

Abstract
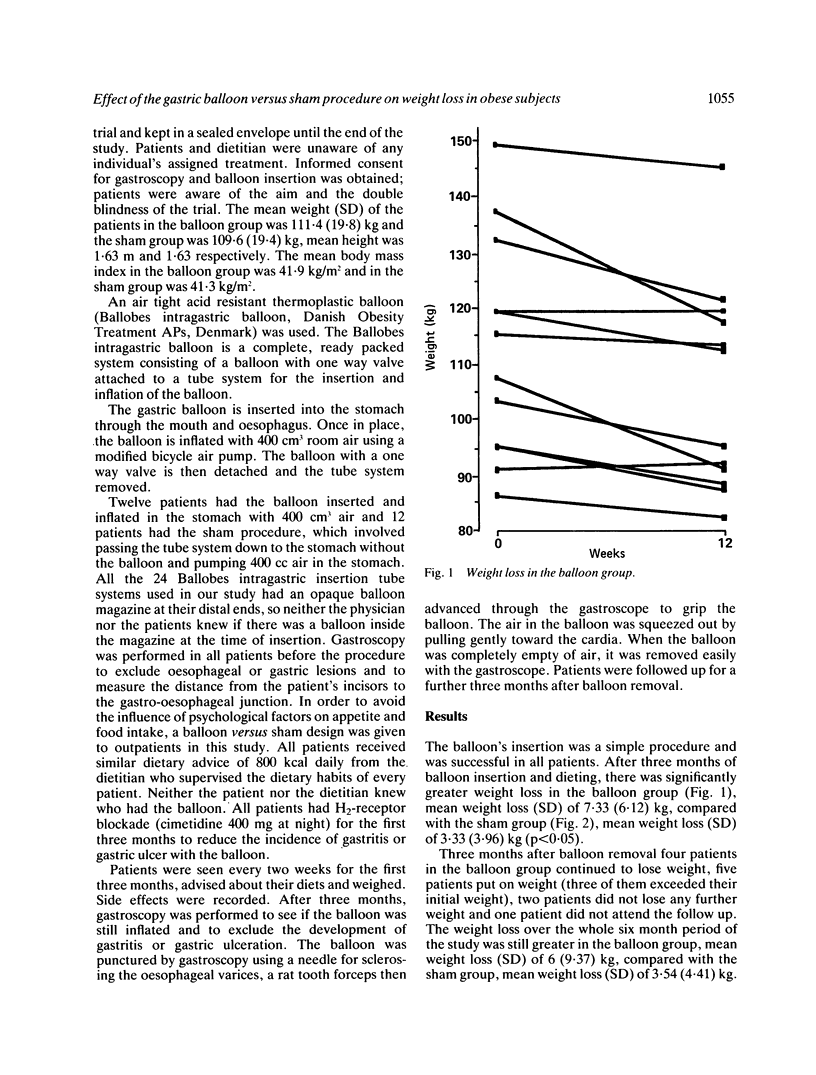
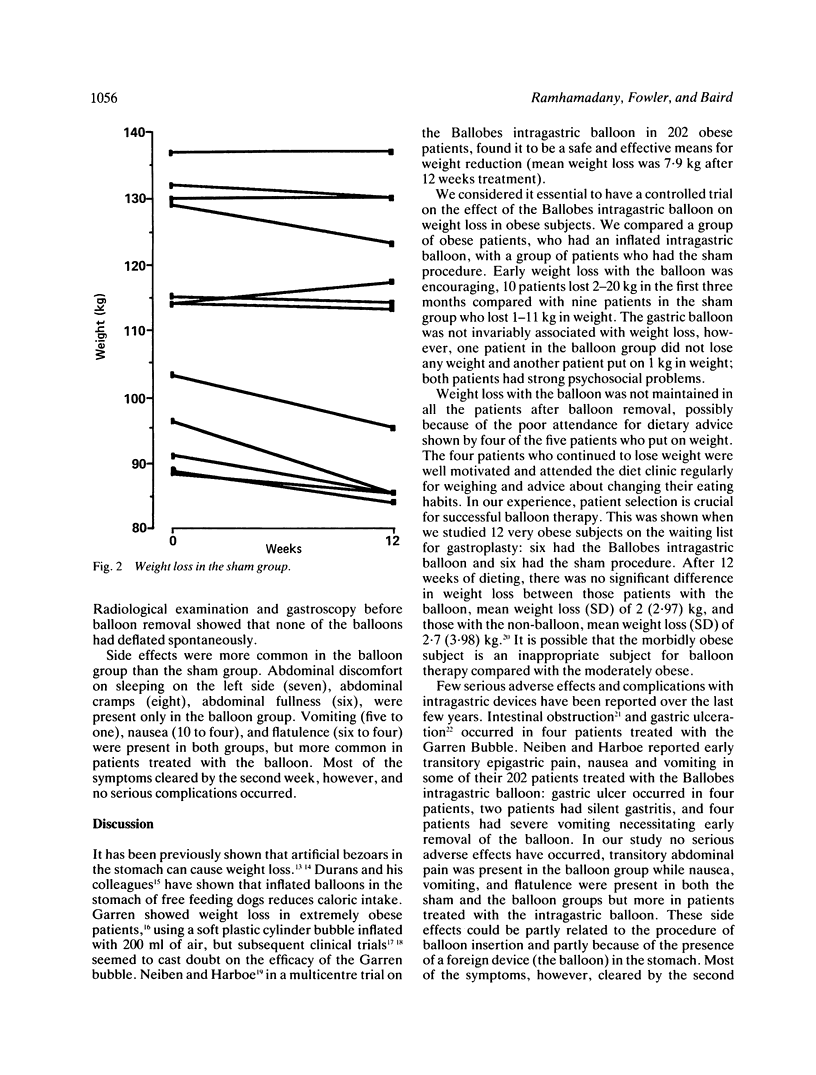
The mechanism by which intragastric balloons induce weight loss is not known, although they may act simply by reducing the amount of food needed to induce satiety. The knowledge that a balloon is present may influence the patients' eating patterns and reduce caloric intake and weight. In order to test whether the balloon or the secondary psychological effect caused weight loss, a double blind balloon versus sham procedure was devised with both groups receiving identical outpatient dietary advice (800 kcal/day). Twenty four obese women with body mass index greater than 30 kg/m2 from an obesity clinic were studied. Twelve had the balloon and 12 the sham procedure. The balloon was removed after three months and the patients were followed for a further three months. There was significantly greater weight loss in the balloon group, mean weight loss (SD) of 7.33 (6.12) kg compared with the sham group, mean weight loss (SD) of 3.33 (3.9) kg (p less than 0.05). Weight loss was not maintained in all patients after balloon removal. Side effects were more common in the balloon group (abdominal pain, nausea, and vomiting) but resolved by the second week. We conclude that the intragastric balloon is a safe and effective method of inducing weight loss in well motivated obese patients.
Full text
PDF
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Bray G. A., Benfield J. R. Intestinal bypass for obesity a summary and perspective. Am J Clin Nutr. 1977 Jan;30(1):121–127. doi: 10.1093/ajcn/30.1.121. [DOI] [PubMed] [Google Scholar]
