

Abstract
Objective
To determine whether the combined administration of adrenomedullin and adrenomedullin binding protein-1 (AM/AMBP-1) has any modulatory effects on the cardiovascular response during the progression of sepsis.
Summary Background Data
Polymicrobial sepsis is characterized by an early, hyperdynamic phase followed by a late, hypodynamic phase. Recent studies have shown that AM, a newly reported potent vasodilator peptide, plays a major role in initiating the hyperdynamic response. Moreover, the reduced vascular responsiveness to AM appears to be responsible for the transition from the hyperdynamic phase to the hypodynamic phase of sepsis. Although the novel AMBP-1 augments AM-mediated action in vitro, it remains unknown whether AM/AMBP-1 maintains vascular responsiveness to AM at the late stage of sepsis.
Methods
Sepsis was induced by cecal ligation and puncture (CLP) in adult male rats. Human AMBP-1 (40 μg/kg body weight) was infused intravenously at the beginning of sepsis for 20 minutes and synthetic AM (12 μg/kg body weight) was continuously administrated for the entire study period using an Alzert micro-osmotic pump, beginning 3 hours before the induction of sepsis. At 20 hours after the onset of sepsis (i.e., the late stage), cardiac output, systemic oxygen delivery, stroke volume, total peripheral resistance, and organ blood flow in the liver, gut, kidneys, and heart were determined using radioactive microspheres. Plasma levels of transaminases (ALT, AST) and lactate were also measured. Additional studies were conducted to determine whether administration of AM alone or AMBP-1 alone alters the cardiovascular response at 20 hours after CLP. In additional rats, the necrotic cecum was excised at 20 hours after CLP following AM/AMBP-1 treatment, the peritoneal cavity irrigated with saline, and the midline incision closed in layers. Survival was then examined for a period of 10 days thereafter.
Results
Administration of AM/AMBP-1 prevented the decrease in the measured systemic and regional hemodynamic parameters at 20 hours after the onset of sepsis. Moreover, AM/AMBP-1 significantly attenuated hepatic damage and the elevation of plasma lactate, and prevented hemoconcentration. Treatment with AM/AMBP-1 reduced the overall 10-day mortality rate from 57% to 7%. Neither AM nor AMBP-1 alone was sufficient to maintain cardiovascular stability at 20 hours after CLP.
Conclusions
Since AM/AMBP-1 delays or even prevents the transition from the hyperdynamic phase to the hypodynamic phase of sepsis, attenuates tissue injury, and decreases sepsis-induced morality, these agents should provide a novel approach for maintaining cardiovascular stability and preventing cell and organ damage during the progression of polymicrobial sepsis.
The incidence of sepsis has increased significantly over the past two decades. 1,2 Despite improvements in the management of septic patients with systemic antibiotics, aggressive surgical intervention, and careful monitoring, septic shock and multiple organ failure continue to be the most common cause of death in surgical intensive care units. 3 It is possible that the subtle alterations in cellular functions that occur early after the onset of sepsis are not identified and are consequently missed, leading to inadequate or delayed treatment of the septic patient. 4 In this regard, experimental polymicrobial sepsis induced by cecal ligation and puncture (CLP) is characterized by an early, hyperdynamic phase followed by a late, hypodynamic phase. 5 Adreno-medullin (AM), a newly reported and potent vasodilator peptide, is an important mediator involved under both physiologic and pathobiological conditions. 6 Our recent studies have shown that upregulation of AM plays a major role in initiating the hyperdynamic response during the early stage of sepsis, 6–8 and the reduced vascular responsiveness to AM appears to be responsible for the transition from the hyperdynamic phase to the hypodynamic phase during the progression of polymicrobial sepsis. 9
In 1999, Elsasser et al reported that specific AM binding proteins exist in the plasma of several species, including humans. 10 Recently, the purified AM binding protein in human plasma (i.e., AM binding protein-1 [AMBP-1]) has been identified as identical to human complement factor H. 11 Studies have shown that AMBP-1 enhances AM-mediated induction of cAMP in fibroblasts, augments the AM-mediated growth of a cancer cell line, and suppresses the bactericidal capability of AM on Escherichia coli. 11 Although studies have demonstrated that a chronic increase in vascular AM production in transgenic mice was protective against the circulatory collapse, organ damage, and mortality following endotoxic shock, 12 it remains unclear whether the increased production of AM was accompanied by an enhanced AMBP-1 expression and/or binding capacity in that study. Despite the fact that AM and AMBP-1 interact synergistically under in vitro conditions, 11 it remains to be determined whether AMBP-1 reverses the vascular hyporesponsiveness to AM at the late stage of sepsis. Therefore, the present study was conducted to determine whether administration of AM in combination with AMBP-1 (AM/AMBP-1) maintains cardiovascular stability and thereby prevents the occurrence of the hypodynamic phase during the progression of polymicrobial sepsis.
METHODS
Experimental Model of Sepsis
Male adult Sprague-Dawley rats (280–320 g), purchased from Charles River Laboratories (Wilmington, MA), were used in the present study. All surgery was performed using aseptic procedures, with the exception of the induction of sepsis by CLP. Polymicrobial sepsis was induced by CLP as previously described. 5,13 In brief, the rats were fasted overnight but allowed water ad libitum before the experiment. The animals were then anesthetized with isoflurane inhalation, and a 2-cm abdominal midline incision was performed. The cecum was exposed, ligated just distal to the ileocecal valve to avoid intestinal obstruction, and then punctured twice with an 18-gauge needle. The punctured cecum was then squeezed to expel a small amount of fecal material and the abdominal incision was closed in two layers. Various parameters were determined at 20 hours after CLP (i.e., the late, hypodynamic phase of polymicrobial sepsis 5). Sham-operated rats underwent the same surgical procedure except that the cecum was neither ligated nor punctured. All animals received normal saline (3 mL/100 g body weight) subcutaneously immediately after the surgical procedure to provide fluid resuscitation.
