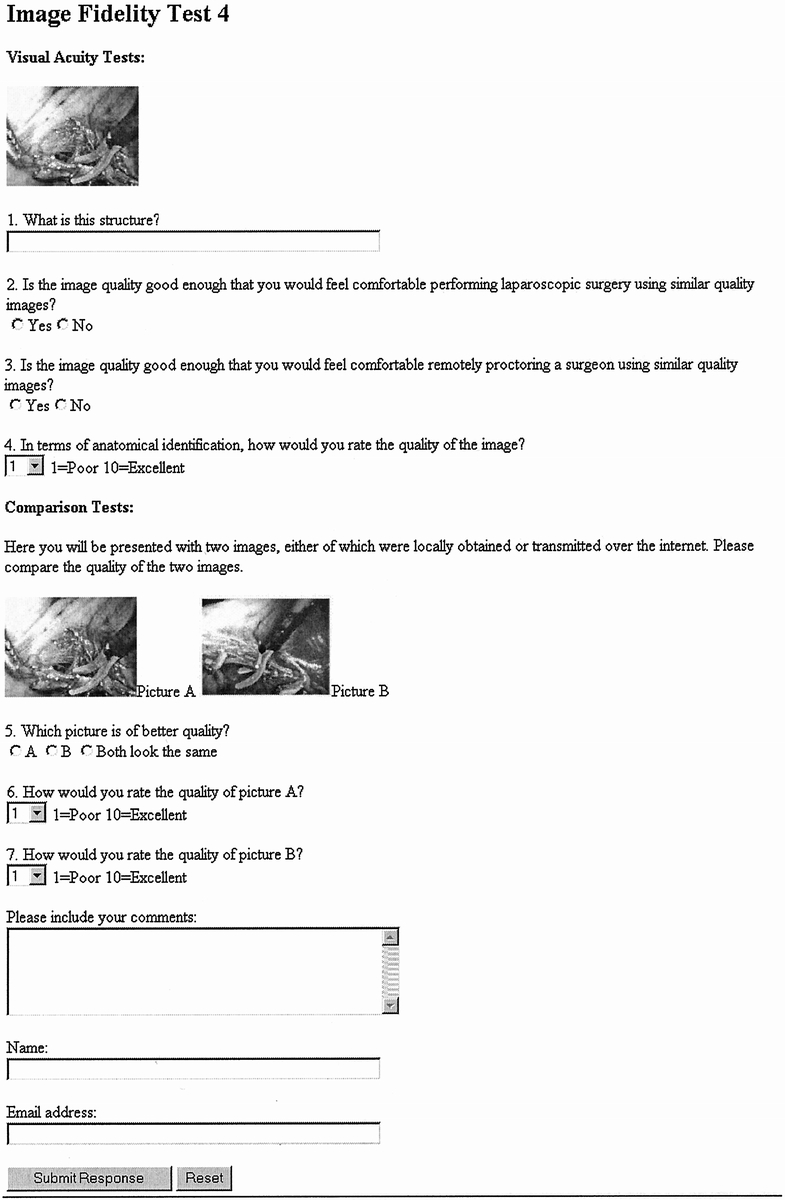
Figure 4. Web-based evaluation tool.
Table 2. EQUIPMENT AND SPECIFICATIONS USED TO COLLECT AND VIEW DATA
RESULTS
As the laparoscopic cholecystectomy proceeded in Sucua, surgeons at VCU were able to identify correctly the cystic duct and cystic artery via a low-bandwidth IP video connection. Anatomy was confirmed before surgical clips were applied. Identification and confirmation of fine anatomic detail were accomplished using still images sent via FTP. The time for consultation and confirmation was less than 5 minutes.
Subsequently, surgeons in Samana were successfully advised by surgeons at VCU during five laparoscopic cholecystectomies via a low-bandwidth POTS or satellite phone IP video connection. The remote surgeons confirmed the critical anatomy before the local surgeons continued the operation by application of the surgical clip. Using the Web-based questionnaire, 15 surgeons determined that the remote and local images were of similar quality (Figs. 5 and 6). Interestingly, although the surgeons were able to proctor these procedures remotely, the static images “grabbed” during these cholecystectomies were not thought to be adequate to remotely perform or proctor laparoscopic cholecystectomies when viewed out of context within the Web-based questionnaire. Of the 15 surgeons who participated in this study, 69% reported they would not feel comfortable using similar-quality images to perform laparoscopic surgery. In addition, 68% of these surgeons reported they would not feel comfortable remotely proctoring surgeons using images of similar quality. These data emphasized the importance of image context in laparoscopic surgery. There was no significant difference between the quality of remote images that were transmitted by LAN or lower-bandwidth connections.