- Buckwalter J. A., Herbst C. A., Jr Gastric partition for morbid obesity: greater curvature gastroplasty or gastrogastrostomy. World J Surg. 1982 Jul;6(4):403–411. doi: 10.1007/BF01657667. [DOI] [PubMed] [Google Scholar]
- Lal M. M., Dhall J. C. Trichobezoar: a collective analysis of 39 cases from India with a case report. Indian Pediatr. 1975 Apr;12(4):351–353. [PubMed] [Google Scholar]
- McFarland R. J., Grundy A., Gazet J. C., Pilkington T. R. The intragastric balloon: a novel idea proved ineffective. Br J Surg. 1987 Feb;74(2):137–139. doi: 10.1002/bjs.1800740222. [DOI] [PubMed] [Google Scholar]
- Nieben O. G., Harboe H. Intragastric balloon as an artificial bezoar for treatment of obesity. Lancet. 1982 Jan 23;1(8265):198–199. doi: 10.1016/s0140-6736(82)90762-0. [DOI] [PubMed] [Google Scholar]
- Oscai L. B., Holloszy J. O. Effects of weight changes produced by exercise, food restriction, or overeating on body composition. J Clin Invest. 1969 Nov;48(11):2124–2128. doi: 10.1172/JCI106179. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Percival W. L. "The balloon diet": a noninvasive treatment for morbid obesity. Preliminary report of 108 patients. Can J Surg. 1984 Mar;27(2):135–136. [PubMed] [Google Scholar]
- Rodgers S., Burnet R., Goss A., Phillips P., Goldney R., Kimber C., Thomas D., Harding P., Wise P. Jaw wiring in treatment of obesity. Lancet. 1977 Jun 11;1(8024):1221–1222. doi: 10.1016/s0140-6736(77)92434-5. [DOI] [PubMed] [Google Scholar]
- Sullivan A. C., Comai K. Pharmacological treatment of obesity. Int J Obes. 1978;2(2):167–189. [PubMed] [Google Scholar]