

In many disease registries, including cancer registries, misclassification of American Indian and Alaska Native (AI/AN) race is common. This type of misclassification threatens the validity of existing estimates of disease occurrence in this population.1–9 From a public health perspective, the underestimation of cancer incidence has a potentially great effect, as appropriate cancer control measures are less likely to be implemented in light of spuriously low rates. The problem of racial misclassification of AI/AN race in cancer registries appears to be widespread: investigators in several states have shown that AI/AN race is frequently underreported in both federally sponsored and state-supported cancer registries.4–8
We conducted record linkage studies to evaluate the extent of racial misclassification of AI/ANs in the cancer registries for Idaho, Oregon, and Washington states that constitute the administrative unit of the Indian Health Service (IHS) known as the Portland Area IHS. We also calculated estimates of cancer incidence among AI/ANs in these states.
METHODS
We obtained cancer data for the years 1996 and 1997 from the Oregon State Cancer Registry, the Washington State Cancer Registry, and the Cancer Data Registry of Idaho. All 3 registries adhere to strict quality control guidelines as established by the North American Association of Central Cancer Registries. We obtained a roster of Northwest AI/ANs from the Portland Area IHS area patient file, a compilation of patient demographic data from Indian health care facilities in Idaho, Oregon, and Washington. The file included 122 938 records at the time of our linkages with the state cancer registries. Eligibility for services by IHS requires that a person have documentation of membership in or descent from an enrolled member of a federally recognized tribe. All non–AI/ANs were removed from the cleaned enrollment file (the Northwest Tribal Registry [NTR]) that we used for the linkage. The NTR includes information on percentage of AI or AN heritage, known as ‘blood quantum’. An enrolled tribal member whose grandparents were AI or AN, without other genetic admixture, would be considered to be of ‘full blood quantum’. A tribal member with only two of four grandparents entirely of AI or AN heritage would report 50% blood quantum. Variations in percentage AI or AN blood quantum among an enrolled tribal member’s ancestors would result in different degrees of reported AI or AN blood quantum in the NTR.
To link the state cancer registry data from 1996–1997 to the NTR, we used AutoMatch software (Version 4.2, Matchware Technologies, Inc, Kennebunk, Me, 1998), which employs probabilistic record linkage algorithms. For data analyses, we included matched records for patients identified as AI/AN by both the NTR and the cancer registries (these cases were considered “correctly classified”) and matched records for patients identified by the cancer registries as non-AI/AN (these cases were considered “incorrectly classified” by the state registries). All nonmatched records were excluded from further analyses, including cases that were classified as AI/AN in the state registry data but did not match with any individual in the NTR (Table 1 ▶).
TABLE 1.
—Results of Cancer Data Linkage Between Northwest Tribal Registry (NTR) Enrollment Files and State Cancer Registries, Northwest AI/AN Cancer Linkage Project
| Source | No. |
| NTR files | 122 938 |
| AI/ANs listed in state cancer registries 1996–1997 (before linkage study) | 332 |
| State cancer registries and NTR (matches)a | 412 |
| Coded as AI/AN in state registries and NTR | 197 |
| Coded as AI/AN in state registries but not in NTR (nonmatches) | 135 |
aThis was the analytic data file used for this study.
Denominators for rate calculations were based strictly on the NTR, and not on census information. Multiple logistic regression was used to examine factors associated with incorrect prelinkage classification of AI/AN status in the state registries.10
RESULTS
Table 1 ▶ shows the results of our record linkage for 1996–1997. Of the 412 matches, 215 cases (52.2%) were originally misclassified by the state registries as race other than AI/AN. Of the 215 racially misclassified cases, 200 (93%) were coded as White. In a multiple logistic regression model that included age, sex, year of diagnosis, and blood quantum, the most significant findings related to misclassification by the state registries were female sex (odds ratio [OR] = 1.2, 95% confidence interval [CI] = 0.8, 1.9) and low blood quantum (OR = 7.5, 95% CI = 4.0, 14.0) as compared with full blood quantum. A dose response was observed in the data, with lower Indian blood quantum associated with higher odds of misclassification (data not shown).
Of the total 412 cases (37 in situ and 375 invasive cases) considered for this report, 181 (43.9%) occurred in males and 231 (56.1%) in females. Washington State contributed the largest proportion of linked cases (66.0%), followed by Oregon (24.8%) and Idaho (9.2%). Rate calculations were based only on invasive cases. The postlinkage age-adjusted rate for invasive cancer of all sites, both sexes combined, was 257.5 per 100 000 person-years (95% CI = 219.0, 296.1). The rate for males (Table 2 ▶) was higher than the rate for females (Table 3 ▶).
TABLE 2.
