

Abstract
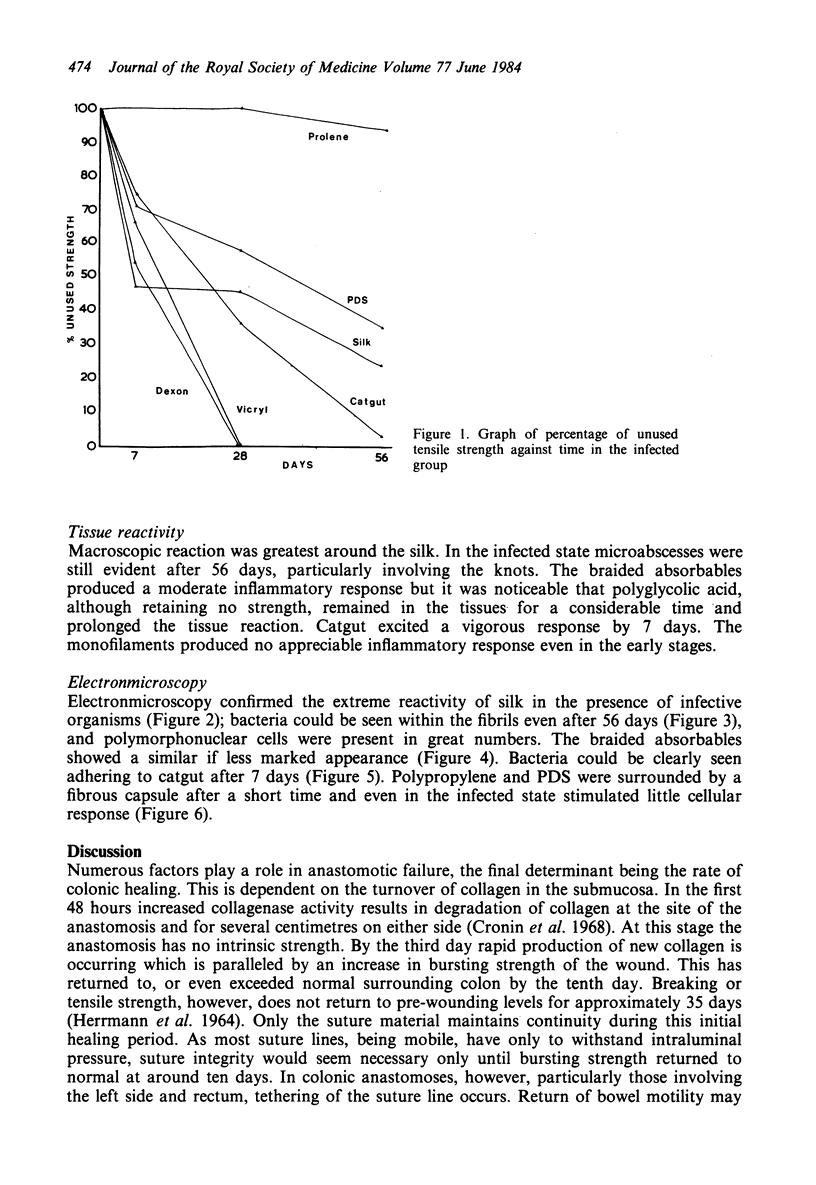
Following injury, normal colon takes approximately 30 days to regain full breaking strength. This healing period can be lengthened by local infection. Colonic anastomoses are likely to be contaminated by intraluminal organisms, and suture material in such a situation is known to potentiate the development of sepsis. Experiments were designed to evaluate six suture materials used in colonic surgery to determine which retained adequate tensile strength and which excited least inflammatory response. The results indicate that absorbable sutures, with the exception of polydioxanone, lose strength too rapidly for use alone. Braided materials, notably silk, produce a prolonged tissue response and harbour bacteria. Monofilament materials are unreactive and appear least likely to delay healing. Polydioxanone, which is monofilament and absorbable, is recommended for use in the colon.
Full text
PDF



