

Abstract
Objective
To compare estimates of dental visits among adults using three national surveys.
Data Sources/Study Design
Cross-sectional data from the National Health Interview Survey (NHIS), National Health and Nutrition Examination Survey (NHANES), and National Health Expenditure surveys (NMCES, NMES, MEPS).
Study Design
This secondary data analysis assessed whether overall estimates and stratum-specific trends are different across surveys.
Data Collection
Dental visit data are age standardized via the direct method to the 1990 population of the United States. Point estimates, standard errors, and test statistics are generated using SUDAAN.
Principal Findings
Sociodemographic, stratum-specific trends are generally consistent across surveys; however, overall estimates differ (NHANES III [364-day estimate] versus 1993 NHIS: –17.5 percent difference, Z=7.27, p value < 0.001; NHANES III [365-day estimate] vs. 1993 NHIS: 5.4 percent difference, Z=–2.50, p value=0.006; MEPS vs. 1993 NHIS: –29.8 percent difference, Z=16.71, p value < 0.001). MEPS is the least susceptible to intrusion, telescoping, and social desirability.
Conclusions
Possible explanations for discrepancies include different reference periods, lead-in statements, question format, and social desirability of responses. Choice of survey should depend on the hypothesis. If trends are necessary, choice of survey should not matter; however, if health status or expenditure associations are necessary, then surveys that contain these variables should be used, and if accurate overall estimates are necessary, then MEPS should be used. A validation study should be conducted to establish “true” utilization estimates.
Keywords: Dental care/utilization, dental health surveys, United States epidemiology, adult
The nation requires valid and reliable estimates of the proportion of the population with a dental visit each year for a variety of important purposes. For example, public health practitioners and legislators rely on these data to develop policy concerning access to care and the financing of oral health services. Policymakers also use these data to identify barriers to oral health care for specific populations subgroups and to create programs that eliminate obstacles to oral health care. Researchers use dental visit data to assess trends over time and to evaluate changes resulting from the implementation of health programs. Finally, federal agencies use these utilization estimates to track progress toward national health objectives (Health People Objectives) (U.S. Department of Health and Human Services 1997).
There are three main sources of nationally representative dental visit data in the United States. These sources include the National Health Interview Survey (NHIS), National Health and Nutrition Examination Survey (NHANES), and health expenditure surveys (1977 National Medical Care Expenditure Survey [NMCES], 1987 National Medical Expenditure Survey [NMES], and 1996 Medical Expenditure Panel Survey [MEPS]). The National Center for Health Statistics (NCHS) of the Centers for Disease Control and Prevention conducts the NHIS and NHANES, and the Agency for Healthcare Research and Quality, formerly the Agency for Health Care Policy and Research, administers the health expenditure surveys.
The NHIS has long been the standard data source in the United States for dental visit information. For example, public health professionals used dental visit data from the NHIS for baseline and periodic national health objective assessments during the 1980s and 1990s. In more recent years, the relative ease with which researchers have had access to NHANES and health expenditure survey data suggests that surveys other than the NHIS might be relied on to provide dental visit estimates in the future. Although one might hypothesize that the dental visit estimates derived from the NHANES and health expenditure surveys should be comparable to those derived from the NHIS, this hypothesis has remained untested.
The purpose of this investigation was to compare dental visit estimates derived from the standard NHIS with estimates derived from NHANES and the health expenditure surveys. We assessed differences on two levels: (1) overall estimates across surveys and (2) stratum-specific trends within surveys. This investigation is important because it addresses whether, and to what extent, NHANES and the health expenditure surveys differ from the standard NHIS and places the differences in the context of relevant political, public health, and research issues.
Selection of Surveys and Survey Years
This manuscript contains data derived from several surveys, including the 1986 NHIS, 1989 NHIS, and 1993 NHIS; NHANES I (conducted between 1971 and 1975) and NHANES III (conducted between 1988 and 1994); and 1977 NMCES, 1987 NMES, and 1996 MEPS health expenditure surveys. We selected these surveys because they were representative of the U.S. population, they served as common references for dental visits, and they were administered by more than one federal agency. We selected several survey years from within each data source in order to assess the stability of estimates over time.
NHIS
The objective of the NHIS is to assess timely health issues through the collection and analysis of data related to (1) health and illness status, (2) general health attitudes, behaviors, and knowledge, and (3) health care utilization (Massey et al. 1989). The NHIS is the largest source of such self-reported data for the civilian, noninstitutionalized household population of the United States. Prior to a survey redesign in 1997, the NHIS questionnaire consisted of two parts: a set of basic health and demographic items contained within a core component and one or more sets of questions on current health topics contained within a supplement component. Questions contained within the supplement component change from year to year in response to current interest and need for data (Massey et al. 1989). The NHIS frequently includes an oral health supplement that contains questions regarding oral health care utilization. An advantage of the NHIS is that it uniquely allows analysis of the associations between oral health care utilization and a variety of health and illness status items, as well as health attitudes, behaviors, and knowledge.
The NHIS has included questionnaire items concerning dental visits and utilization on and off since the late 1950s. For the purposes of this investigation, we selected three of the most currently available NHIS instruments: the 1986 NHIS, the 1989 NHIS, and the 1993 NHIS. The 1986 NHIS contained a Dental Health Supplement questionnaire that assessed utilization of oral health care services using several reference periods, including 2 weeks, 12 months, and 5 years or beyond (Jack and Bloom 1988). The supplement was administered to half of the total NHIS sample (n =62,052 persons) (Jack and Bloom 1988). Only survey participants 2 years of age or older were eligible for the dental visit questions, and the survey allowed proxy respondents to answer the utilization items for those unable to respond for themselves.
The 1989 NHIS also contained a Dental Health Supplement questionnaire (Jack and Bloom 1988); however, unlike the 1986 version, this supplement was administered to the entire sample of 109,603 persons (Bloom, Gift, and Jack 1993). Again, only survey participants 2 years of age or older were eligible for the dental visit question, and proxy respondents were allowed.
The dental visit item for the 1993 NHIS was contained within the Oral Health Section of the Year 2000 Supplement questionnaire (Benson and Marano 1994). This questionnaire only contained an item that used an open-ended format, and it was asked solely of adults 18 years of age or older. The Oral Health Section was administered to one sample adult from each household but only during the latter half of the survey year (n = 21,028) (Benson and Marano 1994). Proxy respondents were allowed for this NHIS supplement, as well.
