

Abstract
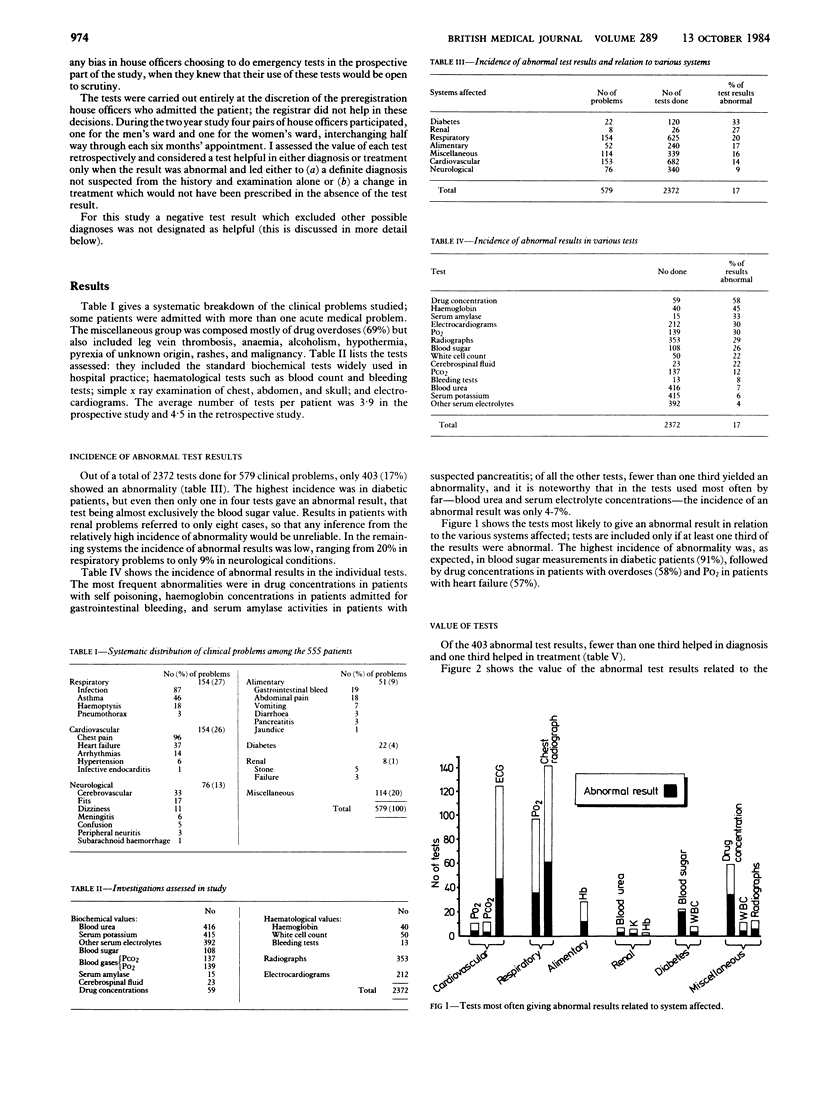
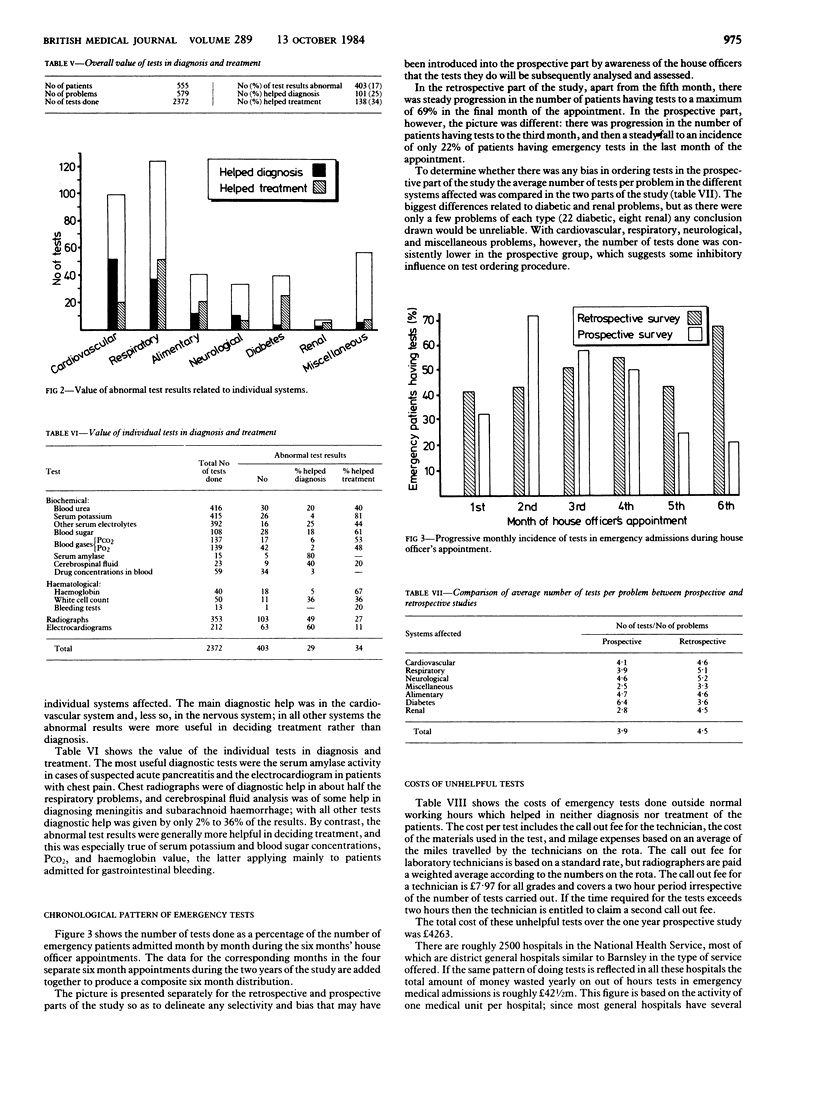
A two year combined retrospective and prospective study of 555 acute medical admissions to a district general hospital was carried out to assess the value of emergency biochemical, haematological, radiological, and electrocardiographic tests in diagnosis and treatment. For the study the tests were considered helpful only if they disclosed an abnormality and resulted in a definite diagnosis or change of treatment which would not have been possible from the history and examination alone. A total of 2372 emergency tests were carried out in the 555 patients who presented with 579 acute medical problems. Only 403 (17%) of the test results were abnormal and, of these, only one third helped in treatment and less than one third helped in diagnosis. The most useful diagnostic tests were serum amylase activity in abdominal pain, the electrocardiogram in chest pain, the chest radiograph in respiratory problems, and cerebrospinal fluid analysis in suspected meningitis or subarachnoid haemorrhage. The most useful tests in treatment were blood sugar value in diabetes, PCO2 in obstructive airways disease, and haemoglobin concentration in gastrointestinal haemorrhage. Of the tests requested by far the most often--blood urea and serum electrolyte concentrations--only 7% gave abnormal results and were rarely of any help in either diagnosis or treatment. Analysis of the reasons for the uncritical use of emergency tests by house officers suggested that better undergraduate training, regular audit by senior members of medical units, abolition of routine investigational procedures, and more selective laboratory reports would help to build up the house officer's confidence in his own skills of history taking and physical examination without recourse to indiscriminate use of laboratory and other investigations.
