

Abstract
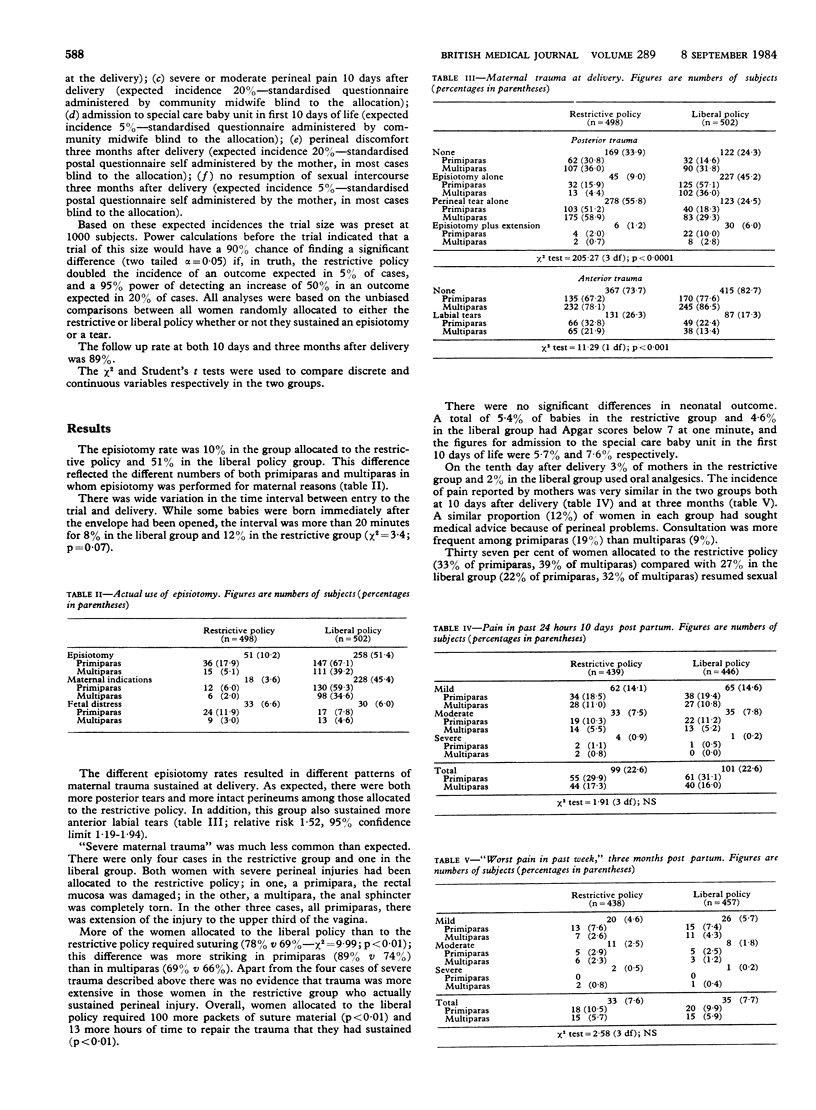
One thousand women were allocated at random to one of two perineal management policies, both intended to minimise trauma during spontaneous vaginal delivery. In one the aim was to restrict episiotomy to fetal indications; in the other the operation was to be used more liberally to prevent perineal tears. The resultant episiotomy rates were 10% and 51% respectively. An intact perineum was more common among those allocated to the restrictive policy. This group experienced more perineal and labial tears, however, and included four of the five cases of severe trauma. There were no significant differences between the two groups either in neonatal state or in maternal pain and urinary symptoms 10 days and three months post partum. Women allocated to the restrictive policy were more likely to have resumed sexual intercourse within a month after delivery. These findings provide little support either for liberal use of episiotomy or for claims that reduced use of the operation decreases postpartum morbidity.
Full text
PDF

Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Russell J. K. Episiotomy. Br Med J (Clin Res Ed) 1982 Jan 23;284(6311):220–220. doi: 10.1136/bmj.284.6311.220. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Stewart P., Hillan E., Calder A. A. A randomised trial to evaluate the use of a birth chair for delivery. Lancet. 1983 Jun 11;1(8337):1296–1298. doi: 10.1016/s0140-6736(83)92412-1. [DOI] [PubMed] [Google Scholar]
- Thacker S. B., Banta H. D. Benefits and risks of episiotomy: an interpretative review of the English language literature, 1860-1980. Obstet Gynecol Surv. 1983 Jun;38(6):322–338. [PubMed] [Google Scholar]