—Selected Age-Adjusted Invasive Cancer Incidence Rates (per 100 000)a for Northwest American Indians (AIs) and Alaskan Natives (ANs), 1996–1997, Compared With Other AI/ANs and US Whites: Males
| Rate (95% Confidence Interval) | ||||||
| Cancer site | Northwest AI/ANs | Minnesota AIs7 | New Mexico AIs11 | Alaskan Natives12 | California AIs6;b | US Whites11 |
| Prostate | 82.2 (47.1,117.3) | 111.9 (85.8, 138.0) | 71.1 (58.9, 85.3) | 68.9 (54.0, 86.8) | 70.0 | 147.4 (146.5, 148.3) |
| Lung and bronchus | 41.1 (17.4, 64.8) | 97.1 (73.2, 121.0) | 16.6 (11.2, 23.9) | 123.1 (103.4, 145.6) | 46.7 | 71.1 (70.4, 71.7) |
| Colon-rectum | 34.9 (12.9, 56.9) | 56.5 (38.4, 74.6) | 28.0 (20.7, 37.2) | 86.5 (70.4, 105.6) | 36.6 | 51.7 (51.2, 52.2) |
| All | 269.4 (208.5, 330.3) | 441.6 (391.2, 491.9) | 247.6 (224.8, 272.1) | 439.0 (401.5, 479.3) | 257.4 | 475.4 (473.7, 477.0) |
aAdjusted to 1970 standard million.
bConfidence materials not published.
TABLE 3.
—Selected Age-Adjusted Invasive Cancer Incidence Rates (per 100 000)a for Northwest American Indians (AIs) and Alaskan Natives (ANs), 1996–1997, Compared With Other AI/Ans and US Whites: Females
| Rate (95% Confidence Interval) | ||||||
| Cancer site | Northwest AI/ANs | Minnesota AIs7 | New Mexico AIs11 | Alaskan Natives12 | California AIs6;b | US Whites11 |
| Breast | 81.1 (53.0, 109.1) | 82.9 (61.8, 104.0) | 51.7 (43.3, 61.4) | 114.0 (97.5, 132.6) | 44.7 | 113.1 (112.3, 113.8) |
| Lung and bronchus | 35.9 (15.8, 55.9) | 55.5 (37.7, 73.2) | 6.6 (3.7, 10.8) | 59.8 (47.4, 74.6) | 31.5 | 43.4 (43.0, 43.9) |
| Colon-rectum | 26.1 (9.6, 42.6) | 37.6 (22.9, 52.3) | 18.0 (13.1, 24.2) | 67.3 (54.0, 82.8) | 20.1 | 36.2 (35.8, 36.6) |
| All | 250.2 (200.1, 300.3) | 338.9 (296.3, 382.5) | 187.6 (171.3, 205.3) | 377.1 (345.9, 410.5) | 181.4 | 350.1 (348.8, 351.4) |
aAdjusted to 1970 standard million.
bConfidence materials not published.
DISCUSSION
Our data confirm that a large proportion of Northwest AI/ANs diagnosed with cancer in 1996–1997 were misclassified by state cancer registries, and that misclassification was strongly associated with low AI/AN blood quantum. Our report also documents the comparatively low rates of cancer among Northwest AI/ANs for all sites combined and for most cancer sites for which the data are adequate to make comparisons. Our findings add to the overall picture of cancer incidence among AI/ANs nationwide, and further show that cancer rates for all sites combined and for specific sites are heterogeneous among the various tribes in the United States.
Without valid and accurate cancer data, tribal communities and policymakers will be misinformed, ultimately leading to the development of inappropriate or poorly targeted public health interventions for cancer. Reduction of AI/AN racial misclassification may be partially achieved through clinician education and by training registry chart abstractors and reporting officials to look for comments about AI/AN race in medical records and other documents used at the time of cancer registration.11
FIGURE 1.
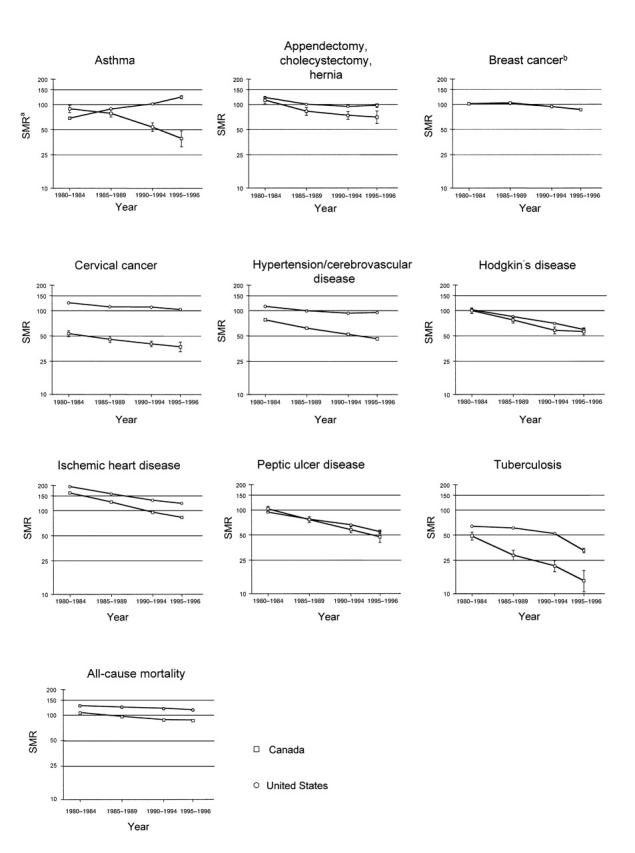
—Avoidable mortality in the United States and Canada, 1980–1996.
