

Abstract
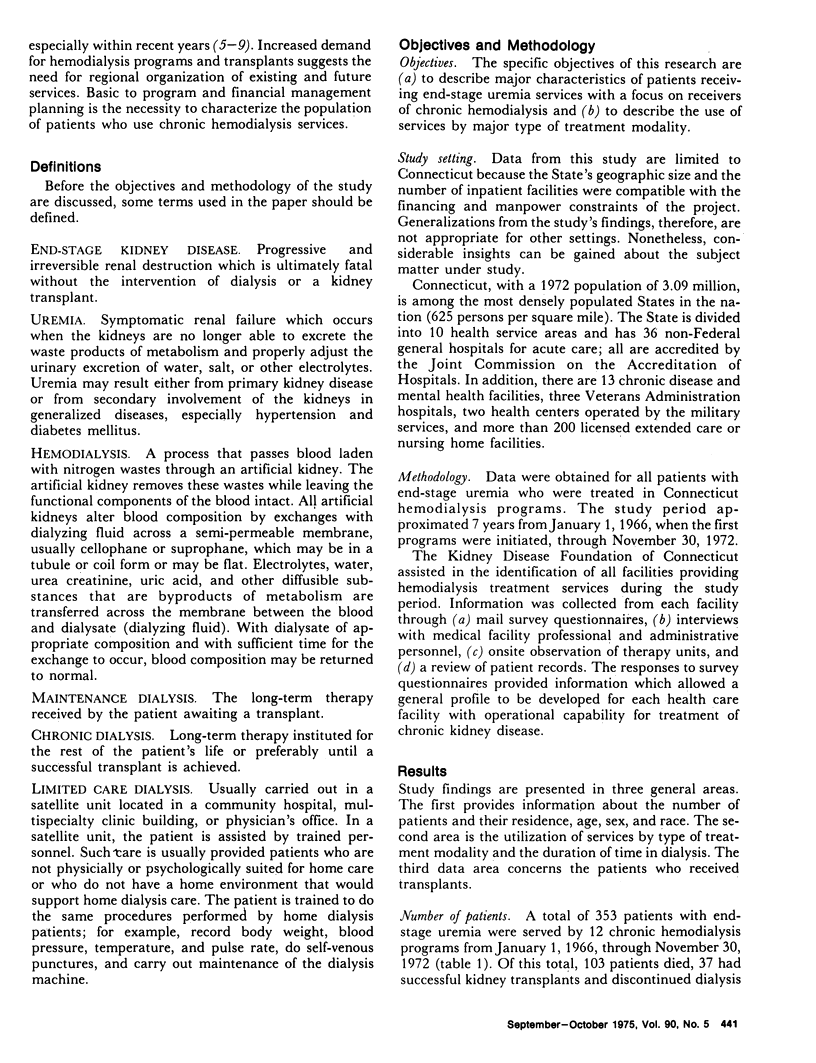
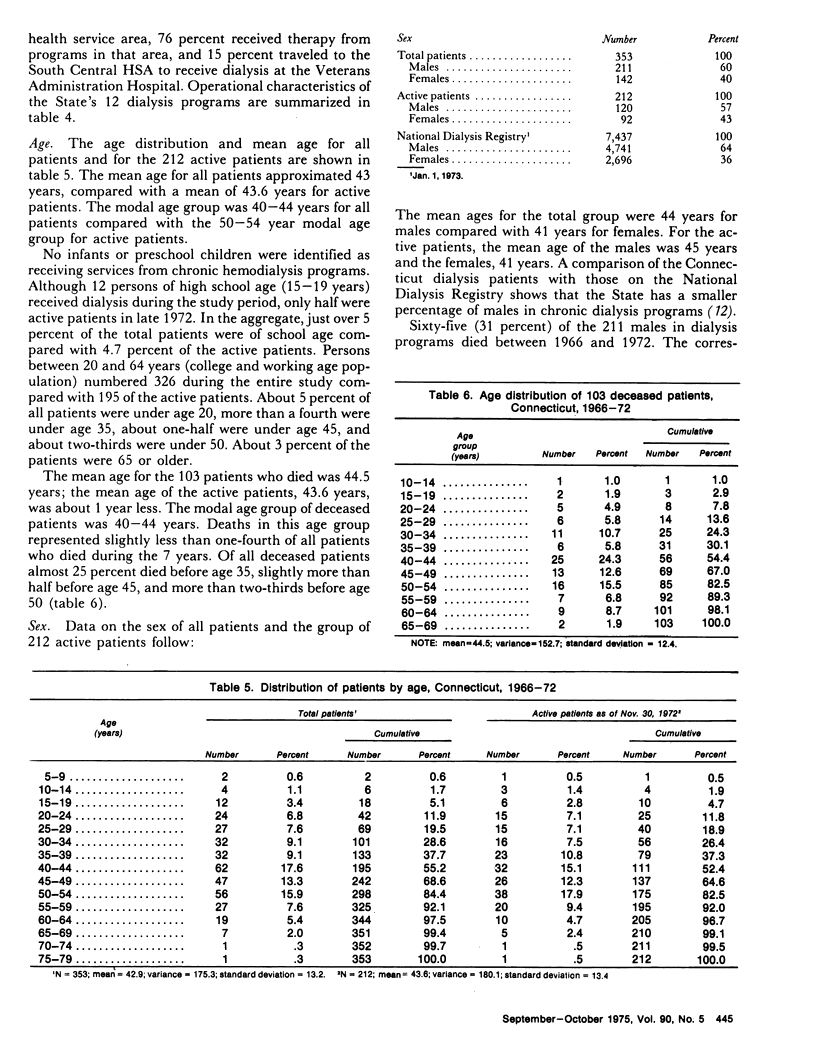
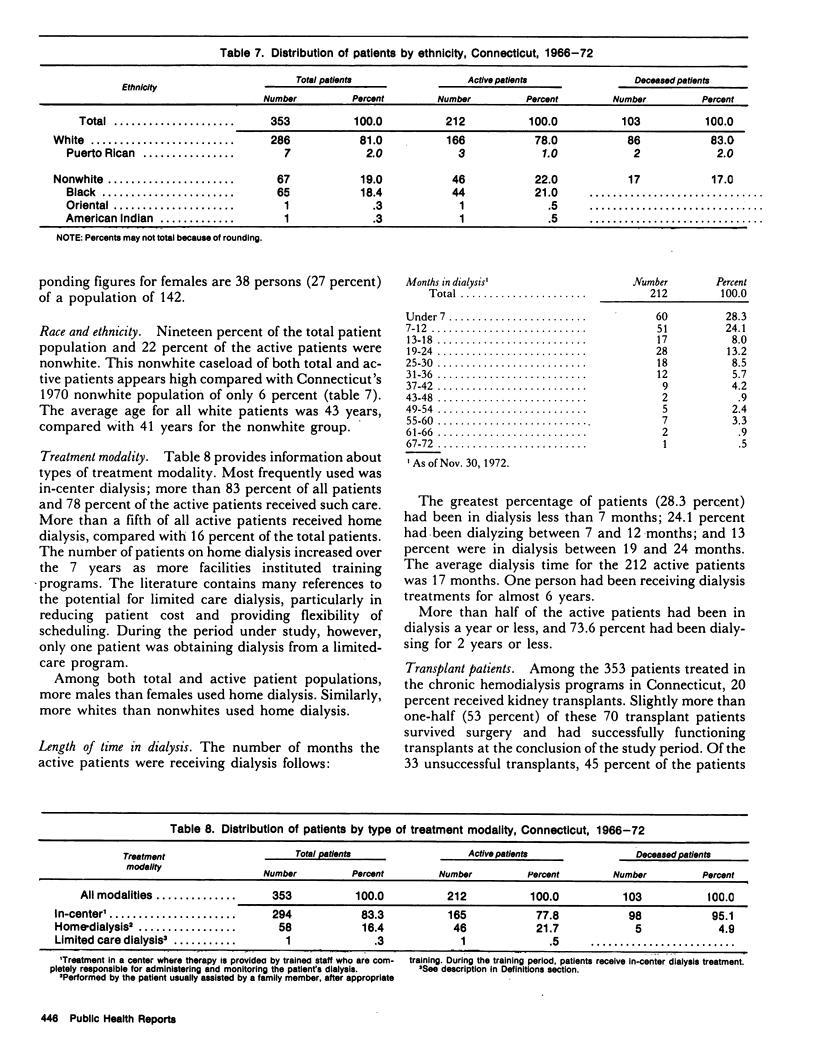
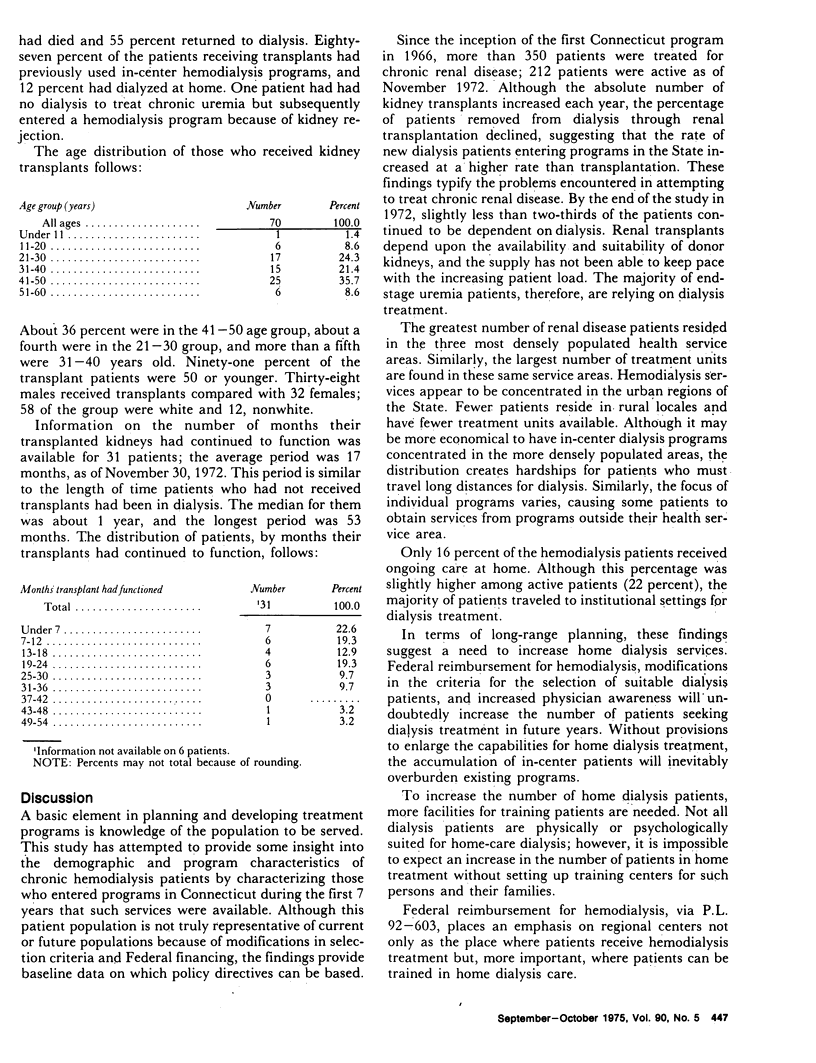
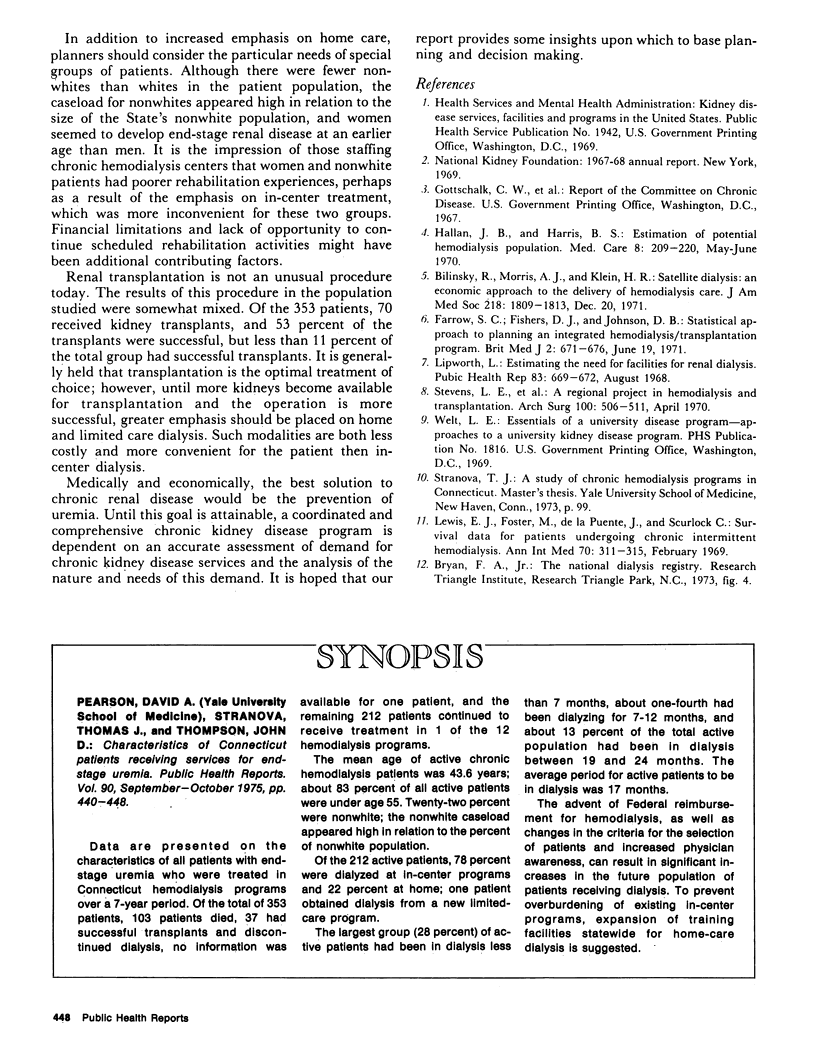
Data are presented on the characteristics of all patients with end-stage uremia who were treated in Connecticut hemodialysis programs over a 7-year period. Of the total of 353 patients, 103 patients died, 37 had successful transplants and discontinued dialysis, no information was available for one patient, and the remaining 212 patients continued to receive treatment in 1 of the 12 hemodialysis programs. The mean age of active chronic hemodialysis patients was 43.6 years; about 83 percent of all active patients were under age 55. Twenty-two percent were