

Abstract
The primary aim of the Trial of Activity in Adolescent Girls (TAAG) is to test an intervention to reduce by half the age-related decline in moderate to vigorous physical activity (MVPA) in middle school girls. The intervention will be evaluated using a group-randomized trial involving 36 middle schools. The primary endpoint is the mean difference in intensity-weighted minutes (i.e., MET-minutes) of MVPA between intervention and comparison schools assessed using accelerometry.
The TAAG study design calls for two cross-sectional samples, one drawn from 6th graders at the beginning of the study and the second drawn from 8th graders at the end of the study following the 2-year implementation of the intervention. An important strength of this design over a cohort design is the consistency with the goals of TAAG, which focus on environmental-level rather than individual-level interventions to produce change. The study design specifies a recruitment rate of 80% and a smaller sample of girls at baseline (n=48 per school) than at follow-up (n=96 per school).
A two-stage model will be used to test the primary hypothesis. In the first stage, MET-weighted minutes of MVPA will be regressed on school, time (baseline or follow-up), their interaction, ethnicity and week of data collection. The second stage analysis will be conducted on the 72 adjusted means from the first stage. In the main-effects model, we will regress the follow-up school mean MET-weighted minutes of MVPA on study condition, adjusting for the baseline school mean.
The TAAG study addresses an important health behavior, and also advances the field of group-randomized trials through the use of a study design and analysis plan tailored to serve the main study hypothesis.
Keywords: Accelerometry, Cross-sectional design, Intervention, Middle School, Group-randomized trial, Physical activity
1. Introduction
National recommendations have encouraged both children and adults to promote health by being physically active [1–4]. Healthy People 2010 guidelines recommend that adolescents participate in moderate-intensity physical activity for at least 30 min on 5 or more days per week or engage in at least 20 min of vigorous activity at least three times per week [5]. National surveys consistently demonstrate that boys are more active than girls, that physical activity levels decline throughout adolescence and that the decline is particularly dramatic among girls. The 1995 National Youth Risk Behavioral Survey (YRBS) found that 64% of high school students and 52% of high school females met recommended levels for vigorous activity, and 25% of high school students reported no vigorous activity [1]. Kimm and colleagues reported a 9.6% decline in physical activity in girls from 11.5 to 12.5 years and a 12.8% decline from 12.5 to 13.5 years of age [6].
Schools can be an efficient venue for providing lifestyle-oriented physical activity instruction; however, programs to increase overall physical activity may not be effective without partnership and support from families, communities, and authoritative bodies [7]. Adolescents in middle school are influenced by both their peers and their families, indicating a stage in which integrative interventions are appropriate. Compared to boys, adolescent girls prefer different activities, tend to participate in physical activity for different reasons, and may face different barriers. For example, data from the Youth Risk Behavior Survey indicated that 74.4% of boys engaged in vigorous activities in the previous 7 days compared with 52.1% of girls [8]. Furthermore, 54% of girls compared with 23% of boys had engaged in aerobics or dancing, whereas 62% of boys and 30% of girls played basketball, football, or soccer [1]. Boys are more likely to report motivators for physical activity as an opportunity for competition, recognition, strength enhancement, and an opportunity for solitude than girls, whereas girls are more likely to report weight management as a motivator [9]. This information suggests that in order to be effective in girls, interventions should be designed specifically for girls [1,9–11].
In response to the documented need to foster physical activity levels of adolescent girls, the National Heart, Lung, and Blood Institute initiated the Trial of Activity in Adolescent Girls (TAAG), a multi-center group-randomized trial. The primary aim of TAAG is to determine if an intervention that provides opportunities for physical activity by linking schools to community organizations can reduce the age-related decline in moderate to vigorous physical activity (MVPA) in middle school girls. The primary endpoint for evaluating the intervention is the mean difference in intensity-weighted minutes (i.e., MET-minutes) of moderate-to-vigorous physical activity between girls in intervention and comparison schools. We hypothesize that the mean daily MET-weighted minutes of MVPA will be 15.6 units higher in girls in the intervention schools compared to the controls. This effect is a 10% difference in the mean level (156.4 MET-weighted minutes) measured in a preliminary study [12]. Since levels of MVPA have been shown to decline approximately 20% in girls between 6th and 8th grades [6,13], this represents an approximate 50% reduction in the expected decline. MET-minutes of MVPA are assessed using an accelerometer (Actigraph, Manufacturing Technologies, http://www.mtiactigraph.com). Secondary aims include testing the effects of the intervention on intermediate factors at the individual (student) and environmental (school and community) levels, as well as maintenance of the intervention effect one year after the intervention ceases.
