

Abstract
Objectives. This study examined long-term response to an individual preventive intervention for high-risk college drinkers relative to the natural history of college drinking.
Methods. A single-session, individualized preventive intervention was evaluated within a randomized controlled trial with college freshmen who reported drinking heavily while in high school. An additional group randomly selected from the entire screening pool provided a normative comparison. Participant self-report was assessed annually for 4 years.
Results. High-risk controls showed secular trends for reduced drinking quantity and negative consequences without changes in drinking frequency. Those receiving the brief preventive intervention reported significant additional reductions, particularly with respect to negative consequences. Categorical individual change analyses show that remission is normative, and they suggest that participants receiving the brief intervention are more likely to improve and less likely to worsen regarding negative drinking consequences.
Conclusions. Brief individual preventive interventions for high-risk college drinkers can achieve long-term benefits even in the context of maturational trends.
Lifetime consumption of alcohol typically reaches its highest levels during an individual's late teens and early 20s.1 Numerous studies document a range of negative consequences of high levels of alcohol consumption, including violence, date rape, accidents, academic problems, and family conflict.1,2 The college campus is one setting where the pattern of youthful heavy drinking is felt acutely. College students, on average, drink more than their noncollege peers of the same age3 and routinely report negative consequences from both their own and others' drinking.4 While heavy drinking in college is associated with personality factors such as impulsivity,5 noncomformity,6 and depression,5,7,8 contextual factors such as distance from parents, close association with peers, dormitory residence, association with fraternities and sororities, large-group social events, and athletics appear to support and exacerbate heavy drinking as well.9–13
Heavy drinking in college should not be confused with dependent drinking in later life, however. Several studies note significant reductions in heavy drinking in the 20s.14–16 At the individual level, Schulenberg and colleagues17 followed the drinking patterns of high school seniors for at least 6 years and noted that a subset of individuals (17%) reported more than isolated patterns of heavy drinking over time. Thus, college administration and health officials, who are under increasing pressure to provide both preventive and treatment services as a public health service for college students, are faced with a multifaceted social problem that is common, risky, and limited in time for most but chronic for some.
Unfortunately, few interventions have a documented positive impact in changing college drinking behavior. In particular, commonly offered educational programs have little impact.18 We recently reported on one model of indicated prevention, which involves personalized individual feedback and brief motivational interventions for high-risk students during a single brief, nonconfrontational counseling session.19–21 Students who received this preventive intervention reported significantly greater reductions in alcohol-related problems at the 2-year follow-up compared with a randomly assigned control group.21,22
In the current analysis, we examine the natural history of drinking patterns and related problems over 4 years, within both high-risk and normative samples. The preventive intervention is evaluated over this extended period of time. Finally, using individual classification of reliable change,22 we describe developmental trajectories of drinking among college students who drank heavily in high school and describe rates of clinically significant change.
METHODS
Participants and Recruitment
All students younger than 19 years who had committed themselves to attending the University of Washington in the fall of 1990 (n = 4000) were mailed a questionnaire during the spring before matriculation. For completing the questionnaire, students were paid $5 and entered into a drawing for a prize. The questionnaire included items about quantity and frequency of alcohol consumed during a typical week and peak alcohol consumption in the past 3 months.21 The questionnaire also included the Rutgers Alcohol Problem Inventory23 to assess drinking-related consequences during the previous 3 years. A total of 2041 students (51%) provided complete questionnaires and indicated a willingness to participate in a future study.
From the completed questionnaires, 508 individuals were identified as being at “high risk” by the following criteria: drinking at least once a month and consuming 5 to 6 drinks on at least 1 occasion in the last month, or experiencing at least 3 negative consequences from drinking (Rutgers Alcohol Problem Inventory items) on 3 to 5 different occasions in the previous 3 years. An additional normative comparison sample was selected randomly from the entire pool of responders (n = 151), including 33 persons who met high-risk criteria, to track the natural history of changes in drinking behavior within the cohort over time.
Potential participants were invited by letter and by phone. Participants were paid $25 for entering the study, completing the baseline questionnaire and interview, and providing 2 collateral contacts who could confirm the participant's rates of alcohol consumption. Of those contacted, 348 (68%) who were identified as being at high risk agreed to participate and were randomized into either the intervention or no-intervention control groups; 113 (75%) of those randomly selected for the natural history comparison agreed to participate (28 of the 113 also met high-risk criteria). At baseline assessment in the autumn of their freshman year, high-risk students reported, on average, drinking more than 10 drinks per week during fewer than 2 drinking occasions, reaching a typical estimated peak blood alcohol level of 0.12%. Normative comparison students reported drinking about 5½ drinks per week during 1 drinking occasion, reaching a typical estimated peak blood alcohol level of 0.08%. The high-risk sample was 55% female and 84% White. The normative comparison sample was 54% female and 78% White.