NHANES
NHANES is the primary source of nutrition and physical examination data for the civilian, noninstitutionalized population of the United States (Miller 1977; U.S. Department of Health and Human Services 1994). Since 1970, five health examination surveys have been completed. A sixth health examination survey is currently in the field and will be the first to be conducted as a continuously administered survey. The goals of the survey are to (1) determine the national prevalence of selected diseases and risk factors, (2) estimate national population reference distributions of selected health parameters, and (3) investigate reasons for secular trends in selected diseases and risk factors (Miller 1977; U.S. Department of Health and Human Services 1994). Additional goals, which are unique to NHANES III, include contributing to an understanding of disease etiology and investigating the natural history of selected diseases (U.S. Department of Health and Human Services 1994). An advantage of NHANES is that it uniquely allows analysis of the associations between oral health care utilization and oral health status, such as dental caries and periodontal disease.
NHANES I, conducted between 1971 and 1975, included 20,729 participants (Miller 1977). NHANES III, conducted between 1988 and 1994, included a total of 33,994 participants. The NHANES III survey oversampled children under 6 years of age and adults over 59 years of age, as well as Mexican Americans and non-Hispanic Blacks (U.S. Department of Health and Human Services 1994). Both surveys collected information on health and socioeconomic status via a combination of face-to-face interviews, physical examinations, and laboratory analyses. NHANES I collected dental visit information from participants 25 years of age or older only, whereas NHANES III gathered dental visit data from all participants 2 years of age or older. The physical assessment component of both surveys included a thorough oral examination.
Health Expenditure Surveys
Three health expenditure surveys are the primary source of national data describing the cost and financing of health care among the civilian, noninstitutionalized population of the United States. The first of the health expenditure surveys was the 1977 NMCES (Berk and Bernstein 1985; Cohen and Burt 1985). This survey provides detailed national health care expenditure, utilization, and insurance coverage estimates. The second health expenditure survey was the 1987 NMES (Edwards and Berlin 1989; Harper, Berlin, DiGaetano, et al. 1991). This survey provides additional and enhanced estimates of health care expenditures, utilization, sources of payment, and insurance coverage. The 1996 MEPS (Cohen 1997) was the most recent of the nationally representative health expenditure surveys. The 1996 MEPS is similar to the 1977 NMCES and 1987 NMES in that it provides estimates of health care expenditures, utilization, payment source, insurance coverage, as well as descriptions of socioeconomic level, demographics, and health insurance coverage. The 1996 MEPS differs from the 1977 NMCES and 1987 NMES, however, in that the MEPS data are collected as part of a 2-year panel and the survey has been fielded continuously since 1996. An advantage of health expenditure surveys is that they uniquely allow analysis of the associations between oral health care utilization and health care costs.
The NMCES was a panel study that used a sample of approximately 14,000 households (U.S. Department of Health and Human Services 1981). The NMCES included data that were collected via a series of face-to-face interviews administered six different times over an 18-month period, spanning 1977 and 1978. Annual dental visit and expenditure data were collected in the first five rounds of NMCES (U.S. Department of Health and Human Services 1981).
The 1987 NMES was also a panel study (Edwards and Berlin 1989). This survey oversampled population subgroups of specific interest for policy, such as the older population, persons with limitations in activities, racial and ethnic minorities, and the poor. The NMES used a sample of approximately 14,000 households and included data gathered via face-to-face interviews that were administered five times over an 18-month study period. The survey covered health care use and expenditures, demographic factors, socioeconomic status, and health insurance coverage. NMES also collected information regarding 38,429 dental visits by 13,439 individuals, and it identified the type of service, expenditures, and source of payment for each visit. Although the round four interviews were conducted during the first 4 months of 1988, questions were asked only of dental visits made during 1987.
The sample for the 1996 MEPS included 10,500 NHIS households drawn from 195 primary sampling units that represented areas with a higher proportion of non-Hispanic Blacks and Hispanics. The MEPS instrument differed from the NMES and NMCES in that (1) household respondent data for each panel were collected over 2 consecutive years and (2) the survey was fielded continuously; a new panel was selected each year. The MEPS instrument collected health expenditure and utilization data from household sample persons during three separate rounds over an 18-month period spanning 1996 and 1997 (Cohen 1997). In addition, the sample used during the 1995 NHIS served as the sample for the 1996 MEPS.
Dental Visit Items
Figures 1 through 3 list all of the questionnaire items from each data source. Items contained within the NHIS differed slightly across survey years (Figure 1). The 1986 and 1989 NHIS, for example, contained three different dental visit items. In contrast to the 1986 and 1989 NHIS, the 1993 NHIS contained only a single item that asked about dental visits made during the preceding 12 months. Each of the NHIS dental visit items contained a lead sentence that introduced the oral health sections. The 12-month NHIS questionnaire items were used to derive the estimates contained in this manuscript because they were common to each of the 3 survey years.
Figure 1.
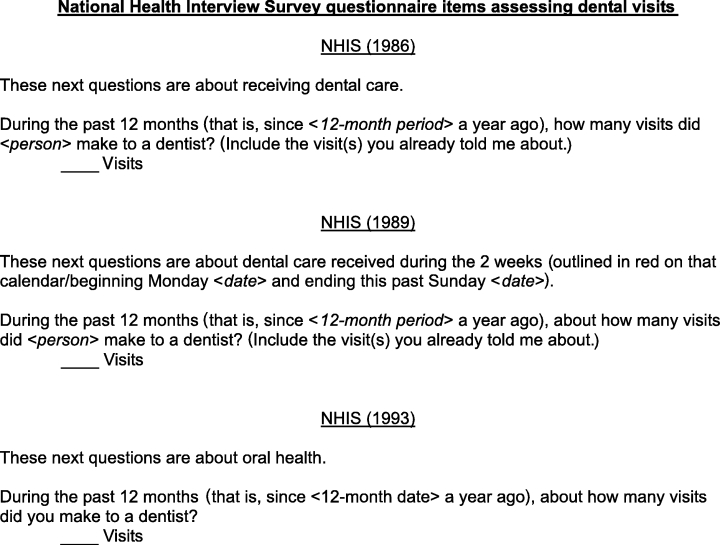
National Health Interview Survey Questionnaire Items Assessing Dental Visits
The dental visit questions contained within NHANES I and III also differed (Figure 2). The NHANES I categorical questionnaire item, for example, asked when was the last time the survey participant had visited or talked with a dentist. The NHANES III questionnaire item asked in an open-ended format how long ago was the last visit to a dentist or dental hygienist. The responses, listed as number of days since last visit, could be coded as visits occurring in the previous 12 months.
