

Abstract
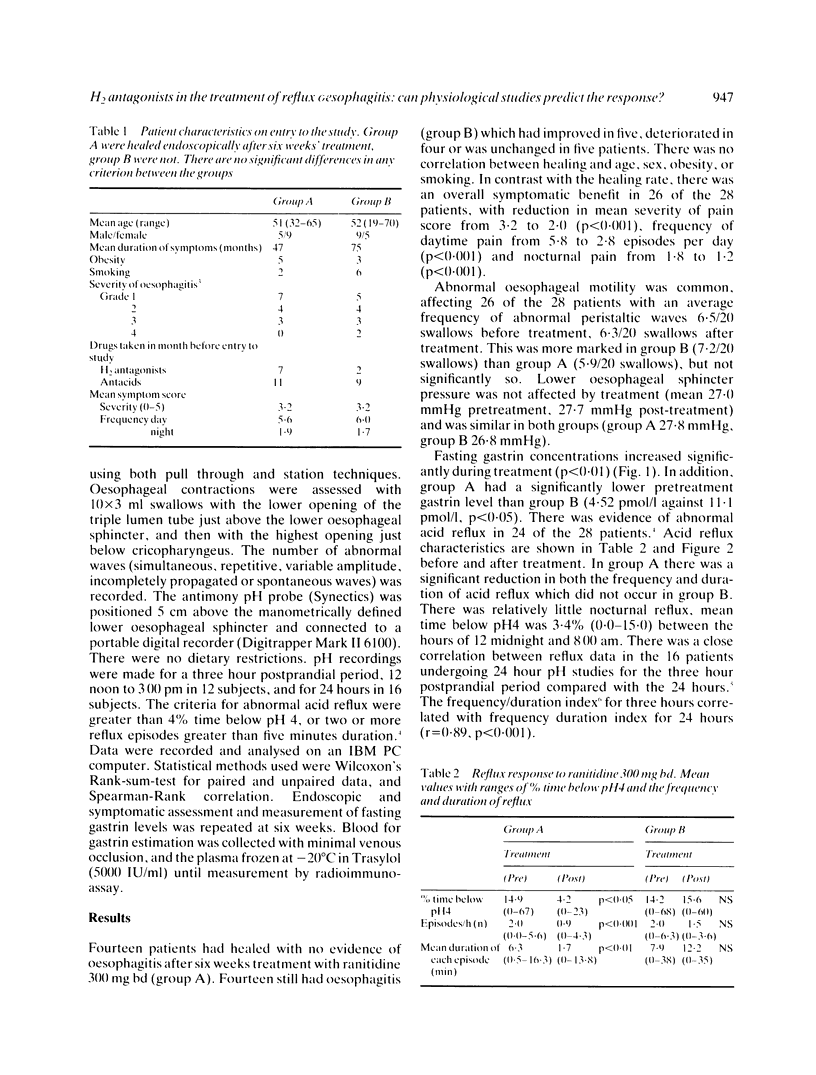
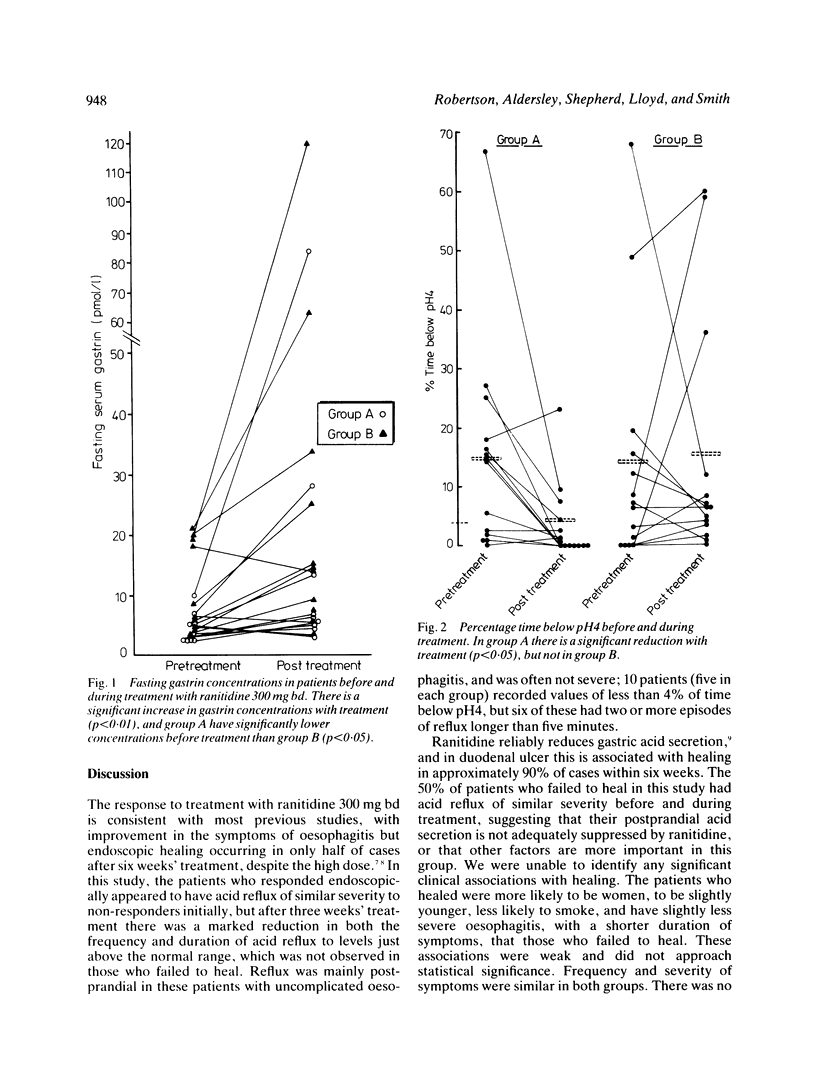
Ambulatory oesophageal pH, oesophageal manometry and fasting serum gastrin concentrations were carried out on 28 patients with reflux oesophagitis, before and during treatment with ranitidine 300 mg bd. Fourteen patients healed endoscopically at six weeks (group A) and 14 had residual oesophagitis (group B). Group A were characterised by a lower serum gastrin concentration before treatment (4.52 pmol/l; 2.4-10: mean and range) than group B (11.1 pmol/l; 3.5-21: p less than 0.05) and showed a marked reduction in acid reflux on treatment to near normal values. Mean per cent time below pH4 fell from 14.9 to 4.2 in group A (p less than 0.05) but was not affected in group B (14.2-15.6, not significant). Abnormal oesophageal motility was found in 13 patients from each group. This did not inhibit the response to ranitidine, and was not improved by healing of oesophagitis.
Full text
PDF

Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Branicki F. J., Evans D. F., Jones J. A., Ogilvie A. L., Atkinson M., Hardcastle J. D. A frequency-duration index (FDI) for the evaluation of ambulatory recordings of gastro-oesophageal reflux. Br J Surg. 1984 Jun;71(6):425–430. doi: 10.1002/bjs.1800710607. [DOI] [PubMed] [Google Scholar]
- DeMeester T. R., Wang C. I., Wernly J. A., Pellegrini C. A., Little A. G., Klementschitsch P., Bermudez G., Johnson L. F., Skinner D. B. Technique, indications, and clinical use of 24 hour esophageal pH monitoring. J Thorac Cardiovasc Surg. 1980 May;79(5):656–670. [PubMed] [Google Scholar]
