

Abstract
Objectives. We used data gathered from 6259 youths between the ages of 13 and 23 years to compare trends in smoking among 4 racial/ethnic groups.
Methods. We weighted trend data to represent baseline respondent characteristics and evaluated these data with linear contrasts derived from multiple regression analyses.
Results. Although African Americans exhibited higher initiation rates than Whites, they exhibited consistently lower rates of regular smoking than both Whites and Hispanics. This seeming anomaly was explained by African Americans’ lower rates of transition to regular smoking and greater tendency to quit. Racial/ethnic disparities were accounted for by differences in pro-smoking influences.
Conclusions. Reducing racial/ethnic disparities in smoking may require reducing differences in the psychosocial factors that encourage smoking.
National surveys reveal striking racial/ethnic disparities in adolescent smoking behavior. Whites and Hispanics are more likely than African Americans to be current or daily smokers throughout adolescence1–5 and also appear to initiate smoking earlier.6,7 Asian youths tend to exhibit lower rates of smoking than Whites and Hispanics but not African Americans.2,8,9 Previous studies have not revealed White/non-White differences in smoking cessation rates during adolescence10,11; however, specific racial/ethnic subgroup differences have not been thoroughly examined.
Documenting racial/ethnic differences in smoking is only a starting point in understanding disparities in cigarette use. Such differences raise important questions about what factors foster group differences in smoking behavior and whether sufficient variation exists to warrant tailoring prevention and cessation programs to specific groups.12 A better understanding of the racial/ethnic context of cigarette use might shed light on how to curb its initiation and escalation during adolescence and young adulthood.13
Previous research suggests important racial/ethnic variations in 4 psychosocial and behavioral risk domains relevant to smoking: social bonds (families, school, religion), exposure to pro-smoking social influences, engagement in problem behavior, and pro-smoking attitudes. Studies have shown that, in comparison with Whites, Hispanics14,15 and Asians16 exhibit stronger levels of family attachment and that Asians17–20 exhibit greater levels of commitment to academic achievement, factors that may result in these groups being less vulnerable to pro-smoking influences and attitudes. Among African Americans, stronger religious ties6 and greater parental disapproval of smoking21,22 seem particularly protective.
In contrast, White youths typically have more friends who smoke and approve of doing so, and they may be more vulnerable than other groups to peer influences6,23,24 and parental smoking.6,16,25,26 Risk taking is a stronger predictor of smoking behavior among African Americans,25,26 whereas behavior problems are more strongly associated with smoking among Whites.26 Finally, smoking-related attitudes are important determinants of smoking behavior,27–29 and there is some evidence that their impact on smoking may vary according to race/ethnicity (e.g., the belief that smoking improves one’s self-image predicts smoking onset among White and Hispanic youths but not African American or Asian youths).26
The goal of our study, which involved a sample of youths from 4 racial/ethnic groups, was to describe trends in lifetime, past-year, and regular (weekly) smoking behaviors occurring between the ages of 13 and 23 years. We expected that, in comparison with African American and Asian youths, White and Hispanic youths would exhibit higher rates of smoking initiation by the age of 13 years and higher rates of weekly smoking over the 10-year period under study. We also examined the extent to which racial/ethnic disparities in smoking behavior could be explained by predictors drawn from the 4 described risk factor domains.
METHODS
Participants
The current sample participated in a multiyear study originally conducted to evaluate Project ALERT, a school-based drug prevention program.30 Participants were recruited from 30 California and Oregon middle schools located in urban, suburban, and rural communities. Nine schools had a minority population of 50% or more; 18 drew from neighborhoods with household incomes below their state median.
The baseline sample consisted of 6527 seventh graders. The present study included 6259 participants who completed the baseline survey (conducted in 1985) and reported their race/ethnicity as White (70%), African American (11%), Asian (11%), or Hispanic (8%). We examined 6 waves of data collected over 10 years when the participants were between the ages of 13 and 23 years. Twelve percent of the sample had dropped out of high school by the age of 18 years.
Measures
At each wave, we classified participants’ smoking status as follows: lifetime smoking (those who had ever smoked), past-year smoking (those who had smoked at least once in the past year), and weekly smoking (those who had smoked 3 or more days in the past month). Indicator variables denoting early initiation (by the age of 14 years) and late initiation (between the ages of 15 and 18 years) were created for participants who completed waves 1, 3, 7, and 8.