Figure 2.
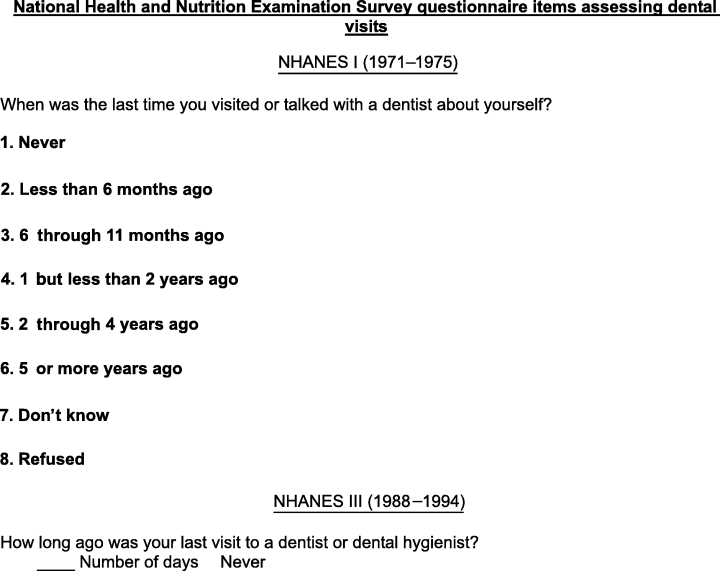
National Health and Nutrition Examination Survey Questionnaire Items Assessing Dental Visits
The conversion of the open-ended NHANES III utilization item to the total number of days since the last visit provided a reasonable estimate of utilization when the exact date of the dental visit was known. It required some interviewer interpretation, however, when the respondent was less sure, for example, when the survey participant reported that his or her last dental visit was “about a year ago.” NHANES III dental visit data are listed in the Results and Discussion sections according to the two ways that the “past year” could have been defined.
Figure 3 lists the utilization items contained within the health expenditure surveys. The NMCES had three questions concerning dental visits. In each case, the reference period for the questionnaire items was a 3-month period between the beginning and end of each round during the 1977 survey year. The NMES combined all oral health care professionals into a single questionnaire item. The reference period for the NMES was similar to the NMCES in that respondents were asked about utilization during different 3- to 4-month time intervals over the course of the year. The MEPS posed the utilization questions in yet another way. The first of two items asked the respondent whether a dental visit was made to any type of dental professional listed on a card, and the second item asked if the respondent had seen any other type of oral health care professional listed on the card. The reference period for the MEPS was similar to the NMCES and NMES in that the questions were asked for different 3- to 4-month time periods during the year. A lead statement introduced the utilization sections for each of the health expenditure surveys.
Figure 3.
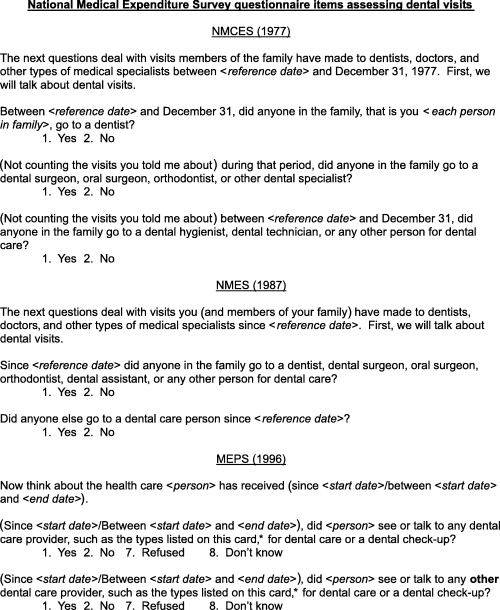
National Medical Expenditure Survey Questionnaire Items Assessing Dental Visits
Descriptive Variables
Descriptive variables included age, gender, race/ethnicity, poverty status, and level of education. Race/ethnicity included three categories: non-Hispanic White, non-Hispanic Black, and Hispanic. In the definition of Hispanic, the NHIS and health expenditure surveys included persons from several Latin American countries and Spain, whereas the NHANES III survey included only Mexican Americans. NHANES I did not oversample Hispanics and was thus unable to provide reliable estimates for this group. Races other than White or Black were excluded from this study because of small sample sizes in each of the surveys. The poverty status variable included three categories: at or above 100 percent poverty, below 100 percent poverty, and unknown. The education variable included three categories based on number of years of formal education.
Analyses
Age is significantly associated with oral health care utilization. Because the distribution of age in the United States has changed during the past 3 decades and because the national surveys have spanned these decades, we required a way to remove the potential confounding effect of age from the derivation of dental visit estimates. In order to correct for changes in the distribution of age in the population over time and remove age as a potential confounder, we adjusted, or standardized, the utilization estimates presented in this manuscript to the age distribution of the 1990 United States population, via the direct standardization method. In the direct method of standardization, the adjusted rates are derived by applying stratum-specific rates from each of the survey populations to a single standard population, akin to adjusting for inflation in an economic evaluation. Although differences between the crude and age-standardized estimates were very small, we nonetheless included adjusted estimates in the manuscript so that changes in the distribution of age in the population could be eliminated as a possible explanation for any variations across surveys and time. We compared the proportion of the population that reported a dental visit on two levels for this investigation. For example, we based comparisons of estimates derived from two different data instruments on a two-sample t test for independent samples with unequal variance. These comparisons were calculated using a normal distribution:
In comparing estimates derived from a single data instrument and survey year, we used odds ratio associations and 95 percent confidence intervals to test statistically significant differences. For efficiency, we calculated these comparisons only for the most recent version of each survey instrument.
The SAS statistical software package (SAS Institute, Inc. 1988) was used to code variables, and the SUDAAN statistical software package (Research Triangle Institutes 1995; Shah, LaVange, Barnwell, et al. 1989) was used to yield estimates of dental visit and standard errors. We used SUDAAN because this software package takes the complex, multistage sampling design of each data source into account when it produces standard errors for confidence intervals and Z statistics.