Confidence in the representativeness of the sample is potentially limited by the 50% response rate to the initial mailing. However, drinking rates within the normative comparison sample are quite consistent with averages noted in national databases (e.g., Monitoring the Future24). The level of drinking among high-risk participants is more extreme than in national averages; 79.5% reported drinking at least 5 to 6 drinks on 1 occasion in the past month at baseline, compared with about 40% within the Monitoring the Future Study.
Measures
All participants used 6-point scales to rate the quantity, frequency, and peak occasions of their drinking (QFP21) and completed the Daily Drinking Questionnaire,25 which asks about the actual number of drinks for each day of a typical drinking week, yielding drinking days per average week and average drinks per drinking day.
To assess negative drinking consequences, we asked participants to complete the Rutgers Alcohol Problem Inventory,23 a 23-item instrument designed to assess problem drinking among adolescents, and the Alcohol Dependency Scale,26 a well-established assessment for severity of drinking problems. At baseline only, trained interviewers administered the alcohol dependence questions from the Diagnostic Interview Schedule,27 questions on drinking patterns and consequences from the Brief Drinker Profile,28 and interview sections to assess family history of alcoholism and personal history of conduct problems. Other questionnaires assessed alcohol expectancies, psychiatric symptomatology, stress, perceived drinking norms, and sexual behavior.21 Results from these assessments are not included in this report.
Baseline and Follow-Up Procedure
At baseline, all participants completed the interview and questionnaire packet described above. Follow-up assessments, which repeated the questionnaire measures included at baseline, were completed by mail annually (with the exception of an initial 6-month follow-up described previously21). Assessments were completed, whenever possible, within the middle of the autumn academic term to minimize the impact of well-known seasonal variations (football season, spring break, final examinations, etc.). Participants were paid $20 for each annual assessment. All collateral reporters were phoned after each participant assessment, and collateral interviews were successfully completed for approximately 50% of subjects at each assessment point. These data are not analyzed for this report; previous analyses at the 2-year follow-up demonstrated reasonable reliability with subjects' self-reports, with no evidence of systematic over- or underreporting of drinking.21 Collecting collateral data is thought to enhance the validity of participants' self-report in conditions of confidentiality.29
Preventive Intervention
Freshman participants who had been randomly assigned to the intervention group were contacted during the winter term and scheduled for an individualized feedback session. Participants were instructed to self-monitor drinking patterns 2 weeks before the scheduled session. Eight interviewers using a written manual20 provided personal feedback concerning the consumption patterns as reported on diary cards and at baseline assessment. Rates of drinking were compared with norms for same-age peers. Individualized feedback also included information about perceived risks and benefits of drinking, mythology concerning drinking behavior, the biphasic effects of alcohol, and placebo and tolerance effects. The style of the intervention was consistent with motivational interviewing30: client-centered in tone, but nevertheless seeking to highlight and explore discrepancies between current behavior and plans, goals, and aspirations. Each participant was also given a 1-page list of tips for reducing risks associated with drinking.20
During the winter term of their second year in college, participants randomized into the prevention condition were mailed feedback results comparing their drinking and its consequences with the norms of their college peers. The summary sheets contained bar graph results from 3 assessments (baseline, spring of the freshman year, and fall quarter of the sophomore year) and concluded with a paragraph that personalized the feedback for each participant. After the mailing, we also phoned prevention group participants in the highest-risk categories (n = 56) to express concern about risk and offer additional feedback sessions. Thirty-four motivational interviews were conducted in the second year, most over the phone (n = 26).
Missing Data
Two methods of processing missing data were compared: listwise deletion and multiple imputation. Participants with missing data at the 4-year follow-up were eliminated from data analyses. Missing data occurring at the 1-, 2-, or 3-year assessments were replaced by a multiple imputation method using maximum likelihood estimation.31,32 Sensitivity analyses indicated no differences in parameter estimates between imputation of missing values and list-wise deletion of cases with missing data; therefore, data with imputed values were used for all subsequent analyses to preserve sample degrees of freedom.