Participants were assessed on the 4 psychosocial/behavioral domains mentioned earlier: pro-smoking social influences (parental smoking approval, adult smoking, friends’ smoking approval, best friend and peer smoking, cigarette offers), social bonds (academic orientation, school grades, nuclear family, talking to parents about personal problems), problem behavior (deviance, rebelliousness, lifetime marijuana use, alcohol use frequency), and pro-smoking attitudes (smoking intentions, low levels of resistance self-efficacy, global smoking beliefs).
Analyses
We derived hypotheses about racial/ethnic differences in smoking outcomes based on plots that tracked observed lifetime, past-year, and weekly smoking rates among respondents from each racial/ethnic group over time (Figure 1 ▶). We evaluated these data with linear contrasts derived from multiple regression analyses. Three regression analyses involved the use of all of the available data to model each smoking outcome (lifetime, past year, weekly) as a function of race/ethnicity, study wave, and the interaction between race/ethnicity and study wave. A fourth analysis examining early initiation as a risk factor for subsequent smoking was restricted to participants who completed survey waves 1, 3, and 7 (n = 3881) or completed waves 1, 3, 7, and 8 (n = 2762).
FIGURE 1—
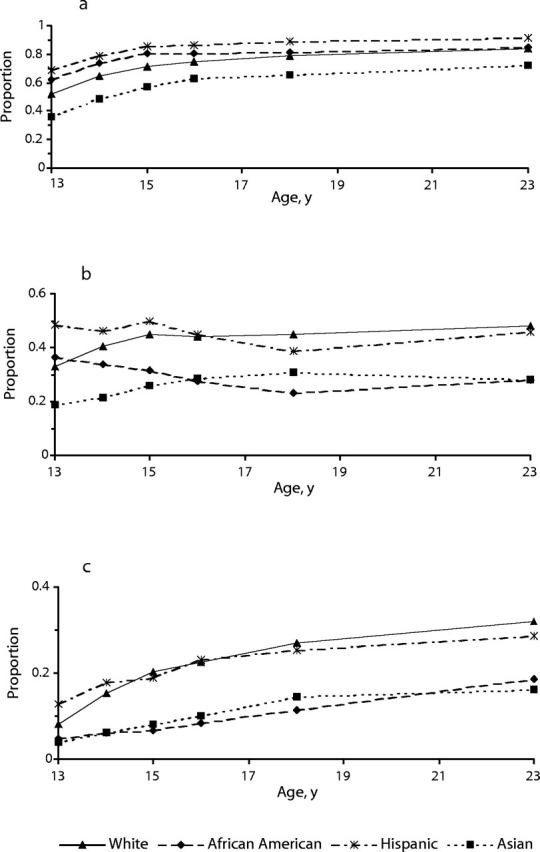
Racial/ethnic trends in (a) lifetime, (b) past-year, and (c) weekly smoking from adolescence to young adulthood.
We conducted follow-up regression analyses examining risk and protective factors associated with observed racial/ethnic differences in smoking initiation and weekly smoking. Our first models examined the extent to which each of the 4 risk factor domains measured at 13 years of age could account for the significant difference in initiation rates between White and African American adolescents at 14 years of age (based on the significance and change in magnitude of the odds ratio [OR] representing the racial/ethnic group difference when each domain of interest was included in the model relative to the original model not including any explanatory variables). We used an analogous procedure to examine differences in weekly smoking rates between Whites and African Americans, as well as between Whites and Asians, at the ages of 14 and 18 years (with predictors measured at 13 and 16 years, respectively).
Models predicting smoking rates at the age of 14 years included White, Asian, and African American participants who completed surveys at 13 and 14 years of age (n = 5857); models predicting smoking rates at 18 years included White, Asian, and African American participants who completed surveys at 16 and 18 years (n = 3591). For descriptive purposes, we also created plots of the means observed for 5 risk and protective items over time, including all participants in each wave and conducting pairwise mean comparisons among specific racial/ethnic groups for each item. We controlled for type I error rates in all pairwise mean comparisons with a Bonferroni adjustment. All analyses incorporated nonresponse weights that corrected for attrition bias31 (attrition rates ranged from 10% at wave 3 to 46% at wave 8); in addition, each analysis controlled for treatment and participant clustering within schools.