We used full sampling weights during the analysis so that all estimates would be representative of the civilian, noninstitutionalized population of the United States. We restricted analysis to persons aged 25–59 years because all three national surveys asked persons of this age range the dental visit questions. We also limited the analysis to this age group because it encompassed the adults that were likely to be employed and have some type of dental insurance.
Utilization Estimates Within Surveys and Across Survey Years
Table 1 lists the standardized proportion of adults who reported a dental visit in the previous year, according to the NHIS. The overall proportion of persons with a dental visit increased steadily from 1986 to 1993; however, only the difference in overall dental visit proportions between the 1986 NHIS and the 1993 NHIS was statistically significant (Z=–3.30, p <0.001).
Table 1.
Age-Standardized Percentage of Adults Who Reported a DentalVisit in the Previous Year According to the National Health Interview Survey, United States, 1986, 1989, and 1993
| 1986 NHIS | 1989 NHIS | 1993 NHIS | ||||
|---|---|---|---|---|---|---|
| Characteristic | Percent | SE | Percent | SE | Percent | SE |
| Overall | 60.2 | 0.6 | 62.0 | 0.6 | 63.5 | 0.8 |
| Age | ||||||
| 25–44 years | 61.5 | 0.6 | 62.7 | 0.6 | 63.5 | 0.8 |
| 45–59 years | 57.2 | 0.8 | 60.5 | 0.8 | 63.4 | 1.0 |
| Gender | ||||||
| Men | 57.0 | 0.7 | 58.4 | 0.6 | 59.6 | 1.1 |
| Women | 63.3 | 0.6 | 65.5 | 0.6 | 67.2 | 0.7 |
| Race/ethnicity | ||||||
| Non-Hispanic White | 63.0 | 0.6 | 65.1 | 0.6 | 66.9 | 0.9 |
| Non-Hispanic Black | 46.4 | 1.1 | 48.2 | 1.3 | 51.2 | 1.5 |
| Hispanic* | 48.3 | 1.4 | 49.5 | 1.7 | 48.7 | 1.8 |
| Poverty status | ||||||
| At or above | 63.4 | 0.6 | 65.0 | 0.6 | 66.6 | 0.8 |
| Below | 37.7 | 1.2 | 36.2 | 1.3 | 39.8 | 1.9 |
| Unknown | 44.8 | 1.6 | 46.2 | 1.3 | 45.0 | 2.3 |
| Level of education | ||||||
| Less than 12 years | 39.2 | 0.9 | 38.9 | 0.9 | 40.7 | 1.7 |
| 12 years | 57.2 | 0.6 | 58.6 | 0.6 | 59.3 | 1.0 |
| Greater than 12 years | 72.5 | 0.5 | 73.6 | 0.6 | 73.8 | 0.8 |
Mexican Americans and all other persons of Latin American or Spanish descent.
Table 2 lists the age-standardized proportion of adults that reported a dental visit in the previous year, according to NHANES I and III. The overall proportion of U.S. adults with a dental visit increased significantly from 46.9 percent during 1971–1975 to either 52.4 percent or 66.9 percent during 1988–1994, depending on whether “the last year” in NHANES III included 364 or 365 days, respectively. Note that the response categories for the NHANES I questionnaire item required that the dental visit estimate be based on a time period of less than 365 days (Figure 2). Consequently, comparisons between NHANES I and NHANES III surveys should be based on the NHANES III categorization that included only 364 days in its definition (NHANES IIIa). The differences in overall dental visit proportions between NHANES I and NHANES IIIa (Z=–3.23, p <0.001) and between NHANES I and NHANES IIIb (Z=–12.86; p <0.001) were each statistically significant.
Table 2.
Age-Standardized Percentage of Adults Who Reported a DentalVisit in the Previous Year According to the National Health and Nutrition Examination Survey, United States, 1971–1975, 1988–1994
| NHANES I | NHANES IIIa | NHANES IIIb | ||||
|---|---|---|---|---|---|---|
| Characteristic | Percent | SE | Percent | SE | Percent | SE |
| Overall | 46.9 | 1.1 | 52.4 | 1.3 | 66.9 | 1.1 |
| Age | ||||||
| 25–44 years | 48.5 | 1.3 | 52.0 | 1.4 | 67.3 | 1.3 |
| 45–59 years | 43.4 | 1.5 | 53.1 | 1.8 | 65.9 | 1.5 |
| Gender | ||||||
| Men | 44.0 | 1.6 | 47.8 | 1.6 | 62.0 | 1.6 |
| Women | 49.7 | 1.2 | 56.8 | 1.5 | 71.6 | 1.2 |
| Race/ethnicity | ||||||
| Non-Hispanic White | 49.5 | 1.1 | 55.4 | 1.5 | 69.3 | 1.3 |
| Non-Hispanic Black | 25.6 | 2.6 | 39.3 | 1.4 | 58.1 | 1.4 |
| Hispanic* | — | — | 37.4 | 1.5 | 52.3 | 1.4 |
| Poverty status | ||||||
| At or above | 47.8 | 1.5 | 55.4 | 1.3 | 69.4 | 1.2 |
| Below | 22.2 | 3.6 | 28.2 | 2.1 | 44.4 | 1.9 |
| Unknown | 49.4 | 1.5 | 47.0 | 3.6 | 65.5 | 3.2 |
| Level of education | ||||||
| Less than 12 years | 31.0 | 1.6 | 33.9 | 2.0 | 48.7 | 1.9 |
| 12 years | 47.8 | 1.5 | 46.9 | 1.8 | 63.5 | 1.6 |
| Greater than 12 years | 62.2 | 1.7 | 63.8 | 1.6 | 76.7 | 1.4 |
Mexican Americans only
=Previousyear defined as including the last 364 days
=Previousyear defined as including the last 365 days
Table 3 lists the age-standardized proportion of adults who reported a dental visit in the previous year, according to the three health expenditure surveys. The proportion of U.S. adults with a dental visit remained relatively stable across survey years. There were no statistically significant differences in overall proportions among the health expenditure surveys.
Table 3.