Data Preparation
All outcome measures were standardized with the normative comparison sample baseline mean and standard deviation, yielding relative scores from a normative baseline whose mean equals 0 and whose standard deviation equals 1. We also converted the standardized outcome measures in each drinking domain to 3 unit-weighted factor scores by computing the mean of the standardized relevant measured indicators33: drinking frequency (a 6-point Likert scale of drinking frequency and Daily Drinking Questionnaire estimates of drinking days per week), drinking quantity (2 6-point Likert scales measuring average and peak drinking quantity, respectively, and the Daily Drinking Questionnaire measure of average drinks per drinking day), and negative consequences (Rutgers Alcohol Problem Inventory and Alcohol Dependency Scale). Although the metric of the original variables is not retained, these unit-weighted factors enhance the reliability and validity of the dependent variables and avoid conclusions based on single variables.34
RESULTS
Success of Randomization
No significant baseline differences were observed between prevention and control conditions for alcohol consumption, related consequences, or demographic and individual difference factors.21
Longitudinal Attrition
At the 4-year follow-up, 363 of the 433 unique participants (84%) from the 2 high-risk groups and the normative comparison group completed assessments. Complete data sets at baseline and all 4 follow-up periods were provided by 328 participants (76%), and 346 participants (80%) provided data at 4 of 5 time points, including year 4. Consistent with university norms, 53% of the sample reported having graduated at the 4-year follow-up.
Attrition rates at the 4-year assessment did not differ significantly between high-risk and normative comparison groups, or between randomized high-risk group conditions (prevention vs control). Attrition was not significantly related to participant's sex or to baseline quantity, frequency, or consequences of drinking.
Changes in Drinking and Negative Consequences by Prevention Condition
Three distinct mixed model analyses35 provided hypothesis tests with restricted maximum likelihood parameter estimates for the effects of group (prevention and control) and time (baseline and 1-, 2-, 3-, and 4-year follow-up) on the 3 major outcome factor scores: frequency, quantity, and negative consequences. The mixed models included specifications for a priori contrasts for adjacent time points (baseline vs 1-year follow-up, 1-year vs 2-year follow-up, etc.), repeated-measures effects for time, time-by-treatment interactions, and random-effects estimates for subjects. A priori contrasts of time-by-treatment effects allow evaluation of increasing or decreasing differences between experimental groups at the 3- or 4-year assessments.
Standardized mean differences from normative baselines among high-risk participants for drinking frequency, drinking quantity, and negative drinking consequences over the 4-year follow-up are listed in Table 1 ▶. Figure 1 ▶ displays drinking rates and consequences for high-risk participants and normative comparison samples. Significant main effects over time were noted in all 3 analyses. Over 4 years, the magnitude of change was greatest for measures of negative drinking consequences (F4321 = 45.65, P < .001), compared with those of drinking quantity (F4321 = 28.22, P < .001) and drinking frequency (F4321 = 7.58, P < .001), which demonstrated the smallest effect.
TABLE 1—
Mean Standardized Factor Scores (SD) and Differences (SEM) Between High-Risk Prevention Group and High-Risk Control Group Over 4 Years: Preventive Intervention for College Drinkers
| Follow-Up | |||||||
| Drinking Factor | Baseline | 1 Year | 2 Year | 3 Year | 4 Year | Time Test F4321 | Group × Time Test F4321 |
| Frequency | 7.58*** | 1.26 | |||||
| Control | 0.74 (0.88) | 0.80 (0.92) | 0.62 (0.84) | 0.88 (1.02) | 0.71 (0.99) | ||
| Prevention | 0.78 (0.88) | 0.60 (0.89) | 0.52 (0.88) | 0.75 (0.93) | 0.64 (1.04) | ||
| Difference | –0.04 (0.10) | 0.20 (0.10) | 0.09 (0.10) | 0.13 (0.11) | 0.06 (0.12) | ||
| Quantity | 28.22*** | 4.33*** | |||||
| Control | 0.73 (0.90) | 0.76 (0.82) | 0.59 (0.85) | 0.51 (0.81) | 0.38 (0.77) | ||
| Prevention | 0.91 (0.92) | 0.60 (0.89) | 0.46 (0.93) | 0.48 (0.84) | 0.27 (0.78) | ||
| Difference | –0.17 (0.10) | 0.15 (0.10) | 0.12 (0.10) | 0.03 (0.09) | 0.10 (0.09) | ||
| Negative consequences | 45.65*** | 2.38* | |||||
| Control | 1.46 (1.27) | 1.23 (1.37) | 0.95 (1.22) | 0.80 (1.26) | 0.72 (1.25) | ||
| Prevention | 1.39 (1.26) | 0.79 (1.24) | 0.53 (1.06) | 0.52 (1.10) | 0.40 (1.06) | ||
| Difference | 0.06 (0.14) | 0.44 (0.15)** | 0.41 (0.13)** | 0.28 (0.13)* | 0.31 (0.13)** | ||
Note. Factor scores reflect elevations in SD units relative to baseline mean for the normative comparison group. All mean values are significantly greater than 0.0. Difference score = control score minus prevention score, and difference deviations are standard errors as computed by SAS PROC MIXED.35 Rounding of factor scores creates slight discrepancies in difference scores. Statistical tests of difference scores represent bivariate tests where H0: Tcontrol = Tprevention.
*P < .05; **P < .01; ***P < .001 for all tests.