RESULTS
Smoking Initiation
Figure 1 ▶ shows 10-year trends in lifetime, past-year, and weekly smoking among Whites, Hispanics, African Americans, and Asians. By the age of 13 years, nearly 70% of Hispanic youths and more than 60% of African American youths had started smoking. Slightly more than half of all White adolescents had also initiated cigarette use, as compared with only 36% of Asian youths. By the age of 18 years, these percentages had climbed to 90% for Hispanics, 80% for Whites and African Americans, and 65% for Asians. Over the next 5 years, initiation levels rose less sharply (between 2 and 7 percentage points for all groups).
The lifetime smoking plot suggests that African Americans and Hispanics initiate smoking earlier than Whites and Asians. Pairwise comparisons of initiation rates at the age of 14 years among the 4 racial/ethnic groups revealed that significantly more African Americans and Hispanics than Whites and Asians initiated smoking (for all comparisons, P < .002). However, lifetime smoking rates across the 2 earlier-initiating groups did not significantly differ at 14 years (t29 = −1.7, P = .096).
Regular Smoking
African American youths exhibited comparatively high rates of smoking onset at the age of 13 years and thereafter; however, in comparison with Whites and Hispanics, fewer African Americans made the transition to regular (weekly) smoking. Moreover, Whites and Hispanics had substantially higher levels of regular smoking than Asians and African Americans throughout the entire period. By the age of 15 years, about 1 in 5 Hispanics and Whites had become regular smokers, as compared with 1 in 12 Asians and 1 in 14 African Americans. By the age of 23 years, regular smoking rates among Hispanics and Whites (29% and 32%, respectively) were approximately twice those among African Americans (16%) and 1.5 to 1.7 times those among Asians (19%).
Statistical tests largely supported this 2-group distinction. Hispanics and Whites were significantly more likely to be weekly smokers than Asians and African Americans at all waves, although the Asian–White contrast at 13 years was only marginally significant (P < .03 for all but the latter comparison). In addition, no significant differences existed between the proportions of weekly Hispanic and White smokers aged between 14 and 23 years or between the proportions of weekly Asian and African American smokers at any time point.
To illuminate why African Americans exhibited high initiation rates but low levels of regular smoking, we examined their past-year smoking trends, which declined between the ages of 13 and 18 years (Figure 1 ▶). We then posited and tested 2 possible explanations for the shift in smoking behavior: (1) African Americans try smoking but quit early and (2) African Americans who do not quit maintain their smoking habit at lower levels than other groups.
If the first explanation is correct, African Americans should reduce their past-year smoking rates over time more than other racial/ethnic group members. In fact, we found that past-year smoking among African Americans decreased significantly more so than among Whites (t29 = −7.7, P < .0001) and Asians (t29 = −4.6, P < .0001) but not Hispanics (t29 = −1.0, P = .303). As did African Americans, Hispanic youths tended to try smoking and then quit, exhibiting decreases in past-year smoking that were greater than those observed among Whites (t29 = −5.0, P < .0001) and Asians (t29 = −3.5, P < .001). However, because so many Hispanics initiated smoking during early and middle adolescence, quitting appeared to have less of an impact on their weekly smoking rates.
To test the second hypothesis, we looked at whether African Americans who had smoked in the past year exhibited lower levels of regular smoking than members of other racial/ethnic groups. We restricted the sample for this regression model to participants who had smoked in the past year, modeling weekly smoking as a function of race/ethnicity, time, and their interaction. Evaluation of the linear contrasts supported this explanation. Among those who had smoked in the past year, African Americans were less likely than Whites to be regular smokers at waves 1, 3, 5, and 6 (wave 1: t29 = −4.6, P < .0001; wave 3: t29 = −4.6, P < .0001; wave 5: t29 = −6.8, P < .0001; wave 6: t29 = −3.7, P < .001). They were also less likely to be weekly smokers at one or more of these time points than Hispanics (F6,24 = 7.78, P < .0001) but not Asians (F6,24 = 1.97, P = .11).
Risks of Regular Smoking
Although early initiation is a major risk factor for regular smoking in late adolescence and young adulthood,32–35 the preceding observations suggest that this may not be the case for African Americans. To test the general hypothesis that early initiation increases the risk of subsequent regular smoking and the specific hypothesis that African Americans who start smoking early are not at greater risk for regular smoking, we used data from participants who completed surveys at waves 1, 3, and 7 (to model smoking outcomes at the age of 18 years; n = 3881) and participants who completed surveys at waves 1, 3, 7, and 8 (to model smoking outcomes at the age of 23 years; n = 2762) (Table 1 ▶).