Full text
PDF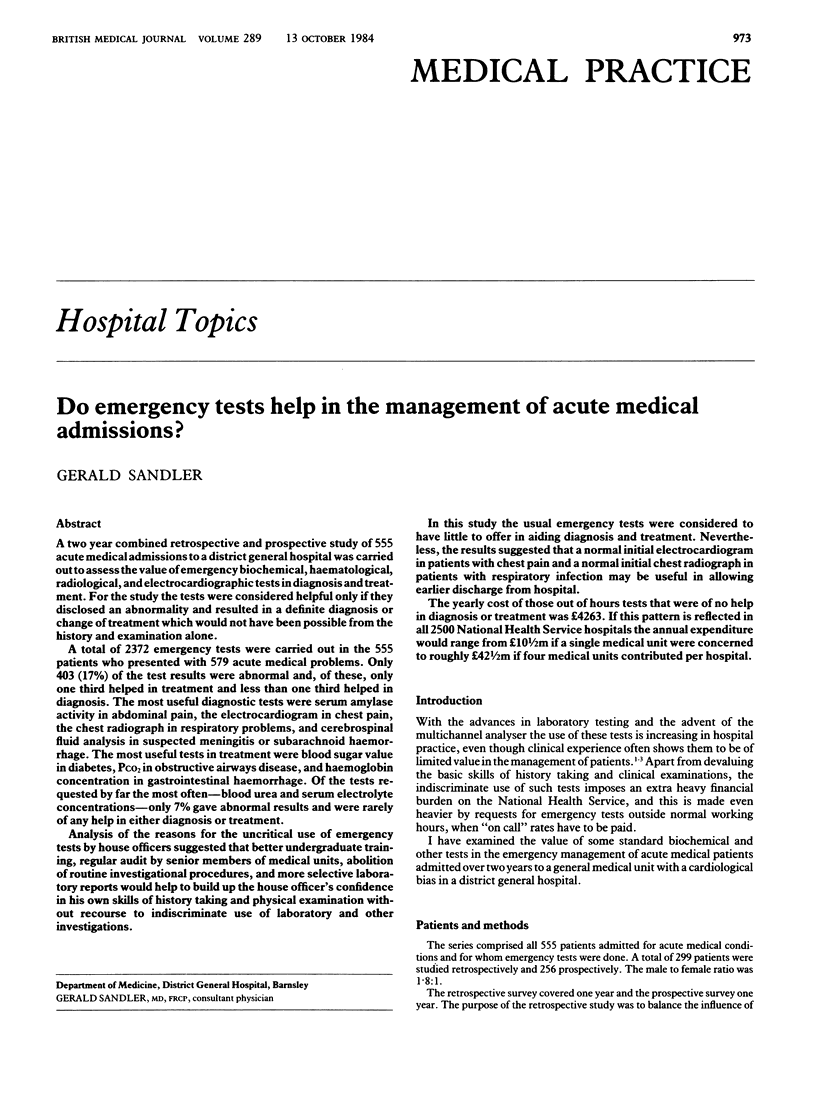

Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Brod J. The rational basis of diagnosis in internal medicine. J R Coll Physicians Lond. 1977 Jul;11(4):323–334. [PMC free article] [PubMed] [Google Scholar]
- Daniels M., Schroeder S. A. Variation among physicians in use of laboratory tests. II. Relation to clinical productivity and outcomes of care. Med Care. 1977 Jun;15(6):482–487. doi: 10.1097/00005650-197706000-00004. [DOI] [PubMed] [Google Scholar]
- Epstein F., Epstein N. Surgical treatment of spinal cord astrocytomas of childhood. A series of 19 patients. J Neurosurg. 1982 Nov;57(5):685–689. doi: 10.3171/jns.1982.57.5.0685. [DOI] [PubMed] [Google Scholar]
- Hampton J. R., Harrison M. J., Mitchell J. R., Prichard J. S., Seymour C. Relative contributions of history-taking, physical examination, and laboratory investigation to diagnosis and management of medical outpatients. Br Med J. 1975 May 31;2(5969):486–489. doi: 10.1136/bmj.2.5969.486. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wertman B. G., Sostrin S. V., Pavlova Z., Lundberg G. D. Why do physicians order laboratory tests? A study of laboratory test request and use patterns. JAMA. 1980 May 23;243(20):2080–2082. [PubMed] [Google Scholar]