The experiments described below were performed in adherence with the National Institutes of Health guidelines for the use of experimental animals. This project was approved by the Institutional Animal Care and Use Committee of the University of Alabama at Birmingham.
Administration of AM/AMBP-1
Synthetic rat AM (Phoenix Pharmaceuticals, Belmont, CA) was administered continuously via a jugular vein using an Alzet mini-osmotic pump (Durect, Cupertino, CA) for the entire duration of the study. Rats were fasted overnight but allowed water ad libitum before the experiment. The fasted animals were anesthetized with isoflurane inhalation and a 1.0-cm incision was made in the neck. A 200-μL mini-osmotic pump was prefilled with AM solution (dissolved with sterile normal saline to 20 μg/mL) and connected to a Silastic catheter (size 0.030“ I.D., 0.065” O.D.; Baxter, McGaw Park, IL). The prefilled pump was then primed in sterile normal saline for 2 hours at 37°C before implantation. The prefilled and primed mini-osmotic pump was then implanted subcutaneously in the rat 3 hours before induction of sepsis and the Silastic catheter was inserted into the right jugular vein for continuous infusion of AM at a constant rate of 8 μL/h for 23 hours (total dosage 12 μg/kg body weight). Following the closure of the neck incision, CLP was performed 3 hours after the implantation of the pump. The right femoral vein was then cannulated using PE-50 tubing, and 1 mL human AMBP-1 solution (containing 12 μg AMBP-1; Cortex, San Leandro, CA) was infused via the femoral venous catheter using a Harvard Pump (Harvard Apparatus, Holliston, MA) at a rate of 0.05 mL/min for a period of 20 minutes. The dose of AMBP-1 administered was approximately 40 μg/kg body weight. Vehicle-treated animals received sterile normal saline instead of AM/AMBP-1. In additional groups of septic animals, either AM alone (12 μg/kg body weight) or AMBP-1 alone (40 μg/kg body weight) was administered, as described above, to determine the effect of each individual agent on septic cardiovascular responses. AM at a dose of 12 μg/kg body weight was used since it increases plasma AM to a level that at least doubles the AM concentration observed during sepsis (600–700 pg/mL at 10–20 hours after CLP 7). The dosage of AMBP-1 used in this study was based on our preliminary study in which 2 to 5 × 10−9 mol/L AMBP-1 significantly enhanced AM-induced vascular relaxation.
Determination of Cardiac Output and Organ Blood Flow
At 20 hours after CLP or sham operation, cardiac output (CO) and blood flow in the liver, small intestine, kidneys, and heart were determined using radioactive microspheres, as previously described. 14–16 In brief, the right femoral artery and vein were cannulated with PE-50 tubing under isoflurane anesthesia. The catheter inserted into the femoral artery was connected to a blood pressure analyzer (Digi-Med, Louisville, KY) to measure mean arterial pressure (MAP) and heart rate (HR). An additional PE-50 catheter was inserted into the left ventricle via the right carotid artery. Strontium-85-labeled microspheres (DuPont/NEN, Boston, MA) were suspended in 15% dextran containing 0.05% Tween-80 surfactant to prevent aggregation. The microspheres were dispersed with a Vortex shaker for 3 minutes, and a ∼0.2 mL suspension of microspheres with an activity of ∼4 μCi/rat was infused into the left ventricle over a period of 20 seconds at a constant rate. An estimated 150,000 microspheres were injected into each rat. The reference blood sample was withdrawn from the femoral arterial catheter beginning 20 seconds before microsphere infusion and continued for 80 seconds at a rate of 0.7 mL/min. At the end of the experiment, rats were killed with an overdose of pentobarbital sodium. Liver, small intestine, colon, rectum, stomach, spleen, pancreas, mesentery, cecum (sham-operated rats only), kidneys, and heart were harvested, washed with normal saline, and gently blotted on filter paper. The radioactivity in the tissue and reference blood samples as well as the remaining microspheres, which were left in the syringe, were counted on a Wallac automatic gamma counter (1480 Wizard, Wallac, Inc., Gaithersburg, MD). CO, blood flow in various organs, stroke volume (SV), and total peripheral resistance (TPR) were calculated as previously described. 14
Determination of Systemic Oxygen Delivery, Lactate, and Hematocrit
Approximately 1-mL blood samples were withdrawn from the femoral artery and vein before the injection of microspheres. Oxygen content, lactate, and systemic hematocrit were measured using a blood gas analyzer (Radiometer Copenhagen, ABL 700 Series, Denmark). Systemic oxygen delivery (DO2) was calculated by multiplying arterial oxygen content with CO. 15
Determination of Plasma Levels of Transaminases
Blood samples (1.5 mL) were collected in EDTA-coated test tubes approximately 2 minutes after the injection of radioactive microspheres via cardiac puncture in different groups of animals. Plasma was separated by centrifugation immediately after blood sampling, and the plasma samples were stored at −70°C until assayed for alanine aminotransferase (ALT) and aspartate aminotransferase (AST). Plasma levels of ALT and AST were measured using a Sigma kit (Sigma, St. Louis, MO) according to the manufacturer’s instruction. Radioactivity in the collected blood samples was not significantly higher than background levels.
Survival Study
In additional animals (n = 14/group), the combination of AMBP-1 (40 μg/kg body weight) and AM (12 μg/kg body weight) in a volume of approximately 1 mL was infused intravenously at a constant rate over 1 hour, beginning at 5 hours after the onset of sepsis. Vehicle-treated animals received 1 mL normal saline solution. Our preliminary data indicated that infusion of AM/AMBP-1 did not significantly affect MAP and HR. At 20 hours after CLP, the necrotic cecum was excised and the abdominal cavity was washed twice using 40 mL of warm, sterile normal saline solution. The abdominal incision was then closed in layers. The procedure of cecal excision in CLP animals (CLPE) was performed to mimic the clinical situation in which the septic focus is removed whenever possible. The animals with CLPE were then allowed food ad libitum and monitored for 10 days to record the time of death in nonsurvivors.