nonwhite; the nonwhite caseload appeared high in relation to the percent of nonwhite population. Of the 212 active patients, 78 percent were dialyzed at in-center programs and 22 percent at home; one patient obtained dialysis from a new limited-care program. The largest group (28 percent) of active patients had been in dialysis less than 7 months, about one-fourth had been dialyzing for 7-12 months, and about 13 percent of the total active population had been in dialysis between 19 and 24 months. The average period for active patients to be in dialysis was 17 months. The advent of Federal reimbursement for hemodialysis, as well as changes in the criteria for the selection of patients and increased physician awareness, can result in significant increases in the future population of patients receiving dialysis. To prevent overburdening of existing in center programs, expansion of training facilities statewide for home care dialysis is suggested.
Full text
PDF
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Bilinsky R. T., Morris A. J., Klein H. R. Satellite dialysis. An economic approach to the delivery of hemodialysis care. JAMA. 1971 Dec 20;218(12):1809–1813. doi: 10.1001/jama.218.12.1809. [DOI] [PubMed] [Google Scholar]
- Farrow S. C., Fisher D. J., Johnson D. B. Statistical approach to planning an integrated haemodialysis-transplantation programme. Br Med J. 1971 Jun 19;2(5763):671–676. doi: 10.1136/bmj.2.5763.671. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hallan J. B., Harris B. S., 3rd Estimation of a potential hemodialysis population. Med Care. 1970 May-Jun;8(3):209–220. doi: 10.1097/00005650-197008030-00005. [DOI] [PubMed] [Google Scholar]
- Lewis E. J., Foster D. M., De la Puente J., Scurlock C. Survival data for patients undergoing chronic intermittent hemodialysis. Ann Intern Med. 1969 Feb;70(2):311–315. doi: 10.7326/0003-4819-70-2-311. [DOI] [PubMed] [Google Scholar]
- Lipworth L. Estimating the need for facilities for renal dialysis. Public Health Rep. 1968 Aug;83(8):669–672. [PMC free article] [PubMed] [Google Scholar]
- Stevens L. E., Reemtsma K., Latimer R. G., Maxwell J. G., Weaver D. H., Ward J. S. A regional project in hemodialysis and transplantation. Arch Surg. 1970 Apr;100(4):506–511. doi: 10.1001/archsurg.1970.01340220182030. [DOI] [PubMed] [Google Scholar]