The National Heart, Lung, and Blood Institute (NHLBI) is participating in and sponsoring this project, which is funded under cooperative agreements. Six universities were awarded funds to establish field centers in the vicinities of Washington, D.C. and Baltimore, Maryland (University of Maryland); Columbia, South Carolina (University of South Carolina); Minneapolis, Minnesota (University of Minnesota); New Orleans, Louisiana (Tulane University); Tucson, Arizona (University of Arizona); and San Diego, California (San Diego State University). The Coordinating Center is at the University of North Carolina, Chapel Hill.
The purposes of this paper are to: 1) describe and give the rationale for the study design and sampling approach for the primary outcome variable, 2) address assessment of mediators and moderators, 3) present the randomization and sampling strategies, and 4) describe the analysis plan.
2. Study design and sampling approach for the primary outcome variable
The dramatic decline in adolescent physical activity begins to occur at ages corresponding to the middle school years (6th, 7th, and 8th grades). Thus, a school- and community-linked intervention trial was designed to fit this 3-year time frame. We anticipated that measures of variables of interest would be obtained before and after an intervention of approximately 2 years’ duration. Furthermore, the units of randomization were schools rather than individuals because the nature of the intervention was to increase opportunities for physical activity by initiating changes in the schools’ curricula and environment and to link schools with community partners to foster additional opportunities for physical activity. Schools have been used as the unit of randomization in many studies as reviewed by Resnicow and Robinson [14]. Within the framework of a group (i.e., school) randomized trial, the TAAG study investigators considered several sampling alternatives for the primary outcome. The three given the most attention were:
A closed cohort with baseline measurements in 6th grade and final measurements in the same girls at 8th grade.
Two cross-sectional samples, one drawn from 6th graders prior to the beginning of the intervention and the second drawn from 8th graders following the 2-year implementation of the intervention.
Two cross-sectional samples, one drawn from 8th graders prior to the beginning of the intervention and the second drawn from 8th graders following the 2-year implementation of the intervention.
The closed cohort design (alternative 1) is a popular design that has been used in several trials testing the effectiveness of health promotion interventions in schools. Two such trials include the Trial for Cardiovascular Health (CATCH) [15,16] and the Pathways study [17,18]. A strength of the closed cohort design is that each participant has variables of interest measured at both baseline and endpoint. Endpoint measures can be adjusted for individual-level baseline values, and the precision of the analysis is often increased as a result. This adjustment can be important when the within-individual correlation over time is likely to be high. A weakness in the closed cohort design in school-based trials is that many participants are likely to be lost to follow-up. Based on data from the selected schools, TAAG estimated that approximately 36% of the girls present at baseline are likely to have changed schools 2 years later at the time of the follow-up measurements.
The classic intention-to-treat analysis of a randomized clinical trial includes all randomized individuals in the groups to which they were assigned, regardless of the treatment they actually received [19]. In a study such as TAAG, efforts to obtain a complete set of measurements on the girls assigned to each treatment condition would require considerable resources, as it is expensive to track and measure students who have left a school. Furthermore, despite extraordinary efforts, ascertainment of measurements in every girl in the cohort is unlikely [20].
The choice of the optimum method of dealing with this loss to follow-up inspires debate among scholars from different disciplines. Many school-based trials have ignored loss to follow-up and done what is called a “completers” analysis. For example, in the Planet Health Project [21] for the primary outcomes (prevalence, incidence, and remission of obesity) the cohort was defined as those students with data at both baseline and follow-up. Two years after baseline, follow-up data were obtained on 83% of the original cohort. Main reasons for lack of follow-up data included school transfer (52%), school absence (27%), and child refusal (10%). The analysis of the Child and Adolescent Trial for Cardiovascular Health (CATCH) study also ignored students who were lost to follow-up, but extraordinary efforts were made to obtain measurements on children who had moved within a 100-mile radius of their school [15,16]. The primary outcome (plasma cholesterol) was measured in 90% of students in a CATCH school at endpoint and 50% of students who had migrated out, for an overall measurement rate of 79%.