Statistical Analysis
Data are presented as means ± SE. One-way analysis of variance and the Tukey test were used for comparison among different groups of animals. In addition, the Kaplan-Meier method was used to compare the difference in mortality rates. The differences were considered significant at P ≤ .05.
RESULTS
Effects of AM/AMBP-1 on Cardiac Output, Oxygen Delivery, Organ Blood Flow
As shown in Figure 1, CO decreased by 38% (P < .05) and systemic DO2 decreased by 33% (P < .05) at 20 hours after CLP with the administration of vehicle (normal saline). In contrast, TPR increased by 59% (P < .05) under such conditions. Administration of AM/AMBP-1 in septic animals, however, increased CO by 48% (P < .05), to a level similar to sham-operated animals. In addition, treatment with AM/AMBP-1 also increased DO2 by 47% (P < .05) and decreased TPR by 37% (P < .05) at 20 hours after CLP. SV was 69.4 ± 3.7 μL/beat/100 g body weight in sham-operated animals and decreased to 39.2 ± 4.1 μL/beat/100 g body weight (decreased by 43%, P < .05) at 20 hours after the onset of sepsis with the administration of vehicle. Treatment with AM/AMBP-1 increased SV to 59.0 ± 2.7 μL/beat/100 g body weight at 20 hours after CLP, which was not significantly different from the sham value.
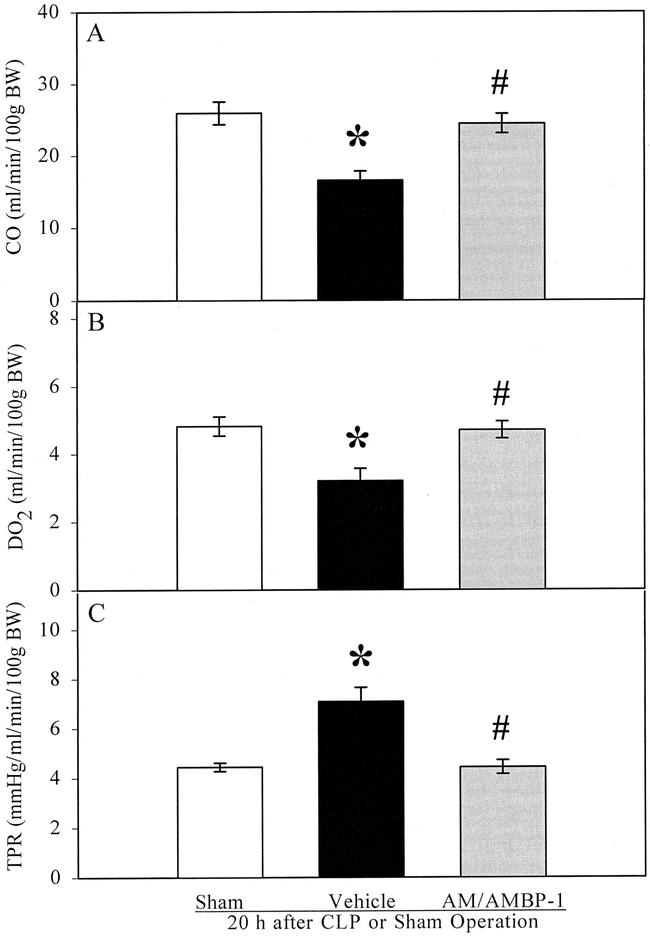
Figure 1. Alterations in cardiac output (CO, A), systemic oxygen delivery (DO2, B), and total peripheral resistance (TPR, C) in sham-operated animals and septic animals treated with vehicle (normal saline) or AM/AMBP-1 at 20 hours after the surgery. There were six animals in each group. Data are expressed as means ± SE and compared by one-way ANOVA and the Tukey test. *P < .05 versus sham-operated animals; #P < .05 versus CLP animals treated with vehicle.
Changes in hepatic perfusion are presented in Figure 2. Although hepatic arterial blood flow was not significantly altered at 20 hours after CLP in vehicle-treated animals, portal venous blood flow and total hepatic blood flow decreased significantly, indicating that the decreased total hepatic perfusion in late sepsis is due solely to the reduced portal perfusion. Administration of AM/AMBP-1, however, maintained hepatic perfusion at 20 hours after the onset of sepsis.
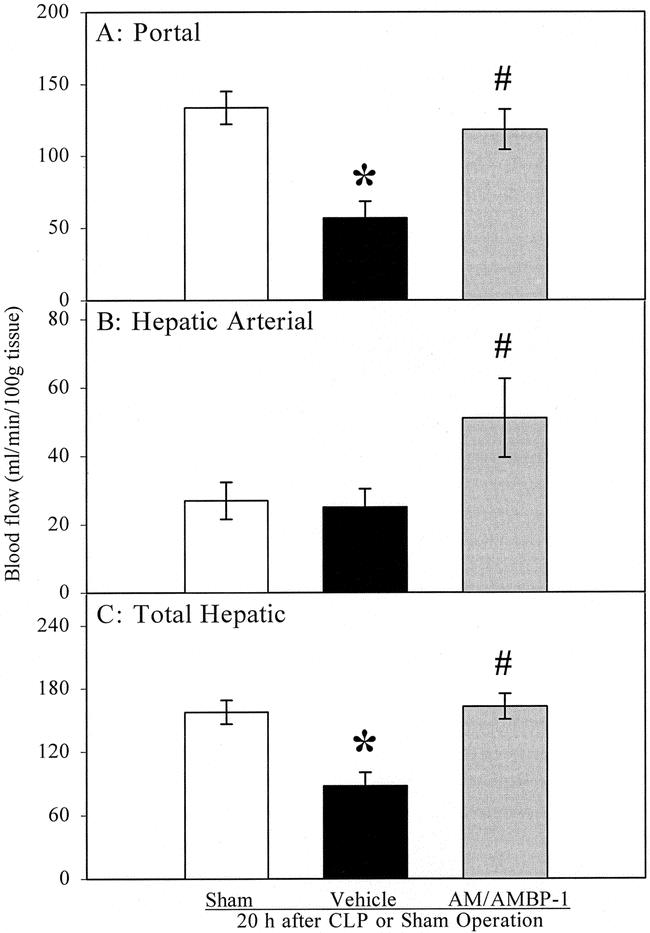
Figure 2. Alterations in portal blood flow (A), hepatic arterial blood flow (B), and total hepatic blood flow (C) in sham-operated animals and septic animals treated with vehicle (normal saline) or AM/AMBP-1 at 20 hours after the surgery. There were six animals in each group. Data are expressed as means ± SE and compared by one-way ANOVA and the Tukey test. *P < .05 versus sham-operated animals; #P < .05 versus CLP animals treated with vehicle.