FIGURE 1—
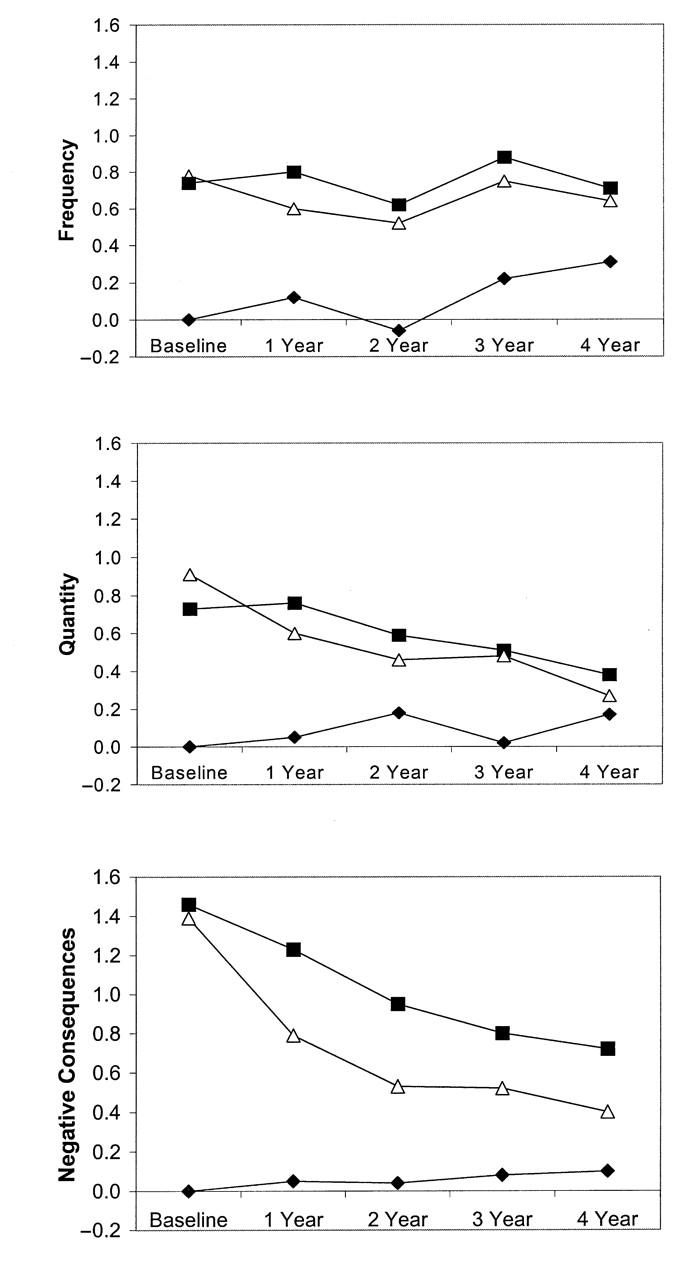
Standardized factor scores for 3 dimensions of drinking behavior over 4 years, shown separately for the high-risk control group (▪), the high-risk prevention group (▵), and the normative comparison group (♦).
Significant prevention group–by–time interactions over 4 years were observed with respect to negative drinking consequences (F4321 = 2.38, P < .05) and for drinking quantity (F4321 = 4.33, P < .001), but not with respect to drinking frequency. Thus, from a multivariate perspective, drinking problems declined significantly over time, and the preventive intervention produced significant differences in alcohol use and related problems over 4 years. Group-by-time effects (differential change) are shown in Table 1 ▶ to result in significant group differences in negative consequences at all follow-up assessments.
A priori contrasts of between-group differences in change scores (t310 complete case analysis, 2-tailed test) represent group-by-time interactions for each interval and thus reveal when treatment effects occur. Differences in the magnitude of change between the high-risk prevention and high-risk control groups from baseline to 1-year follow-up were evident for frequency (P = .03), quantity (P = .0002), and negative consequences (P = .0095). All other adjacent time change contrasts between groups were nonsignificant (P > .05). Thus, the prevention program appears to have its primary effect between the baseline and 1-year assessments. Differences noted at the 3- and 4-year assessments can be interpreted as a continuation of effects noted earlier in the follow-up period.
Trajectories of the normative comparison subjects over time are also evident in Figure 1 ▶. For normative participants (separate analysis on all normative control group subjects), drinking frequency was significantly increased relative to baseline at the 3-year follow-up (t112 = 2.18, P < .05) and 4-year follow-up (t112 = 2.51, P < .05). Drinking quantity showed minor variation over time, with the 2-year assessment being significantly above baseline (t112 = 2.18, P < .05). Mean negative consequences of drinking remained quite stable through the college years.