TABLE 1—
Odds of Regular Smoking at the Ages of 18 and 23 Years, by Race/Ethnicity and Time of Initiation
| Odds of Regular Smoking | ||||||
| Time of Initiation | Age at Measured Outcome | Whites | African Americans | Hispanics | Asians | Full Sample |
| Early (by 14 years)a | 18 years | |||||
| Odds ratio (SE) | 6.93 (0.84) | 2.04 (1.25) | 6.92 (3.69) | 9.48 (4.29) | 6.27 (0.77) | |
| P | <.0001 | .254 | .001 | <.0001 | <.0001 | |
| No. | 2878 | 306 | 331 | 366 | 3881 | |
| Early (by 14 years)a | 23 years | |||||
| Odds ratio (SE) | 20.71 (6.03) | 15.77 (18.09) | 8.95 (6.64) | 6.54 (2.76) | 15.77 (4.00) | |
| P | <.0001 | .023 | .006 | <.0001 | <.0001 | |
| No. | 2063 | 193 | 232 | 274 | 2762 | |
| Late (15–18 years)b | 23 years | |||||
| Odds ratio (SE) | 10.20 (3.18) | 3.77 (4.86) | 2.85 (2.94) | 2.44 (1.45) | 7.38 (1.98) | |
| P | <.0001 | .312 | .319 | .142 | <.0001 | |
| No. | 2063 | 193 | 232 | 274 | 2762 | |
aComparison group: non-initiators at 14 years.
bComparison group: non-initiators at 18 years.
The results showed that early initiators (those who started smoking by the age of 14 years) were 6 times more likely to be weekly smokers at 18 years than those who did not start smoking before high school; they were almost 16 times more likely to be weekly smokers at 23 years. Similarly, those who initiated during high school (late initiators) were 7 times more likely than non-initiators to be regular smokers at 23 years. Moreover, early initiators were twice as likely as late initiators to be regular smokers at 23 years.
However, among African Americans, early initiation was not a significant risk factor for regular smoking by late adolescence (18 years); only when they reached young adulthood (23 years) did early smoking increase their risk of becoming regular smokers. In contrast, Whites, Hispanics, and Asians who had started smoking by early adolescence were significantly more likely than nonsmokers at that age to be regular smokers by 18 years of age, a difference maintained at 23 years. In addition, initiation during high school was associated with an increased risk of regular smoking during young adulthood only among Whites.
Correlates of Racial/Ethnic Differences in Smoking
The results described thus far raise 2 questions: (1) Are the shifts in smoking behavior among African Americans also linked to preexisting or contemporaneous differences in risk and protective factors? and (2) Are Asians, who display consistently low rates of both initiation and regular smoking over time, also likely to have comparatively low-risk profiles? To address these questions, we undertook a pair of analyses. We examined whether models that included variables representing different risk factor domains closed or eliminated the gap in smoking behavior between Whites and African Americans and between Whites and Asians at the ages of 14 and 18 years. We also looked at 6-year trends in selected psychosocial variables across the 4 groups that might presage or complement their smoking patterns over time.
Table 2 ▶ (models 1–3) presents the regression results for lifetime smoking at 14 years and regular (weekly) smoking at 14 and 18 years. Model 1 shows that African Americans were 60% more likely than Whites to have started smoking by the age of 14 years. (Asian initiation levels, although lower than those observed among Whites, were not significantly different at this age.) However, adding social bonding variables at 13 years to the model accounted for the difference, reducing the odds ratio from 1.59 to a nonsignificant 1.17 (model 1B). Note that African Americans had significantly lower grades and higher rates of family disruption at the age of 13 years than did White adolescents (P < .05). Social influence variables also helped explain the difference in lifetime smoking, but they accounted for a much smaller reduction in the African American–White gap, and the difference remained significant (OR = 1.4; model 1A).