Similar to total hepatic blood flow, intestinal and renal perfusion decreased by 54% and 37%, respectively, in late sepsis (Fig. 3). AM/AMBP-1 treatment prevented hypoperfusion in the gut and kidneys. Unlike the above organs, cardiac blood flow (i.e., coronary blood flow) did not decrease at 20 hours after CLP in vehicle-treated animals. Moreover, administration of AM/AMBP-1 increased cardiac blood flow by 77% (P < .05) compared to sham-operated animals. Similarly, administration of AM/AMBP-1 increased hepatic arterial blood flow by 89% over sham values, although it did not reach the statistically significant level (Fig. 2).
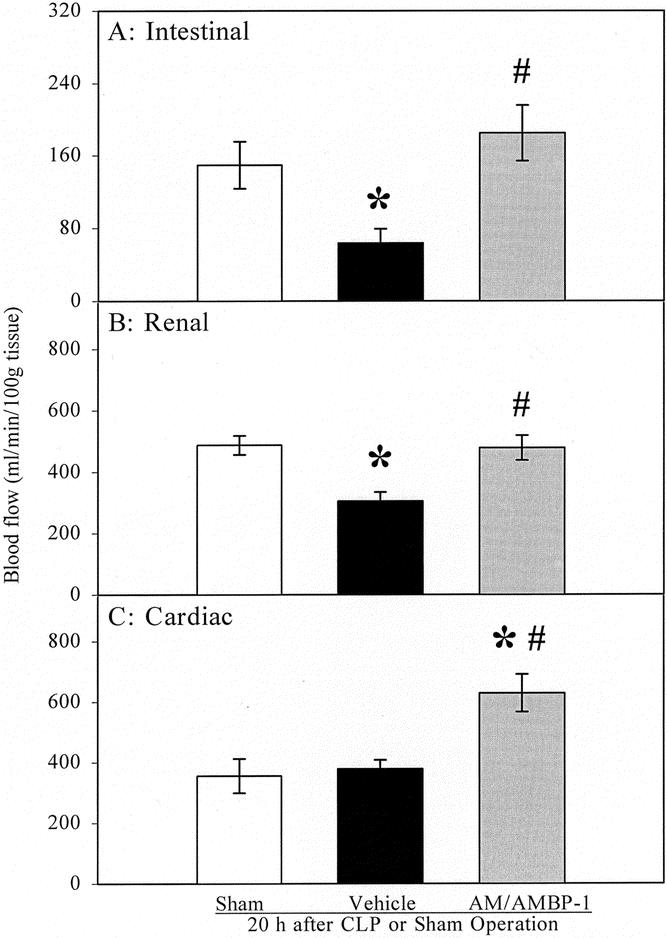
Figure 3. Alterations in small intestinal blood flow (A), renal blood flow (B), and cardiac blood flow (C) in sham-operated animals and septic animals treated with vehicle (normal saline) or AM/AMBP-1 at 20 hours after the surgery. There were six animals in each group. Data are expressed as means ± SE and compared by one-way ANOVA and the Tukey test: *P < .05 versus sham animals; #P < .05 versus CLP animals treated with vehicle.
Effects of AM/AMBP-1 on Plasma Levels of Transaminases, Lactate, and Hematocrit
As shown in Figure 4, plasma levels of ALT and AST increased by 4.5-fold and 3.9-fold, respectively, at 20 hours after CLP in vehicle-treated animals (P < .05). Administration of AM/AMBP-1, however, reduced levels of ALT and AST by 73% and 71% (P < .05), respectively, as compared to septic animals treated with vehicle, and they were not different from sham-operated animals. Similarly, circulating levels of lactate increased by 186% (P < .05), and administration of AM/AMBP-1 prevented the increase in lactate at 20 hours after CLP. Although MAP decreased statistically in AM/AMBP-1-treated septic animals, the reduction of MAP was only 9.6% and 6.4% as compared to sham and CLP with vehicle-treated animals (Table 1). HR was not significantly altered among the groups of animals studied. In contrast, systemic hematocrit increased from 44.1% to 49.1% at 20 hours after CLP (P < .05). Administration of AM/AMBP-1, however, attenuated the increase in systemic hematocrit, and there was no difference as compared with sham-operated animals.