The Pathways study [18] obtained primary outcome (percent body fat) measurements on 83% of the 5th grade students who were randomized in the 3rd grade. However, in contrast to the trials cited above, missing data were replaced using a multiple imputation procedure that substituted predicted values from a regression equation. This equation used coefficients estimated from observed follow-up and baseline values in students in the control schools [22]. This method provided a conservative estimate based on the assumption that children lost to follow-up in both intervention and control groups had an experience like that of children in control schools. In the Pathways study, estimates with or without the imputation were almost identical, as there was no effect of the intervention on percent body fat [18].
The two cross-sectional sampling approaches (alternatives 2 and 3) have the advantage of avoiding loss to follow-up caused by students leaving the school. In the case of TAAG, a cross-sectional sample of 8th grade girls would include those who do not change schools, as well as those who do change schools (in-migration after baseline). Thus the generalizability is increased by including both types of girls, i.e., transient and non-transient. In addition, cross-sectional samples can provide a school-level estimate of the primary outcome, which conceptually matches the group-randomization design. Girls who enroll in a TAAG school after baseline will receive the intended 2-year intervention for varying lengths of time. Although the rather large percentage of students who change schools during the trial would not create missing data in a cross-sectional design, it remains unlikely that all girls selected to be part of the cross-sectional sample would actually be measured. Thus there would still be some missing data, but as a result of incomplete recruitment rather than as a result of drop out from a closed cohort.
As mentioned above, a weakness of cross-sectional designs is that baseline measurements would not be available for each girl, although school-level information on the primary outcome and other variables would be available. Cross-sectional sampling may be preferred over a cohort if the cost of follow-up is high and the power gain due to repeat measurements on the same participants is low [23]. We conducted analyses to compare the power of a design that included cross-sectional sampling of 6th and 8th grade girls to that of sampling a cohort at 6th grade girls and repeating measures on those girls in 8th grade (Table 1). We examined an intervention effect of 15.6 MET-minutes of MVPA assuming three different levels of intraclass correlation (ICC). For the cohort, data for girls lost through attrition are replaced using the response of the control condition. For the cross-sectional sampling we assumed that the amount of in-migration of girls matched out-migration and that girls who were not present in the school at baseline receive on average 60% of the full intervention effect. This was an estimate of the amount of exposure based on the experience of the intervention staff. For the cohort, we assumed girl- and school-level correlations of 0.3 and 0.2, respectively; for the cross-sectional sampling, we conservatively assumed both correlations to be zero, although we do expect some modest school-level correlation. We found that the decrease in power associated with imputation for attrition was appreciably larger than the gain in power from having the baseline values of physical activity for each girl, largely because the school- and girl-level over time correlations for physical activity were expected to be low. In addition, the method of dealing with loss to follow-up from the cohort was conservative. In total, the power to detect a difference of a given size was better for the cross-sectional than for the cohort sampling approach.
Table 1.
Comparison of power of cohort design and cross-sectional design to detect effects of the TAAG intervention on MET-weighted minutes of MVPA*
| Estimates |
||||
|---|---|---|---|---|
| Design | Description | Assumptions | ICC | Power (%) |
| Cohort | Follow a cohort of 6th grade girls measured at baseline through the end of the 8th grade. | 96 girls participate in the baseline survey. The over time correlation for girls is 0.3 and for schools is 0.2. Attrition is 36%. For both conditions, girls lost to follow-up are analyzed as though they were in the control group. | 0.010 0.003 0.000 |
64 85 94 |
| Cross-sections | Independent random samples at 6th grade and 8th grade. | 96 girls participate in both the baseline and follow-up surveys. The over time correlations for girls and for schools are 0. Girls who are present only during the 8th grade will receive 60% of the full intervention. | 0.010 0.003 0.000 |
87 97 99 |
Sampling alternative 3 (two 8th grade cross-sectional samples) has the advantage of focusing all the analyses on 8th grade girls so that secular trends in outcomes among 8th grade girls could be assessed in the baseline and endpoint measures in the control schools. One weakness of alternative 3, which is not shared by the other two approaches, is that there would be no assessment of change in physical activity levels from 6th to 8th grade. Since the primary goal of the TAAG project is to reduce the decline in physical activity levels between the 6th and 8th grades by half, this seemed a significant loss.