TABLE 2—
Unadjusted and Adjusted Odds Ratios for Smoking Among African Americans and Asians, Relative to Whites
| Version of Model and Adjusted Odds Ratio (95% Confidence Interval) | |||||
| Model | Unadjusted Odds Ratio (95% Confidence Interval) | A (Adds Social Influence Variables)a | B (Adds Social Bonding Variables)b | C (Adds Pro-Smoking Attitudes)c | D (Adds Problem Behaviors)d |
| Model 1 (predicting lifetime smoking at 14 yearse) | |||||
| African Americans vs Whites | 1.59* (1.20, 2.12) | 1.40* (1.07, 1.82) | 1.17 (0.89, 1.53) | 1.94* (1.54, 2.45) | 1.57* (1.15, 2.14) |
| Model 2 (predicting weekly smoking at 14 yearse) | |||||
| African Americans vs Whites | 0.36* (0.24, 0.55) | 0.35* (0.23, 0.54) | 0.28* (0.18, 0.45) | 0.39* (0.24, 0.62) | 0.30* (.19, .47) |
| Asians vs Whites | 0.36* (0.17, 0.75) | 0.55 (0.30, 0.99) | 0.49 (0.24, 1.01) | 0.46* (0.25, 0.83) | 0.54 (0.28, 1.04) |
| Model 3 (predicting weekly smoking at 18 yearsf) | |||||
| African Americans vs Whites | 0.36* (0.22, 0.57) | 0.67 (0.42, 1.05) | 0.27* (0.16, 0.45) | 0.54* (0.36, 0.82) | 0.32* (0.20, 0.52) |
| Asians vs Whites | 0.47* (0.28, 0.78) | 0.91 (0.54, 1.53) | 0.61 (0.37, 1.00) | 0.61 (0.33, 1.12) | 0.75 (0.44, 1.27) |
Note. Data were derived from logistic regression models predicting lifetime smoking at 14 years and weekly smoking at 14 and 18 years.
aModel version A includes adult smoking, parental approval of smoking, best friend and peer smoking, and peer approval of smoking and cigarette offers, plus African American and Asian ethnicity (vs White).
bModel version B includes grades, academic orientation, and disrupted family and parent–child communication, plus African American and Asian ethnicity (vs White).
cModel version C includes smoking intentions, cigarette resistance self-efficacy, and beliefs about cigarettes, plus African American and Asian ethnicity (vs White).
dModel version D includes lifetime marijuana use, frequency of alcohol use, deviance, and rebelliousness, plus African American and Asian ethnicity (vs White).
eAll predictors measured at the age of 13 years.
f All predictors measured at the age of 16 years.
*P < .025 (n = 5587 for model 1, n = 5582 for model 2, n = 3591 for model 3).
In contrast, grade 7 predictors did not account for the comparatively lower rates of regular smoking at 14 years among African Americans relative to Whites. As shown in models 2A through 2D in Table 2 ▶, the low odds ratios for African Americans remained significant and quite stable no matter which predictor blocks were added to the basic logistic regression. This is not surprising, given that the same predictors are unlikely to explain contradictory results (i.e., higher rates of lifetime smoking and lower levels of regular smoking at the same time point).
Conversely, Asians exhibited significantly lower rates of weekly smoking than Whites at 14 years and marginally lower rates of lifetime smoking. Three of the 4 predictor blocks (social influences, social bonding, and problem behaviors) accounted for this group’s lower rates of regular smoking, yielding similar odds ratio changes (from a significant odds ratio of 0.36 to nonsignificant odds ratios of 0.55, 0.49, and 0.54 in models 2A, 2B, and 2D, respectively). Including attitudinal variables also lowered the odds ratio (to 0.46), but the difference remained significant. In addition, Asians exhibited more favorable scores than Whites on most domain variables at 13 years (lower scores for parental smoking and approval, peer smoking and approval, family disruption, smoking intentions, deviance, rebelliousness, and other drug use, along with higher grades, academic orientation, and resistance self-efficacy) (P < .05).
By the age of 18 years, social influence variables measured 2 years earlier accounted for African American–White differences in regular smoking, while both social influence and problem behaviors accounted for Asian–White differences (Table 2 ▶, models 3A and 3D). The rate of weekly smoking among African Americans was only 36% that of Whites; the Asian rate was 47% that of Whites. Adding social influence variables to model 3 raised the odds ratio for African Americans to a nonsignificant 0.67; adding pro-smoking attitudes also reduced the African American–White gap (from 0.36 to 0.54), but the odds ratio remained significant. Comparisons of predictor means at 16 years showed that, relative to Whites, African Americans exhibited less pronounced smoking intentions and were exposed to significantly lower levels of parental approval and smoking, best friend and peer smoking, peer approval of smoking, and cigarette offers (P < .05).
Among Asians, adding social influence variables raised the odds ratio for weekly smoking at 18 years of age to a nonsignificant 0.91, while adding problem behaviors raised it to a nonsignificant 0.75; taking into account social bonding and attitudinal variables substantially reduced the Asian–White gap as well. Two years earlier, Asians had significantly more favorable scores than Whites on all but one of the social influence, social bonding, attitudinal, and problem behavior measures (P < .05).