Age-Standardized Percentage of Adults Who Reported a Dental Visit in the Previous Year According to the National Medical Care Expenditure Survey, the National Medical Expenditure Survey, and the Medical Expenditure Panel Survey, United States, 1977, 1987, and 1996
| 1977 NMCES | 1987 NMES | 1996 MEPS | ||||
|---|---|---|---|---|---|---|
| Characteristic | Percent | SE | Percent | SE | Percent | SE |
| Overall | 46.5 | 0.8 | 46.5 | 0.7 | 44.6 | 0.8 |
| Age | ||||||
| 25–44 years | 47.0 | 1.0 | 46.7 | 0.7 | 42.5 | 1.1 |
| 45–59 years | 45.5 | 1.0 | 45.9 | 0.9 | 49.4 | 0.9 |
| Gender | ||||||
| Men | 42.9 | 0.9 | 42.6 | 0.9 | 39.0 | 1.1 |
| Women | 49.8 | 0.9 | 50.1 | 0.8 | 50.0 | 0.8 |
| Race/ethnicity | ||||||
| Non-Hispanic White | 49.8 | 0.8 | 50.4 | 0.8 | 48.8 | 0.9 |
| Non-Hispanic Black | 25.6 | 1.3 | 29.0 | 1.1 | 29.8 | 1.5 |
| Hispanic* | 29.8 | 2.1 | 30.6 | 1.8 | 32.1 | 1.6 |
| Poverty status | ||||||
| At or above | 47.5 | 0.8 | 48.5 | 0.7 | 47.1 | 0.8 |
| Below | 32.6 | 1.8 | 27.7 | 1.8 | 24.5 | 1.8 |
| Unknown | — | — | — | — | — | — |
| Level of education | ||||||
| Less than 12 years | 31.2 | 1.1 | 24.9 | 1.1 | 22.2 | 1.3 |
| 12 years | 46.8 | 0.9 | 43.6 | 0.8 | 38.6 | 1.1 |
| Greater than 12 years | 60.4 | 1.1 | 58.7 | 0.9 | 54.9 | 0.9 |
Mexican Americans and all other persons of Latin American or Spanish descent.
Utilization Estimates Across Surveys
Table 4 compares the 1993 NHIS age-standardized overall dental estimate for adults with estimates from the NHANES III and MEPS data instruments. Dental visit estimates derived from the NHANES III and MEPS instruments were significantly different from those derived from the 1993 NHIS. For example, NHANES IIIa and MEPS substantially underestimated the 1993 NHIS estimate by 17 and 30 percent, respectively. Although estimates from the 1993 NHIS and NHANES IIIb were nearer, NHANES still overestimated the 1993 NHIS estimate by approximately 5 percent.
Table 4.
Comparison of the 1993 NHIS Age-Standardized Overall Dental Visit Estimate for Adults with Estimates from NHANES III and MEPS, United States, 1988–1994, 1996, and 1993
| Comparison to 1993 NHIS | NHANES IIIa | NHANES IIIb | MEPS |
|---|---|---|---|
| Percentage difference | −17.5 | 5.4 | −29.8 |
| Z-statistic | 7.27 | −2.50 | 16.71 |
| p-value | <0.001 | 0.006 | <0.001 |
a=Previous year defined as including the last 364 days
b=Previous year defined as including the last 365 days
Utilization Estimate Trends Across Surveys
Table 5 lists stratum-specific dental visit odds ratio associations for the 1993 NHIS, NHANES IIa and NHANES IIIb, and MEPS. With the exception of age, stratum-specific associations were consistent across surveys. For example, regardless of the data source, men were always significantly less likely than women. Non-Hispanic Whites were always significantly more likely than Hispanics, and persons with higher socioeconomic status (measured via poverty status and level of education) were always significantly more likely than those with low socioeconomic status to have had a dental visit in the last year. Age-specific odds ratio associations were not consistent across surveys, however. MEPS was the only data instrument showing that younger adults were significantly less likely than older adults to have had a dental visit in the last year.
Table 5.
Odds Ratio of a Dental Visit in the Previous Year by Selected Characteristics and National Survey Instrument, United States, 1993, 1988–1994, and 1996
| 1993 NHIS | NHANES IIIa | NHANES IIIb | MEPS | |
|---|---|---|---|---|
| Characteristic | Odds ratio (95% C.I.) | Odds ratio (95% C.I.) | Odds ratio (95% C.I.) | Odds ratio (95% C.I.) |
| Overall | — | — | — | — |
| Age | ||||
| 25–44 years | 1.01 (0.9, 1.1) | 0.97 (0.8, 1.1) | 1.07 (0.9, 1.2) | 0.76 (0.7, 0.8) |
| 45–59 years | Reference | Reference | Reference | Reference |
| Gender | ||||
| Men | 0.73 (0.7, 0.8) | 0.69 (0.6, 0.8) | 0.65 (0.6, 0.8) | 0.65 (0.6, 0.7) |
| Women | Reference | Reference | Reference | Reference |
| Race/ethnicity | ||||
| Non-Hispanic White | 2.15 (1.9, 2.5) | 2.14 (1.8, 2.6) | 2.11 (1.8, 2.5) | 2.27 (1.9, 2.7) |
| Non-Hispanic Black | 1.11 (0.9, 1.3) | 1.11 (0.9, 1.3) | 1.30 (1.1, 1.5) | 0.95 (0.8, 1.2) |
| Hispanic* | Reference | Reference | Reference | Reference |
| Poverty status | ||||
| At or above | 2.95 (2.5, 3.4) | 3.19 (2.6, 3.9) | 2.75 (2.3, 3.4) | 2.84 (2.4, 3.4) |
| Below | Reference | Reference | Reference | Reference |
| Unknown | 1.22 (1.0, 1.5) | 2.26 (1.5, 3.4) | 2.15 (1.5, 3.2) | — |
| Level of education | ||||
| Greater than 12 years | 4.20 (3.6, 4.9) | 3.28 (2.7, 4.0) | 3.38 (2.8, 4.0) | 4.42 (3.8, 5.2) |
| 12 years | 2.18 (1.9, 2.5) | 1.74 (1.4, 2.2) | 1.76 (1.5, 2.1) | 2.25 (1.9, 2.7) |
| Less than 12 years | Reference | Reference | Reference | Reference |
Includes Mexican Americans and all other persons of Latin American or European Hispanic descent for 1993 NHIS and MEPS, and Mexican Americans only for NHANES III
a=Previous year defined as including the last 364 days
b=Previous year defined as including the last 365 days
DISCUSSION
To date, several epidemiological investigations of oral health care utilization have been conducted in the United States, including a recent telephone survey conducted by the American Dental Association and Gallup Organization, Incorporated (American Dental Association 1998) of adult attitudes and behaviors. We only included the nationally representative NHIS, NHANES, and health expenditure surveys in this investigation, however, because these surveys used a common sampling frame. We limited the investigation to surveys with a common sampling frame so that differences in the target samples would not impact the variations noted across surveys.