We reanalyzed the drinking patterns described above to evaluate the possible moderating effects of the participant's sex. Sex did not significantly moderate the prevention effects previously noted for drinking quantity or negative drinking consequences. A 3-way interaction for drinking frequency (F9320 = 2.22, P < .05) proved difficult to interpret. Examination of means suggested that there was greater variability over time among control group males and that, relative to the control condition, the preventive intervention may have reduced drinking frequency among women but not among men.
Analysis of Individual Change
Average changes in drinking rates and problems may mask considerable variability in individual responses, and thus they do not provide a measure of individual risk status and do not indicate how many cases of problem alcohol use might be prevented as a result of this prevention program. To describe outcomes and natural history in terms reflective of individual risk status for college students, we computed risk cutpoints and measures of individual change by using an algorithm reported elsewhere.22 We chose to examine the Alcohol Dependency Scale for the current analysis because it best reflects the negative consequences of drinking (where the prevention program had the greatest impact) and does not contain college-specific items (e.g., slept late for a class) that are less relevant to those who have quit school or graduated by the 4-year follow-up. The risk cutpoint of 5 for the Alcohol Dependency Scale was established empirically to reflect the point at which a subject is equally likely to be a member of the high-risk population or of the normative population containing no high-risk participants (a “functional” comparison22). As described in an earlier report,22 we used an empirical-percentiles approach to determine cutpoints and confirmed the stability of estimates through bootstrapping.36 A reliable change index37 was defined as a difference from baseline scores that meets or exceeds 2 standard errors of the estimate of difference scores.
Participants were then categorized on the basis of their baseline scores and 4-year follow-up scores. Owing to the multidimensional definition of “high risk,” not all high-risk participants were above the risk cutpoint for the Alcohol Dependency Scale at baseline. Similarly, the normative comparison group included some individuals with scores above risk cutpoints at baseline. Participants were classified as “resolved” if their score began above the risk cutpoint, changed reliably (more than the reliable change index), and ended below the cutpoint. Participants were classified as “reliably improved” if their score changed reliably in a direction of fewer dependence symptoms but did not cross the cutpoint. Participants were classified as “reliably worse” if their score moved reliably in the direction of more dependence symptoms but did not cross from below to above the risk cutpoint. “New cases” represents those individuals who became reliably worse over time and crossed from below to above the risk cutpoint. If change did not exceed the reliable change index, participants were classified as “no change.”
Table 2 ▶ presents change categories, based on the Alcohol Dependency Scale, from baseline to 4-year follow-up for all participants. Within the normative comparison group, which represents the population of students at this university and thus includes some high-risk participants, 22.9% of students with scores below the risk cutpoints at baseline became new cases; the modal trajectory was no change (55.7%). Among the 35 normative comparison students whose scores were above a risk cutpoint at baseline, 8.6% reliably improved and 31.4% were resolved at the 4-year follow-up. Trends for high-risk participants as well as preventive intervention effects can also be observed in Table 2 ▶. For example, among high-risk participants with Alcohol Dependency Scale scores above the risk cutpoint at baseline, 32.8% of those in the control condition were resolved at the 4-year follow-up, indicating that roughly a third of those who drink heavily in high school resolve drinking risk over the course of 4 years. This rate improved to 42.6% among those in the prevention condition. Surprisingly, among high-risk participants with Alcohol Dependency Scale scores below the risk cutpoint at baseline, 18.5% of the control group were reliably worse or were new cases 4 years later, compared with 10% of the prevention group. More generalized comparisons also follow from Table 2 ▶. Among high-risk participants, 67% of the prevention group had good outcomes over 4 years (resolved, reliably improved, or no change from a baseline score below the risk cutpoint), compared with 55% of controls.
TABLE 2—
Individual Change (%), Based on the Alcohol Dependency Scale (ADS), for High-Risk Participants and Normative Comparison Participants From Baseline to 4-Year Assessment: Preventive Intervention for College Drinkers
| ADS Score | New Case | Reliably Worse | No Change | Reliably Improved | Resolved |
| Above cutpoint at baseline | |||||
| Normative comparison (n = 35) | … | 8.6 | 51.4 | 8.6 | 31.4 |
| High-risk control (n = 116) | … | 9.5 | 40.5 | 17.2 | 32.8 |
| High-risk prevention (n = 115) | … | 2.6 | 36.5 | 18.3 | 42.6 |
| Below cutpoint at baseline | |||||
| Normative comparison (n = 61) | 22.9 | 9.8 | 55.7 | 11.5 | … |
| High-risk control (n = 27) | 14.8 | 3.7 | 74.1 | 7.4 | … |
| High-risk prevention (n = 30) | 10.0 | 0.0 | 70.0 | 20.0 | … |
DISCUSSION
Central findings suggest that much heavy drinking among college students is transitory, despite some students who report a pattern of continued or worsening consequences over time. Changes in drinking are reflected in specific dimensions of drinking behavior. Compared with a high-risk control sample, in this randomized trial, participants receiving a brief individual preventive intervention had significantly greater reductions in negative consequences that persisted over a 4-year period. Individual change analyses suggest that the dependence symptoms of those receiving the brief intervention are more likely to decrease and less likely to increase.