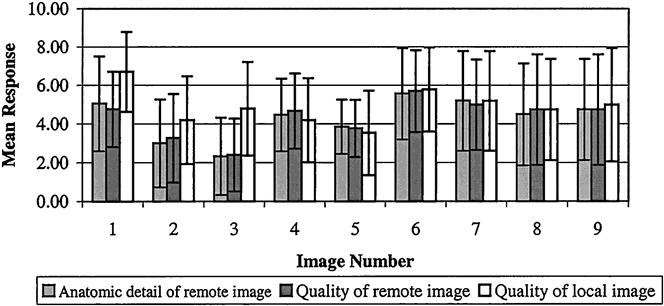
Figure 5. The quality of juxtaposed remote and local images on a scale of 1 (poor) to 10 (excellent) as evaluated by fifteen surgeons. Anatomical detail of the remote image was separately evaluated.
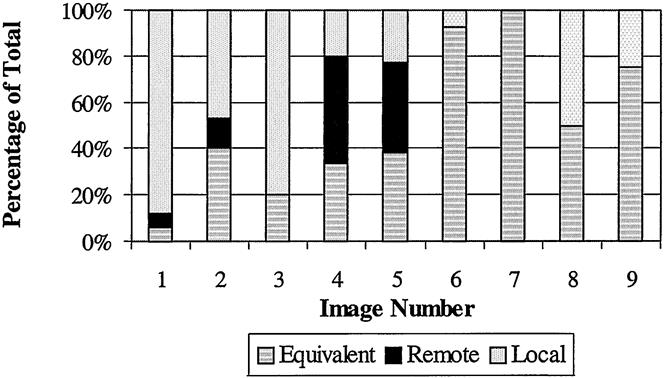
Figure 6. Comparison of juxtaposed remote and local images. An average of 15 surgeons responding to “Which picture is of better quality?”
DISCUSSION
The investigators have clinically evaluated real-time consulting for laparoscopic procedures under a variety of transmission bandwidths. This work is the first to show that identification of anatomic structures is possible via a low-bandwidth Internet connection. We also showed that low-bandwidth telementoring of laparoscopic procedures is possible. The use of lower bandwidths requires approximately 16 seconds for the image to achieve medically useful quality; nevertheless, all anatomic structures were confirmed in less than 5 minutes.
These experiments also showed that the context of images is important in laparoscopic surgery. Although surgeons were successful in remotely proctoring laparoscopic cholecystectomies, they did not feel comfortable identifying anatomic structures when presented with still images from procedures that had been previously proctored. Further experiments are planned to evaluate the effect of image context and surgeon experience in performing and proctoring remote laparoscopic surgery.
The ability to use smaller laparoscopes under low-bandwidth conditions will have to be evaluated. Smaller-diameter laparoscopes are important because they allow surgeons to perform operations under local anesthesia. Although we showed that the image quality provided by smaller laparoscopes is slightly worse than that provided by larger ones, the field of view of the picture also decreases with decreasing scope diameter. The limitations of small-diameter laparoscopes could be significant enough to preclude their use over low-bandwidth connections.
As mentioned earlier, telecommunications in many parts of the world, particularly underdeveloped nations, are not widely available or reliable. 6 In Sucua, POTS lines permitted a 33.6K bps connection to the ISP. However, we did have some problems with authentication at the ISP, and several attempts were required for successful connect. Once the link was established, we were able to videoconference using NetMeeting, send e-mail, send images via FTP, and use network tools. The connection required 20 “hops” (level 3 devices such as routers) with average latency values of 18 ms for the U.S. terrestrial links and delays of more than 1 second per hop for intercontinental links, which used satellite (see Table 1). These delays typically negatively affect audio; therefore, a second line was used successfully for voice communication.
In Samana, telephone service was intermittent. During the second day, the phones could not make any outbound calls, although outside parties could call in. During the loss of POTS, the portable satellite phone was used for IP communications. Because the Inmarsat AOR-W satellite was nearly directly overhead, the antenna was positioned on the roof of the single-story operating room without obstruction. Connection to the satellite was straightforward and reliable. Although the bandwidth for the portable satellite phone was nearly double that of a 33.6K POTS/modem connection, audio was again facilitated by use of a normal telephone call to ensure reliable voice communications. Although studies have shown that 64K bps is adequate for many telemedicine applications, increased fidelity in videoconferencing requires increased bandwidth. 7
As previously mentioned, it is often necessary to use a telephone to enable reliable voice communications as a result of the vagaries of the Internet and more specifically H.323 videoconferencing. Dropped video frames can be tolerated during a videoconference, but dropped audio is not well tolerated. 8 Further, disabling audio over an H.323 link allows more bandwidth for video transmission.