Images in this article




Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Cronin K., Jackson D. S., Dunphy J. E. Specific activity of hydroxyproline-tritium in the healing colon. Surg Gynecol Obstet. 1968 May;126(5):1061–1065. [PubMed] [Google Scholar]
- ELEK S. D., CONEN P. E. The virulence of Staphylococcus pyogenes for man; a study of the problems of wound infection. Br J Exp Pathol. 1957 Dec;38(6):573–586. [PMC free article] [PubMed] [Google Scholar]
- Edlich R. F., Tsung M. S., Rogers W., Rogers P., Wangensteen O. H. Studies in management of the contaminated wound. I. Technique of closure of such wounds together with a note on a reproducible experimental model. J Surg Res. 1968 Dec;8(12):585–592. doi: 10.1016/0022-4804(68)90013-9. [DOI] [PubMed] [Google Scholar]
- Fielding L. P., Stewart-Brown S., Blesovsky L., Kearney G. Anastomotic integrity after operations for large-bowel cancer: a multicentre study. Br Med J. 1980 Aug 9;281(6237):411–414. doi: 10.1136/bmj.281.6237.411. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fontaine C. J., Dudley H. A. Assessment of suture materials for intestinal use by an extramucosal implant technique and a quantitative histological evaluation. Br J Surg. 1978 Apr;65(4):288–290. doi: 10.1002/bjs.1800650420. [DOI] [PubMed] [Google Scholar]
- Goligher J. C., Graham N. G., De Dombal F. T. Anastomotic dehiscence after anterior resection of rectum and sigmoid. Br J Surg. 1970 Feb;57(2):109–118. doi: 10.1002/bjs.1800570208. [DOI] [PubMed] [Google Scholar]
- Greatorex G., Whitaker B. L., Dixon R. A. Anastomotic failure in relation to blood transfusion and blood loss. Proc R Soc Med. 1970 Aug;63(8):751–751. [PMC free article] [PubMed] [Google Scholar]
- HERRMANN J. B., WOODWARD S. C., PULASKI E. J. HEALING OF COLONIC ANASTOMOSES IN THE RAT. Surg Gynecol Obstet. 1964 Aug;119:269–275. [PubMed] [Google Scholar]
- Hawley P. R. Causes and prevention of colonic anastomotic breakdown. Dis Colon Rectum. 1973 Jul-Aug;16(4):272–277. doi: 10.1007/BF02587700. [DOI] [PubMed] [Google Scholar]
- JAMES R. C., MACLEOD C. J. Induction of staphylococcal infections in mice with small inocula introduced on sutures. Br J Exp Pathol. 1961 Jun;42:266–277. [PMC free article] [PubMed] [Google Scholar]
- LeVeen H. H., Wapnick S., Falk G., Olivas O., Bhat D., Gaurdre M., Patel M. Effects of prophylactic antibiotics on colonic healing. Am J Surg. 1976 Jan;131(1):47–53. doi: 10.1016/0002-9610(76)90419-0. [DOI] [PubMed] [Google Scholar]
- Morgenstern L., Yamakawa T., Ben-Shoshan M., Lippman H. Anastomotic leakage after low colonic anastomosis. Clinical and experimental aspects. Am J Surg. 1972 Jan;123(1):104–109. doi: 10.1016/0002-9610(72)90317-0. [DOI] [PubMed] [Google Scholar]
- Schrock T. R., Deveney C. W., Dunphy J. E. Factor contributing to leakage of colonic anastomoses. Ann Surg. 1973 May;177(5):513–518. doi: 10.1097/00000658-197305000-00002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Varma S., Ferguson H. L., Breen H., Lumb W. V. Comparison of seven suture materials in infected wounds--an experimental study. J Surg Res. 1974 Sep;17(3):165–170. doi: 10.1016/0022-4804(74)90103-6. [DOI] [PubMed] [Google Scholar]
- Wilkins J. L., Hardcastle J. D., Mann C. V., Kaufman L. Effects of neostigmine and atropine on motor activity of ileum, colon, and rectum of anaesthetized subjects. Br Med J. 1970 Mar 28;1(5699):793–794. doi: 10.1136/bmj.1.5699.793. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Yamakawa T., Patin C. S., Sobel S., Morgenstern L. Healing of colonic anastomoses following resection for experimental "diverticulitis". Arch Surg. 1971 Jul;103(1):17–20. doi: 10.1001/archsurg.1971.01350070043009. [DOI] [PubMed] [Google Scholar]