These findings suggest that changes in exposure to pro-smoking social influences and changes in the development or maintenance of pro-smoking attitudes may help explain why African Americans were less likely to make the transition from experimental to regular smoking. They also indicate that maintaining lower profiles in regard to all 4 risk factor domains appeared to be important for Asians. To explore these observations further, we examined trends in 2 social influence variables (best friend’s smoking status and frequency of cigarette offers), 1 attitudinal variable (smoking intentions), 1 social bonding variable (poor grades), and 1 problem behavior (alcohol use).
Figure 2 ▶ shows that, throughout the middle and high school years, Asians maintained comparatively low rates on all of these measures. Among African Americans, in contrast, exposure to social influences actually diminished over time. Consistent with their high rates of initiation by 13 years of age, African Americans had high rates of exposure to friends who smoked and cigarette offers at 13 years, rates that paralleled those among White youths. However, their exposure rates dropped after the age of 13 or 14 years, while those among Whites rose. In addition, African Americans exhibited comparatively low smoking intentions at 13 years and, in contrast to Whites and Hispanics, did not become more inclined to smoke over time. Between ages 14 and 18 years, African Americans were consistently more likely than those in other racial/ethnic groups to maintain communication with their parents and to perceive that their parents disapproved of smoking (P < .05; data not shown).
FIGURE 2—

Racial/ethnic trends in selected risk factors between the ages of 13 and 18 years: (a) smoking intentions (b) alcohol use frequency (c) cigarette offers (d) poor school grades (e) best friend smokes.
DISCUSSION
Our analyses of smoking trends over 10 years showed that Hispanics and Whites exhibit consistently higher rates of weekly smoking than African Americans and Asians from 13 years of age through young adulthood. However, African Americans start smoking earlier than Whites and, indeed, exhibit significantly higher rates of lifetime smoking at 13 years than do White adolescents. The reason for this anomaly is that African Americans who initiate cigarette use early in adolescence are more likely to quit than Whites, or, if they continue smoking, they are more likely to maintain the habit at lower levels. Consistent with these results, we found that early initiation raised the risk of regular smoking by the age of 18 years among all groups except African Americans.
Analysis of psychosocial risk factors suggested that African American initiates are less likely to become regular smokers than Whites or Hispanics because their social environment becomes less conducive to smoking after the age of 13 or 14 years and because they do not develop strong smoking intentions (or other pro-smoking attitudes). We found that the proportion of African American youths with a best friend who smoked declined consistently between ages 13 and 18 years, while their exposure to cigarette offers diminished between ages 14 and 18 years. After 13 years of age, African Americans were also more likely than either Hispanics or Whites to experience parental disapproval of smoking and to communicate with their parents about personal problems. By 18 years, differences in previous exposure to pro-smoking social influences fully accounted for the lower rates of regular smoking exhibited by African Americans relative to Whites. Differences in pro-smoking attitudes also helped explain the gap in smoking at 18 years between these 2 racial/ethnic groups.
Among Asians, low rates of cigarette use were accounted for by consistently low scores on multiple risk factors for smoking. At the age of 14 years, controlling for prior characteristics representing each domain removed or substantially diminished the gap in rates of regular smoking between Asian and White adolescents. At 18 years, controlling for prior social influences or problem behaviors removed the gap, while controlling for social bonds or attitudes diminished it substantially.
These results suggest that efforts to change the social environment surrounding early smokers—particularly pro-smoking pressure from family and peers—might help weaken the link between early initiation and smoking escalation. They also support efforts aimed at reducing pro-smoking attitudes, improving family and school bonds, and curbing other problem behaviors.
In addition, the presence of comparatively high scores in regard to other risk factors, such as poor school performance (which predicts future smoking among adolescents36–38), can be offset by counteracting protective factors within the familial or peer environment. African American youths in this study had consistently worse grades than Whites, but their relatively good standing in terms of social influence and attitude variables after 13 years of age appeared to outweigh the potentially negative effects of weak school bonds.
Our results also indicate that late (high school) initiation is a risk factor for regular smoking among White young adults but not among young adults from other racial/ethnic groups. Although previous research suggests that social influences play a significant role in enhancing the vulnerability of White youths to increased smoking after the age of 18 years,23 further efforts are needed to identify shifts in risk and protective factors that may presage or complement this heightened risk.