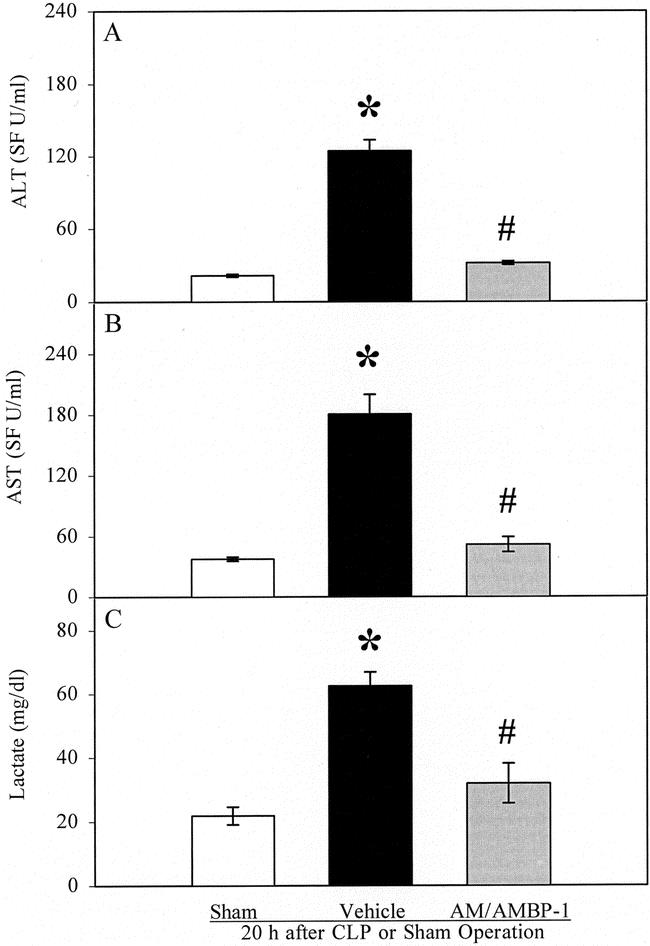
Figure 4. Alterations in plasma levels of alanine aminotransferase (ALT, A) and aspartate aminotransferase (AST, B) and plasma levels of lactate (C) in sham-operated animals and septic animals treated with vehicle (normal saline) or AM/AMBP-1 at 20 hours after the surgery. There were six animals in each group. Data are expressed as means ± SE and compared by one-way ANOVA and the Tukey test. *P < .05 versus sham-operated animals; #P < .05 versus CLP animals treated with vehicle.
Table 1. ALTERATIONS IN MEAN ARTERIAL PRESSURE, HEART RATE, AND SYSTEMIC HEMATOCRIT

Values are presented as means ± SE (n = 6/group) and compared by one-way ANOVA and the Tukey test.
*P < .05 versus sham-operated animals;
†P < .05 versus CLP animals treated with vehicle (normal saline).
Effects of AM/AMBP-1 on Survival Rate
The survival rate after CLP and cecal excision with vehicle administration was 57% at days 2 to 6 and decreased to 43% at days 7 to 10 (Fig. 5). Administration of AM/AMBP-1 at 5 hours after CLP, however, reduced the mortality rate to 7% at days 7 to 10 (P < .05). Since AM/AMBP-1 was administered intravenously at 5 hours after the onset of sepsis (i.e., posttreatment) in the mortality study, we also determined whether posttreatment with AM/AMBP-1 maintains systemic and regional hemodynamic parameters. Our results indicate that similar to the pretreatment as presented in Figures 1 to 3, intravenous administration of AM/AMBP-1 at 5 hours after the onset of sepsis prevented the decrease in CO, SV, systemic DO2, and blood flow in the liver, gut, and kidneys at 20 hours after CLP. Moreover, posttreatment with AM/AMBP-1 prevented the increased TPR. The results are similar between posttreatment and pretreatment groups.
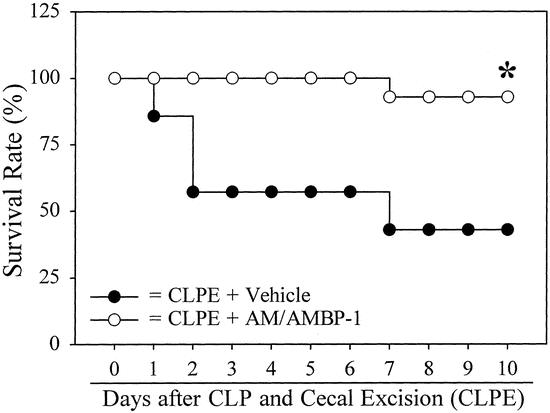
Figure 5. Effects of AM/AMBP-1 on the survival rate at 10 days after CLPE with vehicle treatment and CLPE with AM/AMBP-1 treatment. There were 14 animals in each group. Data were analyzed by the Kaplan-Meier method and compared by the log-rank test. *P < .05 versus CLPE plus vehicle.
Effects of AM Alone or AMBP-1 Alone on Systemic Hemodynamic Parameters
As shown in Table 2, neither AM alone nor AMBP-1 alone prevented the decrease in CO and SV at 20 hours after the onset of sepsis. Although the values of TPR were reduced after administration of AM alone or AMBP-1 alone, the reduction was not statistically significant from vehicle-treated animals, and it was 28% and 40% higher than sham-operated animals. Similarly, although systemic DO2 increased slightly after administration of either AM or AMBP-1 compared to vehicle-treated CLP animals, the increase was not statistically different from vehicle-treated septic animals. Moreover, both AM alone and AMBP-1 alone did not reduce plasma levels of lactate. In an additional limited number of animals, a double dose of AM (i.e., 24 μg/kg body weight for 23 hours) or chronic AM (12 μg/kg body weight for a period of 5 days) was administered. The results indicated that neither the increase in AM dosage nor the prolonged infusion duration was associated with any significant improvement in CO, SV, TPR, systemic DO2, and plasma levels of lactate at 20 hours after CLP (data not shown).
Table 2. EFFECTS OF ADMINISTRATION OF AM ALONE OR AMBP-1 ALONE ON SYSTEMIC HEMODYNAMIC PARAMETERS AND PLASMA LACTATE

TPR, total peripheral resistance; DO2, oxygen delivery; BW, body weight.
*P < .05 versus sham-operated animals.
Values are presented as means ± SE (n = 6/group) and compared by one-way ANOVA and the Tukey test. Values of cardiac output TPR, DO2, and lactate in sham group and CLP-vehicle treated animals are derived from Figs. 1 and 4.