An important strength of the cross-sectional over the cohort sampling approach is the consistency with the goals of TAAG, which focus on environmental-level rather than individual-level interventions to produce change. In TAAG the unit to which the intervention is applied is the school, not the girl. This consideration led the TAAG investigators to favor a cross-sectional rather than a cohort design. Observation of change in physical activity levels between 6th and 8th grade in the control and treatment conditions was considered of more interest than observation over sets of 8th grade girls. Therefore, the cross-sectional alternative 2 was chosen as the primary sampling approach for the TAAG study, i.e., two cross-sectional samples, one drawn among 6th graders at the beginning of the study and the second drawn from 8th graders at the end of the study following the 2-year implementation of the intervention.
A second, post-treatment follow-up assessment is planned in 8th grade students one year after the active intervention phase ends. The purpose of this assessment is to evaluate the sustainability of TAAG intervention in the schools in which it was delivered, rather than in the students who have progressed into other schools. If TAAG intervention components have been institutionalized at the school and community levels, girls in those schools should continue to exhibit positive physical activity behaviors and outcomes beyond the intervention phase funded by the research grant. Assessment of sustainability is an important element in this study design, as it guides the TAAG intervention to consider not only efficacy but also effectiveness as an intervention goal. The overall study design is illustrated in Fig. 1.
Fig. 1.
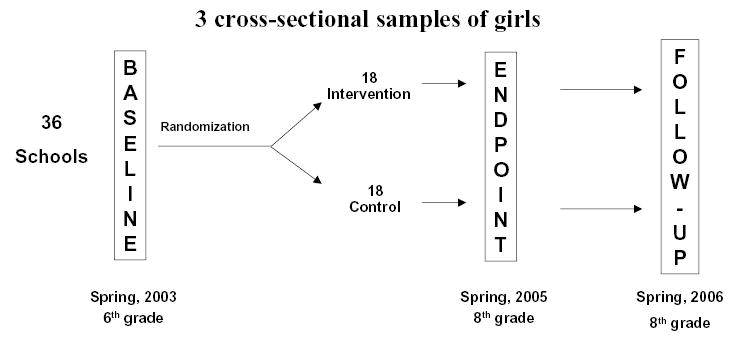
TAAG study design.
3. Approach to assessment of process, mediators, and moderators
To be able to interpret and explain TAAG study outcomes, it is useful to examine information on the implementation of the intervention and hypothesized mediators and moderators. An extensive collection of process variables has been collected in TAAG to document implementation of the intervention. This information is summarized throughout the trial and provided to the investigators to provide intervention quality control. Mediators are variables that are hypothesized to lie in the causal pathway between the intervention activities and the outcomes. The TAAG intervention is expected to be effective because of success in positively influencing mediators. The TAAG conceptual model proposes a social ecological approach whereby intervention activities positively influence girls’ levels of MVPA by affecting physical and social environment and by enhancing intrapersonal psychosocial influences in the girls [24]. Mediators of change include attributes of the physical environment as well as attributes of the girls. A hypothesized environmental mediator is the number of physical activity programs available to students outside of the school day, a number which the intervention aims to increase. These mediators are measured at the school level using previously validated assessment techniques [25], and instruments designed specifically for TAAG. Intra-individual mediators include those psychosocial variables that are expected to change as a result of the TAAG intervention; data for these hypothesized mediators are obtained using self-report. Several girl-level mediators and moderators that will be examined in TAAG are listed in Table 2.
Table 2.
Hypothesized girl-level mediators and moderators measured in TAAG
Mediators:
|
Moderators:
|
Three types of analyses on mediating variables will be informative [26,27]. The first will ascertain whether or not the proposed mediating variable was changed by the intervention. The mediating variable is treated as an outcome, and differences are compared in girls in the intervention versus the control schools. In the second type of analysis, we will determine whether the mediators are related to the primary endpoint. In the third type of analysis, we will assess whether a proposed mediator variable helps to explain changes in an outcome variable previously attributed to the intervention.
For mediators measured in individual girls, it is useful to be able to link baseline and endpoint measures within girls because the within-girl-over-time correlation of those variables is likely to be substantial. Therefore, a closed cohort design was chosen to evaluate the individual-level mediators. All girls who were in the baseline cohort and are still present in the school in 8th grade are re-measured and their data used in the individual-level mediation analyses.