- Fink S. M., McCallum R. W. The role of prolonged esophageal pH monitoring in the diagnosis of gastroesophageal reflux. JAMA. 1984 Sep 7;252(9):1160–1164. [PubMed] [Google Scholar]
- Gill R. C., Bowes K. L., Murphy P. D., Kingma Y. J. Esophageal motor abnormalities in gastroesophageal reflux and the effects of fundoplication. Gastroenterology. 1986 Aug;91(2):364–369. doi: 10.1016/0016-5085(86)90570-6. [DOI] [PubMed] [Google Scholar]
- Goodall R. J., Temple J. G. Effect of cimetidine on lower oesophageal sphincter pressure in oesophagitis. Br Med J. 1980 Mar 1;280(6214):611–612. doi: 10.1136/bmj.280.6214.611. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Olsen A. M., Schlegel J. F. Motility disturbances caused by esophagitis. J Thorac Cardiovasc Surg. 1965 Nov;50(5):607–612. [PubMed] [Google Scholar]
- Rattan S., Coln D., Goyal R. K. The mechanism of action of gastrin on the lower esophageal sphincter. Gastroenterology. 1976 May;70(5 PT1):828–831. [PubMed] [Google Scholar]
- Walt R. P., Male P. J., Rawlings J., Hunt R. H., Milton-Thompson G. J., Misiewicz J. J. Comparison of the effects of ranitidine, cimetidine and placebo on the 24 hour intragastric acidity and nocturnal acid secretion in patients with duodenal ulcer. Gut. 1981 Jan;22(1):49–54. doi: 10.1136/gut.22.1.49. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wesdorp I. C. Treatment of reflux oesophagitis. Scand J Gastroenterol Suppl. 1982;79:106–119. [PubMed] [Google Scholar]