This investigation showed that there was a substantial and statistically significant difference between the overall dental visit estimates derived from the standard NHIS and estimates derived from NHANES and the health expenditure surveys. The investigation also showed that despite differences in the overall estimates, relative stratum-specific dental visit associations were consistent across surveys. The consistent trends were comforting, as a policymaker who was interested, for example, in determining whether non-Hispanic Whites were more likely to report a dental visit than non-Hispanic Blacks would find identical associations, regardless of the data source used. What is disconcerting, however, is that a researcher or policymaker who used the NHIS to estimate the overall proportion of the U.S. population with a dental visit would have drawn a vastly different conclusion about utilization than the researcher or policymaker who used NHANES or the health expenditure surveys, and this difference could have had a substantial impact on program planning, estimation of necessary funds, or determination of national personnel requirements. In the remainder of this section, we discuss some of the possible explanations for these discrepancies; relate the findings to study strengths and limitations; interpret the results in terms of relevant health policy, research, public health programs; and provide general recommendations for those who regularly rely on these data.
There are a number of reasons that the health expenditure surveys consistently yielded lower utilization estimates than the standard NHIS or NHANES. These reasons can be broadly categorized into design issues and unique approaches to assessing dental visits. For example, there were differences across surveys in terms of reference periods, lead-in statements, question wording, the way to which dental professionals were referred, and social desirability. Our discussion begins with reference periods.
On average, U.S. adults report approximately two dental visits per person per year (Bloom, Gift, and Jack 1993). When questionnaire items ask a respondent to recall such infrequently occurring events, cognitive theory suggests that the respondent is more likely to count the individual events in his or her memory than to make an estimate of the number (Blair and Burton 1987; Burton and Blair 1991; Sudman, Bradburn, and Schwartz 1996a). In addition, theory indicates that there is greater uncertainty about recalling events that occurred 90 days or more ago (Burton and Blair 1991). This uncertainty results in a greater number of events that occurred outside of a specified time period being remembered as having occurred within it than otherwise—referred to as intrusion of events (Sudman, Bradburn, and Schwartz 1996b). In addition, studies of cognitive processes indicate that respondents consistently tend to overestimate the number of events when a reference period includes a period more distant in time—referred to as telescoping (Bradburn, Huttenlocher, and Hedges 1994). There is some evidence to suggest that overestimation due to telescoping may be as high as 32 percent (Bradburn, Huttenlocher, and Hedges 1994). The three surveys incorporated a variety of reference periods. For example, the NHIS asked respondents about dental visits made during a 12-month period (Figure 1), a relatively remote interval, whereas the health expenditure surveys asked about visits made during sequential 3- to 4-month periods (Figure 3), a substantially shorter period. According to cognitive theory, a respondent to the NHIS would be more likely to include events incorrectly (intrusion) and overestimate the number of events (telescoping) than would a respondent to the health expenditure surveys, and this theoretical relationship is in keeping with our findings.
It is interesting to note that the NHANES I and NHANES III dental visit items completely lacked reference periods (Figure 2). Despite this omission, however, there was still evidence of intrusion and telescoping in these surveys. We use the explicit response categories in NHANES I and the 364- and 365-day definitions of “the past year” in NHANES III to illustrate the existence of intrusion and telescoping. The response categories for NHANES I were as follows: less than 6 months ago, 6 through 11 months ago, or 1 but less than 2 years ago. Let us assume a NHANES I respondent truly visited the dentist 13 months ago. Let us also assume that the participant could not remember exactly when the visit occurred. The respondent was asked the following: “When was the last time you visited or talked with a dentist about yourself?” He or she might have responded, “About a year ago.” According to intrusion and telescoping theory, this response would have been reasonable, as the respondent would have believed (incorrectly) that his visit 13 months ago actually took place within the last year. The respondent's “about a year ago” response would subsequently have been listed under the 1 but less than 2 years ago response category by the interviewer. This response would not have been counted in a NHANES I dental visit estimate, however, as the 1 but less than 2 years ago category was not included among NHANES I dental visit calculations.
In NHANES III, where no defined response categories existed, the interviewer converted the respondent's answer to number of days. Theconversion may have led to potential differences from NHANES I. The distribution of the NHANES III data suggests that the response “about a year ago” was probably converted by the interviewer to 365 days, even though the interviewer was given specific instructions to probe such ambiguous responses (U.S. Department of Health and Human Services 1996). In contrast to dental visit estimates derived from NHANES I, this response would have been included in a dental visit calculation for NHANES III (Table 2; NHANES IIIb). In addition, changing the cut-off for annual utilization in NHANES III from 364 days to 365 days caused an increase in the overall dental visit percentage from 52 percent (NHANES IIIa) to 67 percent (NHANES IIIb). The 15 percentage point difference was an illustration of the effect that intrusion of events and telescoping might have had on the dental visit results.
A lead statement introduces a survey section by (1) asking the respondent to think of a particular event, occasion, or time frame, (2) explaining a new or difficult concept, or (3) providing transition from one section to another. Hypothetically, a lead sentence would be expected to focus the respondent's attention on particular facts or concepts pertinent to answering the survey items to follow. Given this hypothesis, one would expect that the respondent to the health expenditure surveys would be most focused, and the respondent to the NHANES data source and 1989 NHIS would be least focused. The effect that these differences might have had on the utilization estimates from each data source is unclear; however, it is likely that the health expenditure lead sentences, with their shorter reference periods, additionally helped to diminish telescoping.
An additional difference between the data sources was the general manner by which dental visit information was ascertained across surveys. For example, the NHIS asked its respondents to recall the number of dental visits made during the preceding 12 months (Figure 1). In contrast, the NHANES I and III survey instruments asked its respondents to recall their last visit to a dentist (Figure 2). Finally, the health expenditure surveys simply asked its participants to remember whether they had a dental visit in the previous 3- to 4-month time period (Figure 3). Here again, the shorter reference period in the health expenditure surveys made them less susceptible to telescoping and an overestimation of utilization.
An alternative explanation for the way that data collection might have influenced the dental visit estimates was that the NHIS and NHANES did not require the respondent to provide follow-up information about the reported dental visit, whereas the health expenditure surveys did. Specifically, the health expenditure surveys asked the respondents to describe the types of treatment services that they received and their respective costs. NHIS and NHANES asked only whether the respondent had made a dental visit. Loftus et al. (1992) suggested that respondents sometimes underreport their health care visits when they know that they will be required to provide specific follow-up information about the visit later in the survey. This caution criterion for responding could explain the lower dental visit estimates that were derived from the health expenditure surveys.