Acknowledgments
This research was supported by a National Cancer Institute award to the Northwest Portland Area Indian Health Board, through the Indian Health Service. The opinions expressed in this report are those of the authors, and do not necessarily reflect those of the National Cancer Institute, Northwest Portland Area Indian Health Board, or Indian Health Service.
The authors wish to thank the following colleagues for assistance with this project: Brenda Edwards, PhD; Judith Swan, MPH; Nat Cobb, MD; Charles Wiggins, PhD; Donald Austin, MD; Lori Lambert, MA; David Espey, MD, Paul Stehr-Green, DrPH; Cathie Pedersen; Esther Dunn; Grazia Ori Cunningham; and Kurt Schweigman, MPH.
Human Participant Protection Approval for this study was granted by the Indian Health Service institutional review board.
Peer Reviewed
T. M. Becker oversaw all aspects of the study design, implementation, and analysis, as well as the writing process. L. D.Robertson planned the study, designed the linkage methods, reviewed the first draft, and revised the brief. J. Bettles prepared the Northwest Tribal Registry, conducted the probabilistic record linkages with the state cancer registries, and acted as liaison with affected tribal communities. J. Lapidus imported the data from the linkage software into a statistical package, designed and ran all analyses, interpreted the results, and wrote the Results section. C. J.Johnson prepared the Idaho data for linkage, helped evaluate the results of the linkage, and helped revise the brief. J. Campo provided access to the Washington State Cancer Registry database, assessed those data in comparison with our own internal evaluation of race coding, and reviewed the initial draft. D. Shipley helped to plan and arrange the linkage and analyze and interpret the results.
References
- 1.Sugarman JR, Soderberg R, Gordon JE, Rivara FP. Racial misclassification of American Indians: its effect on injury rates in Oregon, 1989 through 1990. Am J Public Health. 1993;83:681–684. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Frost F, Tollestrup K, Ross A, Sabotta E, Kimball E. Correctness of racial coding of American Indians and Alaska Native on the Washington State death certificate. Am J Prev Med. 1994;10:290–294. [PubMed] [Google Scholar]
- 3.Sugarman JR, Lawson L. The effect of racial misclassification on estimates of end-stage renal disease among AI/AN and Alaska Natives in the Pacific Northwest, 1988 through 1990. Am J Kidney Dis. 1993;21:383–386. [DOI] [PubMed] [Google Scholar]
- 4.Frost F, Taylor V, Fries E. Racial misclassification of Native Americans in a surveillance, epidemiology and end results registry. J Natl Cancer Inst. 1992;84:957–962. [DOI] [PubMed] [Google Scholar]
- 5.Bleed DM, Risser DR, Sperry S, Hellhake D, Helgerson SD. Cancer incidence and survival among American Indians registered for Indian Health Service care in Montana, 1982–1987. J Natl Cancer Inst. 1992;84:1500–1505. [DOI] [PubMed] [Google Scholar]
- 6.Kwong SL, Perkins CI, Snipes KP, Wright WE. Improving American Indian cancer data in the California cancer registry by linkage with the Indian Health Service. J Registry Manage. 1998(February):17–20.
- 7.Partin MR, Rith-Najarian SJ, Slater JS, Korn JE, Cobb N, Soler JT. Improving cancer incidence estimates for American Indians in Minnesota. Am J Public Health. 1999;89:1673–1677. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Sugarman JR, Holiday M, Ross A, Castorina J, Hui Y. Improving American Indian cancer data in the Washington State cancer registry using linkages with the Indian Health Service and tribal records. Cancer. 1996;78:1654–1568. [PubMed] [Google Scholar]
- 9.Stehr-Green P, Bettles J, Robertson LD. Effect of racial/ethnic misclassification of American Indians and Alaskan Natives on Washington State death certificates, 1989–1997. Am J Public Health. 2002;1992:443–444. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Hosmer DW, Lemeshow S. Applied Logistic Regression. New York, NY: John Wiley & Sons Inc; 1989.
- 11.Surveillance, Epidemiology, and End Results (SEER) Program Data (1992–1996) [CD-ROM]. Bethesda, Md: National Cancer Institute; 1998.
- 12.Lanier A, Keyy JJ, Holck P, Smith B, McEvoy T. Alaska Native cancer update, by service unit and year. Anchorage: Alaska Native Health Board; 1999.
- 13.Wiggins CL, Becker TM, Thomas DB. Determinants of racial misclassification of American Indians in a central cancer registry. Abstract presented at: Annual Meeting of the North American Association of Central Cancer Registries; April 15–20, 2000; New Orleans, La.