To understand the impact of the preventive intervention in a broader context, we report the natural history of different dimensions of drinking through the participants' 4 years of college. The frequency of drinking did not change dramatically over 4 years for either high-risk or normative samples. Normative comparison participants, representing the general student body, reported slight increases in drinking frequency over time, particularly at the 3-year follow-up, when many in the sample had reached 21 years of age.38 Drinking frequency among high-risk students declined only minimally over the 4-year period.
Mean drinking quantity and negative consequences increased only marginally within our normative comparison group, suggesting that students in general do not commonly or routinely develop drinking problems during the college years.3,24 However, drinking quantity and associated problems declined steadily over time for high-risk students who entered college with a history of heavy drinking. Recruitment of high-risk students was based on drinking during high school, and thus both developmental and statistical trends probably move toward less extreme behavior (but these same individuals reported mean increases in drinking upon entry into college39). Four years after matriculation, our high-risk control students continued to drink more frequently than the normative comparison students, but their problem scores had markedly decreased and, although still above those of the comparison group, were much less elevated (standardized difference about 0.62) than they were at baseline (standardized difference about 1.40). This pattern of data is consistent with other longitudinal studies showing that adolescents with problem behaviors (including heavy drinking) remain less conventional than others as they age into adulthood, but do not have worse psychosocial adjustment.16
Prevention effects were observed for only some dimensions of drinking behavior. The dimension of greatest interest, negative consequences of drinking, shows the greatest effects. This is important not only because negative consequences measure the degree to which individuals may be harmed as a result of drinking, but also because the preventive intervention targeted individual choices and reduction of risk, rather than drinking rates per se. Our findings are consistent with the goals of harm reduction interventions,40 approaches that focus on minimizing the harmful effects of high-risk drinking. The duration of our prevention effects is also noteworthy. Modest differential changes in drinking quantity and frequency, described in our earlier report of 2-year outcomes,21 do not appear to persist for longer periods of time, yet we found significantly reduced negative consequences 3½ years after the preventive intervention. We are unaware of other studies (much less randomized trials) of prevention efforts among college students that demonstrate such long-lasting effects.
Our analyses of individual change suggest that, regardless of baseline risk status, about 1 in 3 college students, as represented by the normative comparison participants, reliably worsen during the college years. Another third do not change, and a third reliably improve. Among high-risk samples, many more students reliably improve than worsen, and those with scores beginning below risk cutpoints most often report no change in drinking status. Group differences in rates of reliable worsening and improvement among high-risk participants suggest that feedback and advice may function by accelerating a normative developmental process of reducing drinking, as well as by slowing a less typical developmental process that may otherwise lead to an escalation of drinking for some individuals during college years.
The results described in this report should, of course, be interpreted with attention to the inherent limitations of the research method. The study included students from only one large public university. Given variability in drinking across educational settings potentially based on size, private funding, and entry criteria,41 our results may not be generalizable to all other student populations. Assessment was based on self-report, which could result in inaccurate or socially desirable reporting. Self-report of alcohol use, however, has been shown to be quite accurate in many contexts where no penalties exist for specific responses.42 Self-report indices could also reflect students' desire to please researchers, and those receiving the feedback may experience a greater demand for such reporting. Our experimental design did not include an attention-only control to test this effect. However, it is difficult to conclude that response biases would result from such a limited contact (1 hour during freshman year and mailed feedback during sophomore year), would extend for 4 years, and would produce treatment effects in one dimension but not another. Also, participants were reminded that collateral reports were obtained at each assessment point to encourage honest responding.
Although our data are consistent with a broad literature showing that brief interventions are effective in reducing alcohol and drug use,43 to date, we do not know more precisely how these interventions work (our data suggest that developmental processes underlying drinking reduction and drinking escalation might be affected). Nor do we know the critical components for content and delivery of the preventive intervention. Is the primary component merely increased attention to the issue? Can interventions based on this component be conducted by peers in groups or with only mailed feedback? Continued research on these types of issues will facilitate the adoption of effective prevention programming and the continued reduction in harm based on youthful heavy drinking.
Acknowledgments
This research was supported by grant R37 AA05591 from the National Institute on Alcohol Abuse and Alcoholism.
We gratefully acknowledge the support and assistance in the preparation of this report of Thad Leffingwell, Maxine Pollock, Dan Neal, and Lisa Roberts. Others providing essential support for the ongoing management of the research project include Mary Larimer, Jason Kilmer, Lori Quigley, and Ken Weingardt.