The final way the three surveys differed was in the inclusion of various types of health practitioners in the questionnaire items. One could hypothesize that a questionnaire item that included a greater number of professionals might have produced a higher utilization estimate. If this were true, then the health expenditure surveys (Figure 2) would be expected to yield the highest estimates and the NHIS (Figure 1) would be expected to yield the lowest estimates. In fact, the opposite occurred. Consequently, the inclusion of various types of practitioners in the questionnaire items was not a likely explanation for discrepancies among the estimates.
Social desirability in answering is the conscious or unconscious tendency of a survey participant to answer according to social norms and attitudes about a topic (Arleck and Settle 1995). For example, if society suggests that one should visit the dentist annually, a survey respondent might report a dental visit, even if it did not occur, because he or she does not want to appear outside the norm. Consequently, social desirability in answering would lead to an overestimation of dental visits, especially when a 1-year reference period is included in the item. In contrast, overestimation would be less likely to occur when the reference period included a period shorter than 1 year, such as was the case for the health expenditure surveys. Although social desirability is a plausible explanation for the discrepancies among the surveys, it was not possible to estimate exactly how much of the difference was due to this reason.
The surveys had a number of design elements in common. For example, each source
Used an area probability sampling method,
Used a face-to-face interview,
Used the civilian, noninstitutionalized U.S. population as the target population,
Applied the dental visit questions to a large sample size (1,000+ respondents),
Incorporated the dental visit questions as part of a larger, detailed survey instrument (approximately 1 hour for completion),
Did not use call backs to retrieve additional dental visit information after the survey, and
Did not use imputation techniques to estimate dental visit information when missing.
Given that these design elements were common to the surveys, they would not have explained discrepancies in dental visit estimates. The overall response rates were also relatively high for each of the national data sources. We did not have access to dental visit item nonresponse information for each survey and could not assess its impact on the discrepancies noted in our investigation. This investigation of oral health care utilization had a number of strengths. For example, the investigation included several national data sources, each of which was representative of the civilian, noninstitutionalized population of the United States. The study also assessed stability of estimates over time and age-standardized the dental visit estimates to a common population. Finally, the investigation compared overall and stratum-specific estimates in order to provide a more complete picture of similarities and differences across surveys.
This report also had a number of limitations. The most critical shortcoming was the surveys' inability to validate responses to utilization questions. An additional study limitation was that the time periods covered by the individual surveys were not directly comparable. Finally, the surveys applied the dental visit question to persons of specific age ranges, making a comparison of dental visit estimates for all ages impossible. We selected the lower limit of the age range for our study because NHANES I did not ask persons under 25 years of age the dental visit question. Although all of the surveys asked persons older than 59 years of age the dental visit question, we selected age 59 years as our upper age limit because oral health care utilization is highest among younger adults. Consequently, limiting the analysis to persons aged 25 through 59 years meant that we could not compare dental visit data for children and seniors; however, we believe that discrepancies across surveys would have existed among these age groups, as well.
Given differences that existed across the national surveys, public health professionals and policymakers might ask which survey should be used to derive national utilization estimates in the future. This question is difficult to answer and depends on how the estimates are to be used. In some cases, it would depend on which survey was used; in some cases, it would not. For example, if disparities in oral health care utilization by gender, race/ethnicity, poverty status, or level of education were to be documented, then any of the national surveys could be used, as stratum-specific trends were consistent across surveys. In contrast, if specific associations were to be tested, such as the relationship between dental visits and oral health care expenditures or the relationship between dental visits and oral health status, then the particular national survey that included these relevant variables must be used.
A more difficult question to consider is one in which policymakers wanted an accurate overall dental visit estimate so that financing might be planned or personnel requirements might be projected. According to our results, the least desirable source of overall dental visit estimates was NHANES because its items lacked a definite reference period, and responses were vulnerable to intrusion, telescoping, and a lack of specificity in coding between the 364- and 365-day definitions of a dental visit (NHANES III). It appears that even the standard NHIS was troublesome, as responses to the survey were subject to intrusion, telescoping, and social desirability. Although the health expenditure surveys might have underestimated dental visits due to the caution criterion, the health expenditure surveys were most desirable, as responses were less susceptible to intrusion, telescoping, social desirability, and coding ambiguities.
The NHIS has been considered the standard data source for tracking national health objectives relating to oral health care utilization. Recently, in support of our assertion that the health expenditure surveys provided a more accurate source of overall dental visit information, the U.S. Department of Health and Human Services selected MEPS instead of NHIS to track progress toward the national health objectives for 2010 (U.S. Department of Health and Human Services 2000).
The differences among these three data sources highlight the need for future studies to compare self-reported utilization data to actual utilization data among adults. Once these studies have been conducted, health services researchers will have a better understanding of the extent to which the national surveys overestimate or underestimate utilization. Although a validation study would give a better sense of “true” utilization, we do not suggest that the three national surveys incorporate validation during every administration of the survey. The additional costs would be unjustified. It is more reasonable to advise a separate, small-scale validation study to provide a standard estimate by which differences among the national surveys might be compared.
This article highlighted the differences among national dental visit estimates, alerted researchers and public policymakers to methodological issues unique to each data source, and explained why differences in utilization estimates might have occurred. Although choice of national data source depends on a specific research hypothesis, we encourage those who require overall dental visit estimates to consider following the U.S. Department of Health and Human Service's lead and switch to MEPS. We recognize the fact that without a current means to assess “true” utilization, it is impossible to know whether such a switch would underestimate utilization in the United States; however, given the issues presented in this article, cognitive theory supports the use of MEPS.
Acknowledgments
We would like to thank Doris C. Lefkowitz and Alan Monheit, at the Agency for Healthcare Research and Quality, and Jennifer Madans and Elsie Pamuk, at the NCHS, for their thoughtful review. We would also like to thank Brian Rowland and Devi Katikineni at Social and Scientific Systems, Bethesda, MD, for their skillful computer programming support. Finally, we would like to extend special thanks to Janice Poling, Intern at the Center for Cost and Financing Studies, for her input during the writing of the introduction section.