Use of inexpensive, portable, low-bandwidth videoconferencing systems will permit widespread teleproctoring of surgical procedures and diagnosis in the near future. Similar work recently showed successful low-bandwidth transmission of ultrasound images. 9 As widespread application of low-bandwidth videoconferencing will have a positive impact on the practice of medicine in the coming years, it is important to have a rudimentary understanding of how video is transferred over the Internet.
Videoconferencing software, which uses IP (such as Microsoft NetMeeting and White Pine CU-SeeMe), uses a different method of data transfer than a “traditional” transfer control protocol/internet protocol (TCP/IP) application such as a Web browser. In the familiar TCP protocol, several communications are made from system to system to verify that data have been received properly, which allows for error-correction and ensuring the integrity of data transmitted. This is necessary because of the packet-switched nature of IP and the fact that occasionally packets of data are misrouted or lost. It would not be acceptable, for example, that a text e-mail sent over IP should simply lose or misdirect the last 50 words, so this error-correction is necessary to make IP communications effective. In contrast, when sending video or audio data, it is not imperative that every byte be perfectly preserved: if 95% of the data are transferred properly, the recipient may still understand the message communicated, the same as on a phone line with static in the background.
Because TCP transmits so many verifications of data, it costs a significant amount of overhead for communications to take place. If you remove the overhead of error-correction from the audio and video communications, additional bandwidth is available for data. This is how current videoconferencing works, using the real-time transport protocol (RTP) over user datagram protocol (UDP). It is a far more efficient way of sending data in an IP environment, but it does so with the knowledge that some data will be lost in transmission.
The likelihood of any given packet of data being lost or misdirected is no greater than under any other protocol, meaning that it is subject to the same variable circumstances of line noise, timeouts, excessive routing, and malicious packet removal. In general, it is safe to assume that the greater the number of systems between points on a RTP/UDP connection, as well as the greater geographic distance, the more likely it is that packets will be lost with greater frequency. In addition, the quality of network and phone services on any branch of the connecting network will greatly affect the frequency of data loss, so that poor telecommunications systems may be incapable of establishing a reasonable RTP/UDP connection, whereas a good network may have no packet loss whatsoever.
Although most network protocols have error-correction in static data transfer, synchronous compressed video typically does not. In circumstances where the sending and receiving locations are in close proximity and connected by a broadband connection, the image quality is nearly identical. However, when distant locations are connected by lower-band connections, the lack of error-correction will be noticed as subtle changes in image quality. Figure 4 illustrates these phenomena. In this image pair, an M4 Inmarsat satellite phone was brought into the Ecuadorian jungle to a small clinic. The pictures show the slight image degradation as a result of the latency and packet loss caused by the nearly 50,000-mile round trip via a geostationary satellite. Notice the slight blurring, as well as the fact that the second hand is not visible in the remote image (Fig. 7).
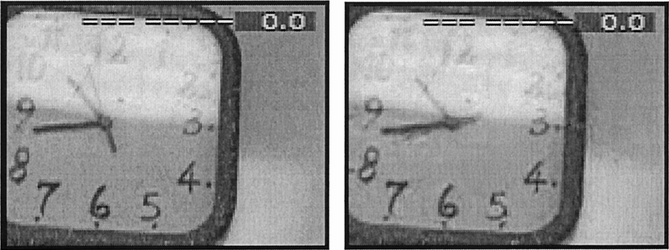
Figure 7. Local image in Quingeo, Ecuador (left) and remote image at Richmond, VA (right).
Microsoft NetMeeting is designed for maximum bandwidth use. It does this through a variety of techniques. For example, it transmits data in series of small packets, which minimizes spikes that are more subject to congestion. During periods of nonactivity, NetMeeting sends virtually no data except for ambient noise. The default algorithms compress video and audio dynamically based on the bandwidth of the connection. For example, a dial-up connection is subject to much more compression than a LAN. With decreasing bandwidth, video performance is most affected, whereas audio performance remains relatively constant.