The strengths of this study included our ability to compare 4 racial/ethnic groups over a relatively long time period and the rich array of psychosocial factors available for assessing differences in smoking behaviors across the groups. Another strength was our use of multiple measures of smoking over time, which yielded a richer and more nuanced picture of racial/ethnic differences and offered insights into how changes in adolescents’ environments may help reverse patterns initiated in early adolescence.
Limitations of the study included our inability to distinguish different Hispanic or Asian subgroups and our reliance on smoking self-reports and a West Coast sample that may not generalize to other cohorts or areas. However, reports of smoking in this cohort were highly accurate when externally validated and subjected to internal consistency checks.39 Furthermore, the prevalence rates observed in our sample in regard to drug use, violence, dropping out of school, and multiple problem behaviors during late adolescence were within the range typically found in national studies.31,40,41
Our results support earlier work indicating that African Americans and Asians are less likely to become regular smokers than Whites and Hispanics.3,9,42 However, our findings that African Americans start smoking earlier than Whites and are less likely to make the transition to regular smoking are new. These differences may be partly attributable to the fact that we included data from younger adolescents and examined rates of regular smoking conditional on past-year smoking. However, they may also be attributable to sample and cohort differences. Future research should seek to replicate our results in different samples involving different cohorts of young people.
Acknowledgments
This work was supported by grant 10RT-0062 from the University of California Tobacco-Related Disease Research Program.
Human Participant Protection The RAND institutional review board approved all data collection and privacy protection procedures and reviewed the study annually. Participants were informed of their right to refuse participation and the procedures for protecting data privacy. Those who agreed to complete the survey and whose parents approved their participation were included in the research process.
Contributors P. L. Ellickson, M. Orlando, and J. S. Tucker drafted and revised the article and supervised the analyses. M. Orlando and D. J. Klein conducted the analyses.
Peer Reviewed
References
- 1.Centers for Disease Control and Prevention. Tobacco use among high school students—United States, 1997. J Sch Health. 1998;68:202–204. [DOI] [PubMed] [Google Scholar]
- 2.Epstein J, Botvin G, Diaz T. Ethnic and gender differences in smoking prevalence among a longitudinal sample of inner-city adolescents. J Adolesc Health. 1998;23:160–166. [DOI] [PubMed] [Google Scholar]
- 3.Johnston LD, O’Malley PM, Bachman JG. Monitoring the Future: National Survey Results on Drug Use, 1975–2001, Volume 1: Secondary School Students. Bethesda, Md: National Institute on Drug Abuse; 2002. NIH publication 02-5106.
- 4.Kopstein A. Tobacco Use in America: Findings From the 1999 National Household Survey on Drug Abuse. Rockville, Md: Substance Abuse and Mental Health Services Administration; 2001. DHHS publication SMA02-3622.
- 5.Nelson D, Giovino G, Shopland D, Mowery P, Mills S, Ericksen M. Trends in cigarette smoking among US adolescents, 1974 through 1991. Am J Public Health. 1995;85:34–40. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Griesler PC, Kandel DB. Ethnic differences in correlates of adolescent cigarette smoking. J Adolesc Health. 1998;23:167–180. [DOI] [PubMed] [Google Scholar]
- 7.Headen SW, Bauman KE, Deane GD, Koch GG. Are the correlates of cigarette smoking initiation different for black and white adolescents? Am J Public Health. 1991;81:854–857. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Chen X, Unger JB, Cruz TB, Johnson CA. Smoking patterns of Asian-American youth in California and their relationship with acculturation. J Adolesc Health. 1999;24:321–328. [DOI] [PubMed] [Google Scholar]
- 9.Wallace JM Jr, Bachman JG, O’Malley PM, Johnston LD, Schulenberg JE, Cooper SM. Tobacco, alcohol, and illicit drug use: racial and ethnic differences among U.S. high school seniors, 1976–2000. Public Health Rep. 2002;117:S67–S75. [PMC free article] [PubMed] [Google Scholar]