Moderators are variables that are not targeted or expected to change as a result of the intervention, but may influence outcomes or may interact with the intervention resulting in differential outcome measures by subgroups. We will examine moderators in secondary analyses, however, we are aware that the power to detect effect modification (interactions) will be low. The TAAG investigators judged that it would be desirable to detect effect modification if one stratum had an effect twice as large as the other stratum. For example, an average intervention effect of 10% could be associated with stratum-specific effects of 6.67% and 13.34%, respectively, to define a minimum detectable difference between the strata of 6.67% (=13.34%–6.67%). We estimate that power for girl-level effect modification will fall between 34% and 59%, while power for school-level effect modification will be between 18% and 32%.
The reasons for the low levels of power are several, including: (1) The effect judged large enough to be important is smaller for effect modification than for the primary analysis (6.67% vs. 10%). (2) For two levels of an effect modifier, the effect of interest is defined as the net difference upper(I–C)–lower(I–C), where upper and lower refer to those above and below the study-wide median on the effect modifier and I and C refer to the intervention and control conditions, respectively; this effect involves four means compared to just two in the primary analysis, thereby increasing the standard error, other factors constant. (3) With girl-level effect modification, the number of girls per condition × stratum × site is only half what it was per condition × site in the primary analysis. (4) With school-level effect modification, the number of schools per condition × stratum × site is reduced by half compared to the number per condition × site in the primary analysis.
4. Randomization and sample size
The unit of randomization is the school. Public middle schools (grades 6–8) were eligible if the majority of children enrolled lived in the community served by the school, so that the community component of the intervention would be relevant to them. Specific school and student exclusion criteria are listed in Table 3. Randomization was stratified by field center and by school district. For school districts with an even number of schools, schools were randomized to intervention or control conditions in equal numbers. For those with an odd number of schools, one school least well matched on socioeconomic factors and recruitment rate was grouped with similarly mismatched schools from other school districts that had an odd number of schools.
Table 3.
Exclusion criteria in the TAAG trial
School exclusion criteria
|
Student exclusion criteria
|
The sample size per school was selected to provide approximately 90% power to detect an absolute difference in MVPA of 10% at the end of the two years of the trial. Details of the power analysis are provided elsewhere [24]. In each of 36 schools (6 per field center), 60 randomly selected sixth grade girls were invited at baseline to be measured with a goal of measuring of at least 80% (48) of those girls. At the end of the 2-year intervention (end point) and in the subsequent year (follow-up), 120 randomly selected eighth grade girls per field center will be invited to participate in the measurements. Again, we will attempt to obtain measurements on at least 80% (96) of those invited to participate.
TAAG was designed such that the sample size for girls at baseline is approximately half as large as the sample size for girls at endpoint and follow-up. This smaller sample size at baseline results in a considerable cost-savings (allowing for greater resources for other study-related activities) with a negligible reduction in power for the primary hypothesis (less than 1% decline in power assuming the ICC=0.01). The effect of the smaller baseline sample is to reduce the magnitude of reduction in error variance due to regression adjustment because the baseline means are estimated with less precision. Even with a reduced sample at baseline, one can still control for potential confounding in the unlikely event that treatment conditions are not balanced on important prognostic factors at baseline. Also, in a school-randomized study, power is largely driven by the number of schools, and is less influenced by the number of girls per school.
5. Analysis plan
The primary analysis for TAAG will be conducted in two stages as though there is no overlap among girls measured in the 6th and 8th grade cross-sectional samples. This two-stage approach avoids many complexities inherent in a single-stage mixed-model regression analysis from a multi-center group randomized trial, including simultaneous estimation of multiple random effects and distributional assumptions for those effects [28]. It mimics an analysis of covariance performed on 8th grade data with regression adjustment for 6th grade values.