According to a Microsoft white paper, 10 during a videoconference NetMeeting sends a complete video frame every 15 seconds and sends only changes in the image (deltas) between these complete video frames. Broader-band connections process and interpret the deltas better, which results in smoother, higher-quality video. Use of low-bandwidth connections requires that the operator minimize camera motion. Because the deltas send changes in the image, continuous camera motion results in unreadable video. Therefore, a second full frame needs to be sent. For the remote site to see a quality image, the camera must be held still for a full cycle plus the new frame: 16 seconds.
Holding a laparoscopic camera still for 16 seconds during surgery is a difficult skill to master. Slow movement of the laparoscope is a learned process, but it can be learned. Procedures that require minimal intermittent camera movement to perform, such as dissection of the cystic duct during a cholecystectomy, can be successfully teleproctored via low-bandwidth connections. However, procedures that mandate rapid camera and instrument movement, such as controlling significant intraoperative bleeding, cannot be teleprocotored via a low-bandwidth connection. As with nonproctored laparoscopic procedures, many intraoperative complications will be best addressed by conversion to an open procedure. The remote surgeons will be able to provide support of the open procedure as the telecommunication connection permits.
In conclusion, low-bandwidth, Internet-based telemedicine is an exciting surgical tool that can support both diagnosis and teaching. 11 Exploitation of these inexpensive, portable technologies will allow remote mentoring of surgical procedures around the world. Further clinical evaluation of these technologies is underway.
Acknowledgments
The authors thank the Hospital de Leopoldo Pou in Samana, Dominican Republic, the Cinterandes Foundation, Mr. Norman Stewart, and all the physicians and nursing staff involved in this project.
Footnotes
Funded in part by a grant from the National Aeronautics and Space Administration and donations from the United States Surgical Corporation and Operation Helping Hands.
Correspondence: Timothy J. Broderick, MD, Assistant Professor of Surgery, VCU/MCV Department of Surgery, Box 980519, Richmond, VA 23298-0519.
E-mail: tjbroder@hsc.vcu.edu
Accepted for publication October 19, 2000.
References
- 1.Angood PB, Doarn CR, Holoday L, et al. The Spacebridge to Russia Project: Internet-based telemedicine. Telemed J 1999; 4: 305–311. [DOI] [PubMed] [Google Scholar]
- 2.Rosser JC, Bell RL, Harnett B, et al. Use of mobile low-bandwidth telemedical techniques for extreme telemedicine applications. J Am Coll Surg 1999; 189: 397–404. [DOI] [PubMed] [Google Scholar]
- 3.Damore LJ, Johnson JA, Dixon RS, et al. Transmission of live laparoscopic surgery over the Internet. Am J Surg 1999; 178: 415–417. [DOI] [PubMed] [Google Scholar]
- 4.Lee BR, Bishoff JT, Janteschek G, et al. A novel method of surgical instruction: international telementoring. World J Urol 1998; 16: 367–379. [DOI] [PubMed] [Google Scholar]
- 5.Acuar JA, Doarn CR, Sargsyan A, et al. Use of Internet for long-term clinical follow-up. Telemed J 1998; 4: 371–374. [DOI] [PubMed] [Google Scholar]
- 6.Testimony of Jack Gleason, Acting Associate Administrator, Office of International Affairs, National Telecommunications, Information Administration, U.S. Department of Commerce On International Satellite Reform. Before the United States Senate Subcommittee on Communications, Committee on Commerce, Science, and Transportation. July 30, 1997. http://www.ntia.doc.gov/ntiahome/congress/gleason.html
- 7.Navein J, Fisher A, Geiling J, et al. Portable satellite telemedicine in practice. J Telemed Telecare 1998; 4 (suppl 1): 25–28. [DOI] [PubMed] [Google Scholar]
- 8.Turner J, Brick J, Brick JE. MDTV Telemedicine Project: technical considerations in videoconferencing for medical applications. Telemed J 1995; 1: 67–71. [DOI] [PubMed] [Google Scholar]
- 9.Bebner JA, Ruddick-Bracken H, Brebner EM, et al. Low-bandwidth tele-ultrasound. J Telemed Telecare 1999; 5: S75–76. [DOI] [PubMed] [Google Scholar]
- 10.Windows NetMeeting Resource Kit. Chapter 7, Network Bandwidth Considerations; www.microsoft.com/windows/NetMeeting/Corp/reskit/Chapter7/default.asp
- 11.Marescaux J, Mutter D, Soler L, et al. The virtual university applied to telesurgery: from tele-education to telemanipulation. Chirurgie 1999; 124: 232–239. [DOI] [PubMed] [Google Scholar]