J. S. Baer, D. R. Kivlahan, and G. A. Marlatt designed the study, obtained funding, and supervised data collection. A. W. Blume assisted in data management, conducted data analyses, and wrote parts of the “Methods” section. P. McKnight conducted mixed model and individual change data analyses and wrote parts of the “Results” section. J. S. Baer wrote the initial draft of all other sections. D. R. Kivlahan served as primary editor. All authors contributed to editing and revision.
Peer Reviewed
References
- 1.Ninth Special Report to the US Congress on Alcohol and Health. Washington, DC: US Dept of Health and Human Services; 1997.
- 2.Institute of Medicine. Broadening the Base of Treatment for Alcohol Problems. Washington, DC: National Academy Press; 1990. [PubMed]
- 3.Schulenberg J, Maggs JL, Long SW et al. The problem of college drinking: insights from a developmental perspective. Alcohol Clin and Exp Res. 2001;25:473–477. [PubMed] [Google Scholar]
- 4.Wechsler H, Davenport A, Dowdall G, Moeykens B, Castillo S. Health and behavioral consequences of binge drinking in college. A national survey of students at 140 campuses. JAMA. 1994;272:1672–1677. [PubMed] [Google Scholar]
- 5.Camatta CD, Nagoshi CT. Stress, depression, irrational beliefs, and alcohol use and problems in a college student sample. Alcohol Clin Exp Res. 1995;19:142–146. [DOI] [PubMed] [Google Scholar]
- 6.Havey JM, Dodd DK. Variables associated with alcohol abuse among self-identified collegiate COAs and their peers. Addict Behav. 1993;18:567–575. [DOI] [PubMed] [Google Scholar]
- 7.Brennan AF, Walfish S, AuBuchon P. Alcohol use and abuse in college students, I: a review of individual and personality correlates. Int J Addict. 1986;21:449–474. [DOI] [PubMed] [Google Scholar]
- 8.Kushner MG, Sher KJ, Erickson DJ. Prospective analysis of the relation between DSM-III anxiety disorders and alcohol use disorders. Am J Psychiatry. 1999;156:723–732. [DOI] [PubMed] [Google Scholar]
- 9.Cashin JR, Presley CA, Meilman PW. Alcohol use in the Greek system: follow the leader? J Stud Alcohol. 1998;59:63–70. [DOI] [PubMed] [Google Scholar]
- 10.Gfroerer JC, Greenblatt JC, Wright DA. Substance use in the US college-age population: differences according to educational status and living arrangement. Am J Public Health. 1997;87:62–65. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Leichliter JS, Meilman PW, Presley CA, Cashin JR. Alcohol use and related consequences among students with varying levels of involvement in college athletics. J Am Coll Health. 1998;46:257–262. [DOI] [PubMed] [Google Scholar]
- 12.Rosenbluth J, Nathan PE, Lawson DM. Environmental influences on drinking by college students in a college pub: a behavioral observation in the natural environment. Addict Behav. 1978;3:117–121. [DOI] [PubMed] [Google Scholar]
- 13.Wechsler H, Dowdall GW, Davenport A, Castillo S. Correlates of college student binge drinking. Am J Public Health. 1995;85:921–926. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Johnston LD, O'Malley PM, Bachman JG, eds. National Survey Results on Drug Use From the Monitoring the Future Study, 1975–1995, Vol 1: Secondary School Students. Rockville, Md: National Institute on Drug Abuse; 1995. NIH publication 95-4026.
- 15.Donovan JE, Jessor R, Jessor L. Problem drinking in adolescence and young adulthood: a follow-up study. J Stud Alcohol. 1983;44:109–37. [DOI] [PubMed] [Google Scholar]
- 16.Jessor RJ, Donovan JE, Costa FM. Beyond Adolescence: Problem Behavior and Young Adult Development. Cambridge, England: Cambridge University Press; 1991.
- 17.Schulenberg J, O'Malley PM, Bachman JG, Wadsworth KN, Johnston LD. Getting drunk and growing up: trajectories of frequent binge drinking during the transition to young adulthood. J Stud Alcohol. 1996;57:289–304. [DOI] [PubMed] [Google Scholar]
- 18.Moskowitz JM. The primary prevention of alcohol problems: a critical review of the research literature. J Stud Alcohol. 1989;50:54–88. [DOI] [PubMed] [Google Scholar]
- 19.Baer JS. Etiology and secondary prevention of alcohol problems with young adults. In: Baer JS, Marlatt GA, McMahon RJ, eds. Addictive Behaviors Across the Lifespan. Newbury Park, Calif: Sage Publications; 1993:111–137.