In the first stage, the girls’ MET-weighted minutes of moderate-to- vigorous physical activity (MVPA) will be regressed on school, time (baseline or follow-up), their interaction, ethnicity, and week of data collection; study condition will not be included in that model:
| (1) |
Here, all terms will be fixed effects, except for week and residual error, to allow for correlation among girls measured in the same week and for random variation among girls. Of interest in this first stage is the estimation of ethnicity-adjusted school means for MET-weighted minutes of MVPA, estimated for each school at 6th grade and at 8th grade. Adjustment for ethnicity will be accomplished in a pooled analysis of 6th and 8th grade data, rather than in separate analyses, to standardize results for the two surveys against the same reference distribution, here the average ethnicity distribution over time. Analysis of pilot and baseline data indicates that adjustment for ethnicity serves to reduce the ICC and thereby increase power. The result of the first stage will be 2 adjusted means for each of the 36 schools.
The second stage analysis will be conducted on the 72 adjusted means from the first stage. In a preliminary step, we will look for evidence of a differential effect of the intervention among the six sites by testing for an interaction between site and condition. If there is a significant interaction, the data cannot be pooled across sites and instead the results will be reported separately for each site. However, we do not anticipate a significant interaction, in which case we will remove the interaction term and proceed with a main-effects model.
In the main-effects model, we will regress the follow-up school mean MET-weighted minutes of MVPA on study condition, adjusting for baseline school mean:
| (2) |
Here, condition and baseline MVPA are fixed effects while site and school are random effects, there is no residual error beyond school, and we use the term school instead of residual error to avoid confusion between Eq. (1) and Eq. (2). Given a proper randomization and a well-executed study, this model provides an unbiased test of the intervention effect. It also provides the statistical basis for inferences to sites and schools like those included in TAAG [24].
6. Conclusion
The TAAG study design was based on considerations from field experiences and results of other group-randomized trials. The group-randomized design and cross-sectional sampling approach are congruent with the conceptual approach of the intervention, which intervenes on the entire school. It also is consistent with practical considerations of the high level of student in- and out-migration that is common in the middle school years. The design was dictated by the specific aims; it allows an integrative examination of environmental, school-level, and individual-level variables. In conclusion, the TAAG study not only addresses an important health behavior, but the design also advances the field of group-randomized trials.
References
- 1.US Department of Health and Human Services. Physical Activity and Health: A Report of the Surgeon General. Atlanta: US Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Chronic Disease Prevention and Health Promotion; 1996.
- 2.Pate R, Pratt M, Blair S, et al. Physical activity and public health: a recommendation from the Centers for Disease Control and prevention and the American college of sports medicine. JAMA. 1995;273:402–7. doi: 10.1001/jama.273.5.402. [DOI] [PubMed] [Google Scholar]
- 3.NIH Consensus Development Conference on Physical Activity and Cardiovascular Health. Physical activity and cardiovascular health. JAMA. 1996;276:241–6. [PubMed] [Google Scholar]
- 4.US Department of Health and Human Services. Healthy People 2000. National Health Promotion and Disease Prevention Objectives. Washington, DC: US Department of Health and Human Services; 1990.
- 5.US Department of Health and Human Services. Healthy People 2010: National Health Promotion and Disease Prevention Objectives. Atlanta: US Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Chronic Disease Prevention and Health Promotion; 2000.
- 6.Kimm S, Glynn N, Kriska A, et al. Longitudinal changes in physical activity in a biracial cohort during adolescence. Med Sci Sports Exerc. 2000;32:1445–54. doi: 10.1097/00005768-200008000-00013. [DOI] [PubMed] [Google Scholar]
- 7.National Center for Chronic Disease Prevention and Health Promotion, Center for Disease Control and Prevention. Guidelines for school and community programs to promote lifelong physical activity among young people. J Sch Health. 1997;67:202–19. doi: 10.1111/j.1746-1561.1997.tb06307.x. [DOI] [PubMed] [Google Scholar]