DISCUSSION
The 52-amino acid residue peptide AM was first isolated by Kitamura et al from human pheochromocytomas and reported in 1993. 17 In general, AM’s physiologic effects are associated with cardiovascular, endocrine, and renal mechanism that control fluid and electrolyte homeostasis. 18 However, the vasodilator properties of AM are of particular interest in the pathophysiology of sepsis. 6 AM elicits its vasodilator effects through two different mechanisms: a direct effect on vascular smooth muscle cells to increase intracellular cAMP by stimulating AM receptors and adenylate cyclase activity, 6,19–21 and an indirect effect on vascular endothelial cells by stimulating Ca2+ mobilization to increase endothelium-derived nitric oxide release via the stimulation of constitutive nitric oxide synthase. 6,22 AMBP-1 (i.e., human complement factor H) is a specific serum-binding protein for AM. AMBP-1 is a single-chain glycoprotein consisting of 20 subunits called short consensus repeats. 23 Studies have demonstrated that AMBP-1 is synthesized by various cells such as mononuclear phagocytes, fibroblasts, endothelial cells, mesangial cells, astrocytes, oligodendrocytes, and neurons; however, the liver is considered to be the primary site for synthesizing and releasing AMBP-1. 24 Although the precise mechanism by which AMBP-1 augments AM activity remains to be determined, studies have shown that AMBP-1 can bind to cell surfaces through the various glycosaminoglycan binding sites present in its structure. 25–27 In addition, it has also been demonstrated that AMBP-1 may modulate neutrophil function. 28 Moreover, AMBP-1 may also act as a carrier and reservoir of AM, providing concentrated levels of AM at the particular tissue or cell population to stimulate its receptors. 11
Polymicrobial sepsis induced by CLP is characterized by a biphasic hemodynamic response—in other words, an early, hyperdynamic stage (2–10 hours after CLP) characterized by increased CO, tissue perfusion, and oxygen delivery, and decreased vascular resistance, followed by a late, hypodynamic stage (longer than 16 hours post-CLP) characterized by reduced CO, organ blood flow, and oxygen delivery, increased TPR, and lactate acidosis. 15,29,30 Previous studies from our laboratory have indicated that plasma levels of AM increased as early as 2 hours after CLP, progressively increased from 5 to 20 hours, and remained elevated at 30 hours after the onset of sepsis. 7 Moreover, the increased AM production and release play an important role in initiating the hyperdynamic response during the early stage of sepsis. 8 However, despite the elevated plasma levels of AM at the late stage of sepsis, vascular responsiveness to AM decreased significantly at both the macro- and the microcirculatory levels. 9 Such a reduction in vascular responsiveness to AM may lead to hemodynamic instability and appears to be responsible for producing the transition from the hyperdynamic to the hypodynamic stage of sepsis. 6,9 Although the precise mechanism responsible for the reduction in vascular responsiveness to AM remains unknown, it is likely that alterations occur in AM–AMBP-1 interaction and/or membrane-bound AM receptors during the progression of sepsis. In this regard, Pio et al have recently shown that AMBP-1 synergistically enhances AM action under in vitro conditions. 11 In line with their findings, our preliminary results have shown that administration of AMBP-1 significantly increased AM-induced vascular relaxation in isolated aortic rings from rats at 20 hours after CLP. Based on the above findings, we hypothesized that administration of AM/AMBP-1 maintains cardiovascular stability and prevents the transition from the hyperdynamic phase to the hypodynamic phase during the progression of polymicrobial sepsis.
Our results demonstrated that administration of AM/AMBP-1 prevented the decrease in CO, SV, systemic oxygen delivery, and blood flow in the liver, gut, and kidneys at 20 hours after the onset of sepsis. In contrast, AM/AMBP-1 significantly decreased TPR under such conditions. Administration of AM/AMBP-1 markedly increased coronary blood flow at 20 hours after CLP, even compared with the sham value. In addition, treatment with AM/AMBP-1 reduced plasma levels of ALT, AST, and lactate at 20 hours after the onset of sepsis and prevented hemoconcentration. Furthermore, administration of AM/AMBP-1 significantly decreased sepsis-induced mortality. These data clearly indicate that AM/AMBP-1 delays or even prevents the transition from the hyperdynamic phase to the hypodynamic phase during the progression of polymicrobial sepsis. The primary focus of the present study was to determine the effects of AM/AMBP-1 on the cardiovascular response during sepsis. Our results have clearly shown that administration of AM/AMBP-1 maintains cardiovascular function even during the late, hypodynamic stage of sepsis. The findings that AM/AMBP-1 significantly attenuated the elevated plasma levels of ALT, AST, and lactate further suggest that AM/AMBP-1 is indeed beneficial in sepsis. In addition, our preliminary results have indicated that the upregulated proinflammatory cytokine TNF-α was significantly attenuated following the administration of AM/AMBP-1. However, future studies are required to determine the effects of AM/AMBP-1 on hepatocellular function, renal function, and gut absorptive function, as well as vascular endothelial cell function.
Although administration of AM alone or AMBP-1 alone did not significantly alter CO and SV, AM increased both parameters by approximately 20% while AMBP-1 increased them by approximately 15%. To determine whether administration of AM could prevent the reduction in CO at the late stage of sepsis, we administered twice the amount of AM in septic animals. Our preliminary results have shown that a higher dose of AM does not prevent the reduction of cardiac output at 20 hours after the onset of sepsis. In addition, administration of AM for 5 days (beginning 4 days before the onset of sepsis) also does not prevent the reduced CO and SV. Moreover, preliminary data show that AMBP-1 does not appear to have any significant effects on vascular relaxation. These results, taken together, suggest that while administration of AM or AMBP-1 alone in sepsis may have some beneficial effects on the cardiovascular response, neither agent is sufficient to prevent the decreased CO and SV. Since we determined the effect of AM on the cardiovascular response only at 20 hours after CLP, it remains to be determined whether administration of AM alone would have any beneficial effects on the cardiovascular response during the early stage of sepsis (i.e., 5–10 hours after CLP). Moreover, future studies are also directed at determining whether administration of AMBP-1 further enhances the hyperdynamic response during the early stage of sepsis (e.g., 5 hours after CLP) and, if so, whether the further enhanced cardiovascular response is beneficial or detrimental.