REFERENCES
- American Dental Association Survey Center. 1997 Survey of Consumer Attitudes and Behaviors Regarding Dental Issues. Chicago IL: American Dental Association; 1998. [Google Scholar]
- Arleck PD, Settle RB. The Survey Research Handbook Guidelines and Strategies for Conducting a Survey. 2d. New York: McGraw-Hill; 1995. [Google Scholar]
- Benson V, Marano MA. Current Estimates from the National Health Interview Survey 1993 National Center for Health Statistics Vital Health Stat. 190. Vol. 10. Hyattsville MD: National Center for Health Statistics; 1994. [PubMed] [Google Scholar]
- Berk ML, Bernstein A. “Use of Home Health Services: Some Findings from the National Medical Care Expenditure Survey.”. Home Health Care Services Quarterly. 1985;6(1):13–23. doi: 10.1300/J027v06n01_03. [DOI] [PubMed] [Google Scholar]
- Blair EA, Burton S. “Cognitive Processes Used by Survey Respondents to Answer Behavioral Frequency Questions.”. Journal of Consumer Research. 1987;14:280–8. [Google Scholar]
- Bloom B, Gift HC, Jack SS. Dental Services and Oral Health: United States, 1989. National Center for Health Statistics Vital Health Stat. 183. Vol. 10. Hyattsville MD: National Center for Health Statistics; 1993. DHHS Publication No. (PHS) 93-1511 [PubMed] [Google Scholar]
- Bradburn NM, Huttenlocher J, Hedges LV, Schwartz N, Sudman S. In: “Telescoping and Temporal Memory” Autobiographical Memory and the Validity of Retrospective Reports. Schwartz N, Sudman S, editors. New York: Springer-Verlag; 1994. [Google Scholar]
- Burton S, Blair EA. “Task Conditions, Response Formulation Processes, and Response Accuracy for Behavioral Frequency Questions in Surveys.”. Public Opinion Quarterly. 1991;55:50–79. [Google Scholar]
- Cohen J. Design and Methods of the Medical Expenditure Panel Survey Household Component. MEPS Methodology Report No. 1. Rockville MD: Agency for Health Care Policy and Research; 1997. AHCPR Publication No. (PHS) 97-0026 [Google Scholar]
- Cohen SB, Burt VL. “Data Collection Frequency Effect in the National Medical Care Expenditure Survey.”. Journal of Economic and Social Measurements. 1985;13(2):125–51. [PubMed] [Google Scholar]
- Edwards WS, Berlin M. Questionnaire and Data Collection Methods for the Household Survey and the Survey of American Indians and Alaska Natives, Method 2. National Medical Expenditure Survey. Rockville MD: Agency for Health Care Policy and Research; 1989. Agency for Health Care Policy and Research.DHHS Publication No. (PHS) 89-3450 [Google Scholar]
- Harper T, Berlin M, DiGaetano R, Walsh D, Ingels J. National Medical Expenditure Survey: Household Survey Final Methodology Report, Deliverable No.1.163. Rockville MD: Westat Inc; 1991. [Google Scholar]
- Jack S, Bloom B. Use of Dental Services and Dental Health: United States, 1986. National Center for Health Statistics. Vital Health Stat. 165. Vol. 10. Washington DC: Government Printing Office; 1988. DHHS Publication No. (PHS) 88-1593 [PubMed] [Google Scholar]
- Loftus EF, Smith KD, Klinger MR, Fiedler J, Tanur JM. “Memory and Mis-memory for Health Events.”. In: Tanur JM, editor. Questions about Questions Inquiries into Cognitive Bases of Surveys. New York: Russell Sage Foundation; 1992. [Google Scholar]
- Massey JT, Moore TF, Parsons VL, Tadros W. Design and Estimation for the National Health Interview Survey, 1985–1994. National Center for Health Statistics Vital Health Stat. 110. Vol. 2. Hyattsville MD: National Center for Health Statistics; 1989. DHHS Publication No. (PHS) 89-1384 [Google Scholar]
- Miller HW. Plan and operation of the National Health and Nutrition Examination Survey, 1971–1973 Vital Health Stat. Vol. 1. Hyattsville MD: National Center for Health Statistics; 1977. (10a and 10b) [PubMed] [Google Scholar]
- Research Triangle Institute. SUDAAN User's Manual: Software for the Statistical Analysis of Correlated Data. Research Triangle NC: Author; 1995. [Google Scholar]
- SAS Institute Inc. SAS/STAT User's Guide, Release 6.03 Edition. Cary NC: Author; 1988. [Google Scholar]
- Shah BV, LaVange LM, Barnwell GB, Killinger JE, Wheeless SC. Software for Survey Data Analysis. Research Triangle Park NC: Research Triangle Institute; 1989. [Google Scholar]
- Sudman S, Bradburn NM, Schwartz N, editors. “Counting and Estimation” Thinking about Answers. The Application of Cognitive Processes to Survey Methodology. San Francisco CA: Josey-Bass; 1996a. [Google Scholar]
- Sudman S, Bradburn NM, Schwartz N, editors. “Event Dating” Thinking About Answers. The Application of Cognitive Processes to Survey Methodology. San Francisco CA: Josey-Bass; 1996b. [Google Scholar]
- U.S. Department of Health and Human Services Public Health Service National Center for Health Service Research. National Health Care Expenditures Study, NMCES Household Interview Instruments, Instruments and Procedures 1. Hyattsville MD: National Center for Health Services Research; 1981. DHHS Publication No. (PHS) 81-3280 [Google Scholar]
- U.S. Department of Health and Human Services Public Health Service National Center for Health Service Research. Healthy People 2000 Review, 1997. Hyattsville MD: National Center for Health Statistics; 1997. National Center for Health Services Research. [Google Scholar]
- U.S. Department of Health and Human Services Public Health Service National Center for Health Service Research. Tracking Healthy People 2010. Washington DC: U.S. Government Printing Office; 2000. [Google Scholar]
- U.S. Department of Health and Human Services National Center for Health Statistics. Plan and Operation of the Third National Health and Nutrition Examination Survey, 1988–1994 Vital Health Stat. 32. Vol. 1. Hyattsville MD: National Center for Health Statistics; 1994. DHHS Publication No. 94-1308 [PubMed] [Google Scholar]
- U.S. Department of Health and Human Services National Center for Health Statistics. NHANES III Reference Manuals and Reports (CD-Rom version) Hyattsville MD: National Center for Health Statistics; 1996. [Google Scholar]