- 8.CDC. Youth risk behavior surveillance—United States. MMWR. 1996;45:SS–4. [PubMed] [Google Scholar]
- 9.Tappe M, Duda J, Ehnrwald P. Perceived barriers to exercise among adolescents. J Sch Health. 1989;59:153–5. doi: 10.1111/j.1746-1561.1989.tb04689.x. [DOI] [PubMed] [Google Scholar]
- 10.Garcia A, Broda M, Frenn M, et al. Gender and developmental differences in exercise beliefs among youth and prediction of their exercise behavior. J Sch Health. 1995;65:213–9. doi: 10.1111/j.1746-1561.1995.tb03365.x. [DOI] [PubMed] [Google Scholar]
- 11.Godin G, Shephard R. Psychosocial factors influencing intentions to exercise of young students from grades 7 to 9. Res Q Exerc Sport. 1986;57:41–52. [Google Scholar]
- 12.McLeroy K, Bibeau D, Stecker A, Glanz K. An ecologic perspective on health promotion programs. Health Educ Q. 1988;15:351–77. doi: 10.1177/109019818801500401. [DOI] [PubMed] [Google Scholar]
- 13.Trost S, Pate R, Freedson P, Sallis J, Taylor W. Using objective physical activity measures with youth: how many days of monitoring are needed? Med Sci Sports Exerc. 2000;32:426–31. doi: 10.1097/00005768-200002000-00025. [DOI] [PubMed] [Google Scholar]
- 14.Resnicow K, Robinson T. School-based cardiovascular disease prevention studies: review and synthesis. Ann Epidemiol. 1997;7:S14–31. [Google Scholar]
- 15.Luepker R, Perry C, McKinlay S, et al. Outcomes of a field trial to improve children’s dietary patterns and physical activity. The Child and Adolescent Trial for Cardiovascular Health (CATCH) JAMA. 1996;275:768–76. doi: 10.1001/jama.1996.03530340032026. [DOI] [PubMed] [Google Scholar]
- 16.Zucker D, Lakatos E, Webber L, et al. Statistical design of the child and adolescent trial for cardiovascular health (CATCH): implications of cluster randomization. Control Clin Trials. 1995;16:96–118. doi: 10.1016/0197-2456(94)00026-y. [DOI] [PubMed] [Google Scholar]
- 17.Davis S, Going S, Helitzer D, et al. Pathways: a culturally appropriate obesity-prevention program for American Indian schoolchildren. Am J Clin Nutr. 1999;69:796S–802S. doi: 10.1093/ajcn/69.4.796S. [Suppl.] [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Caballero B, Clay T, Davis S, et al. Pathways: a school-based, randomized controlled trial for the prevention of obesity in American Indian schoolchildren. Am J Clin Nutr. 2003;78:1030–8. doi: 10.1093/ajcn/78.5.1030. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Hill A, Hill I. Bradford Hill’s Principles of Medical Statistics. London: Edward Arnold; 1991.
- 20.Pirie P, Thomson S, Mann S, et al. Tracking and attrition in longitudinal school-based smoking prevention research. Prev Med. 1989;18:249–56. doi: 10.1016/0091-7435(89)90072-8. [DOI] [PubMed] [Google Scholar]
- 21.Gortmaker S, Cheung L, Peterson K, et al. Impact of a school-based interdisciplinary intervention on diet and physical activity among urban primary school children. Arch Pediatr Adoles Med. 1999;153:975–83. doi: 10.1001/archpedi.153.9.975. [DOI] [PubMed] [Google Scholar]
- 22.Hunsberger S, Murray D, Davis C, Fabsitz R. Imputation strategies for missing data in a school-based multi-centre study: the Pathways study. Stat Med. 2001;20:305–16. doi: 10.1002/1097-0258(20010130)20:2<305::aid-sim645>3.0.co;2-m. [DOI] [PubMed] [Google Scholar]
- 23.Feldman H, McKinlay S. Cohort versus cross-sectional design in large field trials: precision, sample size, and a unifying model. Stat Med. 1994;13:61–78. doi: 10.1002/sim.4780130108. [DOI] [PubMed] [Google Scholar]
- 24.Murray D, Catellier D, Hannan P, et al. School-level intraclass correlation for physical activity in adolescent girls. Med Sci Sports Exerc. 2004;36:876–82. doi: 10.1249/01.mss.0000126806.72453.1c. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.McKenzie T, Sallis J, Nader P. SOFIT: system for observing fitness instruction time. J Teach Phys Educ. 1992;62:195–205. [Google Scholar]
- 26.MacKinnon D, Lockwood C. Advances in statistical methods for substance abuse prevention research. Prev Sci. 2003;4:155–71. doi: 10.1023/a:1024649822872. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.MacKinnon D, Taborga M, Morgan-Lopez A. Mediation designs for tobacco prevention research. Drug Alcohol Depend. 2002;68:S69–83. doi: 10.1016/s0376-8716(02)00216-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Murray D. Design and Analysis of Group-Randomized Trials. New York: Oxford University Press; 1998.