Studies by Shindo et al have shown that AM is protective against the circulatory collapse, organ damage, and mortality characteristic of endotoxic shock in transgenic mice, which chronically express AM gene. 12 In addition, studies by Dobrzynski et al have demonstrated that AM gene delivery attenuates hypertension, cardiac remodeling, and renal injury in deoxycorticosterone acetate-salt hypertension rats. 31 Since the above authors did not determine AMBP-1 levels in their preparations, it is unclear whether the beneficial effect of upregulation of AM gene is due primarily to AM alone or also due to accompanying upregulation of AMBP-1 expression and/or binding capacity. In this regard, we found that CO and organ perfusion were not maintained at 20 hours after CLP if the septic animals were treated with AM alone at different dosages or duration of infusion. This would suggest that AM alone is insufficient to maintain hemodynamic stability during the progression of sepsis. Similarly, the reduction in various hemodynamic parameters was not prevented at 20 hours after the onset of sepsis following the administration of AMBP-1 alone. In contrast, treatment with AM and AMBP-1 in combination is indeed beneficial. Although the mechanism responsible for the beneficial effects of AM/AMBP-1 in sepsis remains to be determined, we propose that the vascular hyporesponsiveness to AM observed during the late, hypodynamic phase of sepsis is at least in part caused by the altered AM–AMBP-1 interaction. Since there is no bioassay for determining AM bioactivity, it is possible that some portion of the circulating AM becomes insufficient during the late stage of sepsis. Nonetheless, further studies are required to determine the precise role of plasma AM, AMBP-1, AM receptors, and the signal transduction mechanism in the development of vascular hyporesponsiveness to AM at the late stage of polymicrobial sepsis. Administration of AM and AMBP-1 was initiated 3 hours before the onset of sepsis and at the time of sepsis procedure, respectively. This pretreatment was performed to maximize the effect of AM/AMBP-1 during the progression of sepsis. Similar to the pretreatment, administration of AM/AMBP-1 following the onset of sepsis (i.e., 5 hours after CLP) has many beneficial effects as evidenced by improved survival rate and systemic and regional hemodynamic parameters.
Although the primary objective of this study was to determine whether administration of AM/AMBP-1 in sepsis is beneficial, a separate study has been completed to examine the possible mechanisms responsible for the improved survival and cardiovascular responses following the administration of AM/AMBP-1 in sepsis. Our preliminary results suggest that the inadequate interaction of AM and AMBP-1 due to the reduced vascular levels of AMBP-1 appears to be responsible for the reduced vascular AM responsiveness observed during the late stage of sepsis. The finding that addition of AMBP-1 restored the reduced AM-induced vascular relaxation at 20 hours after the onset of sepsis suggests that the beneficial effect of AM/AMBP-1 in the present study may be due to the normalization of the vascular responsiveness to AM. Although we have demonstrated that vascular levels of AMBP-1 decrease during the late stage of sepsis, it remains an interesting issue to determine the role of AMBP-1 in the hyperdynamic response during the early stage of sepsis. In addition, our preliminary results have indicated that AM receptor (i.e., calcitonin receptor-like receptor [CRLR], receptor activity-modifying protein-2 [RAMP-2] and RAMP-3) gene expression was not altered in the vascular tissues at 20 hours after the onset of sepsis. However, it remains unknown whether AM receptor binding capacity and/or affinity are altered under such conditions and, if so, whether AM/AMBP-1 has any effects on AM receptors. Moreover, preliminary TNF-α data indicate that serum levels of TNF-α increased by 1,230% at 20 hours after the onset of sepsis. Administration of AM/AMBP-1, however, reduced TNF-α levels by 83% to a level similar to sham-operated animals.
In summary, we have first demonstrated, in a rat model of polymicrobial sepsis, that AM/AMBP-1 prevents the transition from the hyperdynamic phase to the hypodynamic phase, attenuates tissue injury and hemoconcentration during the late, hypodynamic stage of sepsis, and decreases sepsis-induced mortality. Thus, AM/AMBP-1 should be considered as a novel approach to maintain cardiovascular stability and prevent cell and organ damage during the progression of polymicrobial sepsis.
Acknowledgments
The authors thank Dale Fowler, MD, for his critical review of this manuscript and Dung-Tsa Chen, PhD, and Seng-Jaw Soong, PhD, for performing statistical analysis on the mortality data.
Footnotes
Supported by NIH Grants RO1 GM57468 and KO2 AI01461 (P.W.).
Correspondence: Ping Wang, MD, Division of Surgical Research, NS-LIJ Medical Center, North Shore-Long Island Jewish Research Institute, 350 Community Drive, Manhasset, NY 11030.
E-mail: pwang@nshs.edu
Accepted for publication January 18, 2002.