- 20.Dimeff LA, Baer JS, Kivlahan DR, Marlatt GA. Brief Alcohol Screening and Intervention for College Students: A Harm Reduction Approach. New York, NY: Guilford Press; 1999.
- 21.Marlatt GA, Baer JS, Kivlahan DR, et al. Screening and brief intervention for high-risk college student drinkers: results from a two-year follow-up assessment. J Consult Clin Psychol. 1998;66:604–615. [DOI] [PubMed] [Google Scholar]
- 22.Roberts LJ, Neal DJ, Kivlahan DR, Baer JS, Marlatt GA. Individual drinking changes following a brief intervention among college students: clinical significance in an indicated preventive context. J Consult Clin Psychol. 2000;68:500–505. [DOI] [PubMed] [Google Scholar]
- 23.White HR, Labouvie EW. Towards the assessment of adolescent problem drinking. J Stud Alcohol. 1989;50:30–37. [DOI] [PubMed] [Google Scholar]
- 24.Johnston LD, O'Malley PM, Bachman JG, eds. National Survey Results on Drug Use From the Monitoring the Future Study, 1975–1995, Vol 2: College Students and Young Adults. Rockville, Md: National Instutite on Drug Abuse; 1999. NIH publication 99-4661.
- 25.Collins RL, Parks GA, Marlatt GA. Social determinants of alcohol consumption: the effects of social interaction and model status on the self-administration of alcohol. J Consult Clin Psychol. 1985;53:189–200. [DOI] [PubMed] [Google Scholar]
- 26.Skinner HA, Horn JL. Alcohol Dependency Scale (ADS). Toronto, Ontario: Addiction Research Foundation; 1984.
- 27.Helzer JE, Robins LN. The Diagnostic Interview Schedule: its development, evolution, and use. Soc Psychiatry Psychiatr Epidemiol. 1988;23:6–16. [DOI] [PubMed] [Google Scholar]
- 28.Miller WR, Marlatt GA. Brief Drinker Profile. Odessa, Fla: Psychological Assessment Resources; 1984.
- 29.Murray DM, Perry CL. Measurement of substance use among adolescents: when is the “bogus pipeline” method needed? Addict Behav. 1987;12:225–233. [DOI] [PubMed] [Google Scholar]
- 30.Miller WR, Rollnick S. Motivational Interviewing: Preparing People for Change. New York, NY: Guilford Press; 1991.
- 31.Little RJA, Rubin DB. Statistical Analysis With Missing Data. New York, NY: John Wiley & Sons; 1987.
- 32.Schaefer JL. Analysis of Incomplete Multivariate Data. London, England: Chapman & Hall; 1997.
- 33.Gorsuch R. Factor Analysis. 2nd ed. Hillsdale, NJ: Lawrence Erlbaum; 1983.
- 34.Shadish WR. Planned critical multiplism: some elaborations. Behav Assess. 1986;8:75–103. [Google Scholar]
- 35.Little RC, Millken GA, Stoup WW, Wolfinger RO. SAS System for Mixed Models. Cary, NC: SAS Institute; 1996.
- 36.Efron B, Tibshirani RJ. An Introduction to Bootstrap. London, England: Chapman & Hall; 1993.
- 37.Jacobson NS, Traux P. Clinical significance: a statistical approach to defining meaningful change in psychotherapy research. J Consult Clin Psychol. 1991;59:12–19. [DOI] [PubMed] [Google Scholar]
- 38.Baer JS, Marlatt GA, Kivlahan DR, Fromme K, Larimer M, Williams E. An experimental test of three methods of alcohol risk reduction with young adults. J Consult Clin Psychol. 1992;60:974–979. [DOI] [PubMed] [Google Scholar]
- 39.Baer JS, Kivlahan DR, Marlatt GA. High-risk drinking across the transition from high school to college. Alcohol Clin Exp Res. 1995;19:54–61. [DOI] [PubMed] [Google Scholar]
- 40.Marlatt GA. Harm Reduction: Pragmatic Strategies for Managing High-Risk Behaviors. New York, NY: Guilford Press; 1998.
- 41.Wechsler H, Molnar BE, Davenport AE, Baer JS. College alcohol use: a full or empty glass? J Am Coll Health. 1999;47:247–252. [DOI] [PubMed] [Google Scholar]
- 42.Babor TF, Stephens RS, Marlatt GA. Verbal report methods in clinical research on alcoholism: response bias and its minimization. J Stud Alcohol. 1987;48:410–424. [DOI] [PubMed] [Google Scholar]
- 43.Wilk AI, Jensen NM, Havighurst TC. Meta-analysis of randomized control trials addressing brief interventions in heavy alcohol drinkers. J Gen Intern Med. 1997;12:274–283. [DOI] [PMC free article] [PubMed] [Google Scholar]