References
- 1.Bone RC. Sepsis and its complications: the clinical problem. Crit Care Med 1994; 22: S8–S11. [PubMed] [Google Scholar]
- 2.Baue AE, Durham R, Faist E. Systemic inflammatory response syndrome (SIRS), multiple organ dysfunction syndrome (MODS), multiple organ failure (MOF): are we winning the battle? Shock 1998; 10: 79–89. [DOI] [PubMed] [Google Scholar]
- 3.Baue AE. Multiple organ failure, multiple organ dysfunction syndrome, and systemic inflammatory response syndrome: Why no magic bullets? Arch Surg 1997; 132: 703–707. [DOI] [PubMed] [Google Scholar]
- 4.Koo DJ, Chaudry IH, Wang P. Mechanism of hepatocellular dysfunction during sepsis: the role of gut-derived norepinephrine. Int J Mol Med 2000; 5: 457–465. [DOI] [PubMed] [Google Scholar]
- 5.Wang P, Chaudry IH. A single-hit model of polymicrobial sepsis: cecal ligation and puncture. Sepsis 1998; 2: 227–233. [Google Scholar]
- 6.Koo DJ, Zhou M, Chaudry IH, et al. The role of adrenomedullin in producing differential hemodynamic responses during sepsis. J Surg Res 2001; 95: 207–218. [DOI] [PubMed] [Google Scholar]
- 7.Wang P, Zhou M, Ba ZF, et al. Up-regulation of a novel potent vasodilator peptide adrenomedullin during polymicrobial sepsis. Shock 1998; 10: 118–122. [DOI] [PubMed] [Google Scholar]
- 8.Wang P, Ba ZF, Cioffi WG, et al. The pivotal role of adrenomedullin in producing hyperdynamic circulation during the early stage of sepsis. Arch Surg 1998; 133: 1298–1304. [DOI] [PubMed] [Google Scholar]
- 9.Wang P, Yoo P, Zhou M, et al. Reduction in vascular responsiveness to adrenomedullin during sepsis. J Surg Res 1999; 85: 59–65. [DOI] [PubMed] [Google Scholar]
- 10.Elsasser TH, Kahl S, Martinez A, et al. Adrenomedullin binding protein in the plasma of multiple species: characterization by radioligand blotting. Endocrinology 1999; 140: 4908–4911. [DOI] [PubMed] [Google Scholar]
- 11.Pio R, Martinez A, Unsworth EJ, et al. Complement factor H is a serum binding protein for adrenomedullin. The resulting complex modulates the bioactivities of both partners. J Biol Chem 2001; 276: 12292–12300. [DOI] [PubMed] [Google Scholar]
- 12.Shindo T, Kurihara H, Maemura K, et al. Hypotension and resistance to lipopolysaccharide-induced shock in transgenic mice overexpressing adrenomedullin in their vasculature. Circulation 2000; 101: 2309–2316. [DOI] [PubMed] [Google Scholar]
- 13.Chaudry IH, Wichterman KA, Baue AE. Effect of sepsis on tissue adenine nucleotide levels. Surgery 1979; 85: 205–211. [PubMed] [Google Scholar]
- 14.Wang P, Ba ZF, Chaudry IH. Increase in hepatic blood flow during early sepsis is due to increased portal blood flow. Am J Physiol 1991; 261: R1507–R1512. [DOI] [PubMed] [Google Scholar]
- 15.Yang S, Cioffi WG, Bland KI, et al. Differential alterations in systemic and regional oxygen delivery and consumption during the early and late stages of sepsis. J Trauma 1999; 47: 706–712. [DOI] [PubMed] [Google Scholar]
- 16.Yang S, Koo DJ, Chaudry IH, et al. The important role of the gut in initiating the hyperdynamic response during early sepsis. J Surg Res 2000; 89: 31–37. [DOI] [PubMed] [Google Scholar]
- 17.Kitamura K, Kangawa K, Kawamoto M, et al. Adrenomedullin. A novel hypotensive peptide isolated from human pheochromocytoma. Biochem Biophys Res Commun 1993; 192: 553–560. [DOI] [PubMed] [Google Scholar]
- 18.Samson WK, Resch ZT, Murphy TC, et al. Adrenomedullin: is there physiological relevance in the pathology and pharmacology? News Physiol Sci 1999; 14: 255–259. [DOI] [PubMed] [Google Scholar]
- 19.Eguchi S, Hirata Y, Iwasaki H, et al. Structure-activity relationship of adrenomedullin, a novel vasodilatory peptide, in cultured rat vascular smooth muscle cells. Endocrinology 1994; 135: 2454–2458. [DOI] [PubMed] [Google Scholar]
- 20.Eguchi S, Hirata Y, Kano H, et al. Specific receptors for adrenomedullin in cultured rat vascular smooth muscle cells. FEBS Lett 1994; 340: 226–230. [DOI] [PubMed] [Google Scholar]
- 21.Montuenga LM, Martinez A, Miller MA, et al. Expression of adrenomedullin and its receptor during embryogenesis suggests autocrine or paracrine modes of action. Endocrinology 1997; 138: 440–451. [DOI] [PubMed] [Google Scholar]
- 22.Shimekake Y, Nagata K, Ohta S, et al. Adrenomedullin stimulated two signal transduction pathways, cAMP accumulation and Ca2+ mobilization, in bovine aortic endothelial cells. J Biol Chem 1995; 270: 4412–4417. [DOI] [PubMed] [Google Scholar]
- 23.Ripoche J, Day AJ, Harris TJ, et al. The complete amino acid sequence of human complement factor H. Biochem J 1988; 249: 593–602. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Friese MA, Hellwage J, Jokiranta TS, et al. Different regulation of factor H and FHL-1/reconectin by inflammatory mediators and expression of the two proteins in rheumatoid arthritis (RA). Clin Exp Immunol 2000; 121: 406–415. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Blackmore TK, Hellwage J, Sadlon TA, et al. Identification of the second heparin-binding domain in human complement factor H. J Immunol 1998; 160: 3342–3348. [PubMed] [Google Scholar]
- 26.Blackmore TK, Sadlon TA, Ward HM, et al. Identification of a heparin binding domain in the seventh short consensus repeat of complement factor H. J Immunol 1996; 157: 5422–5427. [PubMed] [Google Scholar]
- 27.Pangburn MK, Atkinson MA, Meri S. Localization of the heparin-binding site on complement factor H. J Biol Chem 1991; 266: 16847–16853. [PubMed] [Google Scholar]
- 28.DiScipio RG, Daffern PJ, Schraufstatter IU, et al. Human polymorphonuclear leukocytes adhere to complement factor H through an interaction that involves alphaM-beta2 (CD11b/CD18). J Immunol 1998; 160: 4057–4066. [PubMed] [Google Scholar]
- 29.Wang P, Chaudry IH. Mechanism of hepatocellular dysfunction during hyperdynamic sepsis. Am J Physiol 1996; 270: R927–R938. [DOI] [PubMed] [Google Scholar]
- 30.Deitch EA. Animal models of sepsis and shock: a review and lessons learned. Shock 1998; 9: 1–11. [DOI] [PubMed] [Google Scholar]
- 31.Dobrzynski E, Wang C, Chao J, et al. Adrenomedullin gene delivery attenuates hypertension, cardiac remodeling, and renal injury in deoxycorticosterone acetate-salt hypertensive rats. Hypertension 2000; 36: 995–1001. [DOI] [PubMed] [Google Scholar]