- 10.McGrady GA, Pederson LL. Do sex and ethnic differences in smoking initiation mask similarities in cessation behavior? Am J Public Health. 2002;92:961–965. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Zhu S-H, Sun J, Billings SC, Choi WS, Malarcher A. Predictors of smoking cessation in U.S. adolescents. Am J Prev Med. 1999;16:202–207. [DOI] [PubMed] [Google Scholar]
- 12.Centers for Disease Control and Prevention. Tobacco use among U.S. racial/ethnic minority groups—African Americans, American Indians and Alaska Natives, Asian Americans and Pacific Islanders, and Hispanics: a report of the surgeon general. MMWR Morb Mortal Wkly Rep. 1998;47 (RR-18):2. [PubMed] [Google Scholar]
- 13.Botvin GJ, Schinke SP, Epstein JA, Botvin EM. Effectiveness of culturally focused and generic skills training approaches to alcohol and drug abuse prevention among minority adolescents: two-year follow-up results. Psychol Addict Behav. 1995;9:183–194. [Google Scholar]
- 14.Freeberg AL, Stein CH. Felt obligation towards parents in Mexican-American and Anglo-American young adults. J Soc Pers Relationships. 1996;13:457–471. [Google Scholar]
- 15.Mindel CH. Extended familism among urban Mexican Americans, Anglos, and blacks. Hispanic J Behav Sci. 1980;2:21–34. [Google Scholar]
- 16.Au JG, Donaldson SI. Social influences as explanations for substance use differences among Asian-American and European-American adolescents. J Psychoactive Drugs. 2000;32:15–23. [DOI] [PubMed] [Google Scholar]
- 17.Ellickson PL, Collins RL, Bell RM. Adolescent use of illicit drugs other than marijuana: how important is social bonding and for which ethnic groups? Subst Use Misuse. 1999;34:317–346. [DOI] [PubMed] [Google Scholar]
- 18.Johnson RA, Hoffmann JP. Adolescent cigarette smoking in U.S. racial/ethnic subgroups: findings from the National Education Longitudinal Study. J Health Soc Behav. 2000;41:392–407. [PubMed] [Google Scholar]
- 19.Sue S, Okazaki S. Asian-American educational achievements: a phenomenon in search of an explanation. Am Psychol. 1990;45:913–920. [DOI] [PubMed] [Google Scholar]
- 20.Wallace JM Jr, Bachman JG. Explaining racial/ethnic differences in adolescent drug use: the impact of background and lifestyle. Soc Problems. 1991;38:333–357. [Google Scholar]
- 21.Catalano R, Morrison D, Wells E, Gillmore M, Iritani B, Hawkins J. Ethnic differences in family factors related to early drug initiation. J Stud Alcohol. 1992;53:208–217. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Clark PI, Scarisbrick-Hauser A, Gautam SP, Wirk SJ. Anti-tobacco socialization in homes of African-American and white parents, and smoking and nonsmoking parents. J Adolesc Health. 1999;24:329–339. [DOI] [PubMed] [Google Scholar]
- 23.Ellickson PL, Perlman M, Klein DJ. Explaining racial/ethnic differences in smoking during the transition to adulthood. Addict Behav. 2003;28:915–931. [DOI] [PubMed] [Google Scholar]
- 24.Wallace JM Jr. Explaining race differences in Adolescent and young adult drug use: the role of racialized social systems. Drugs Soc. 1999;14:21–36. [Google Scholar]
- 25.Landrine H, Richardson J, Klonoff E, Flay B. Cultural diversity in the predictors of adolescent cigarette smoking: the relative influence of peers. J Behav Med. 1994;17:331–346. [DOI] [PubMed] [Google Scholar]
- 26.Sussman S, Dent C, Flay B, Hansen W, Johnson C. Psychosocial predictors of cigarette smoking onset by white, black, Hispanic, and Asian adolescents in Southern California. MMWR Morb Mortal Wkly Rep. 1987;36 (suppl 4):11–16. [PubMed] [Google Scholar]
- 27.Conrad KM, Flay BR, Hill D. Why children start smoking cigarettes: predictors of onset. Br J Addict. 1992;87:1711–1724. [DOI] [PubMed] [Google Scholar]
- 28.Flay BR, Hu FB, Richardson J. Psychosocial predictors of different stages of cigarette smoking among high school students. Prev Med. 1998;27:A9–A18. [DOI] [PubMed] [Google Scholar]
- 29.Wang MQ, Fitzhugh EC, Green BL, Turner LW, Eddy JM, Westerfield C. Prospective social-psychological factors of adolescent smoking progression. J Adolesc Health. 1999;24:2–9. [DOI] [PubMed] [Google Scholar]
- 30.Ellickson PL, Bell RM. Drug prevention in junior high: a multi-site longitudinal test. Science. 1990;247:1299–1305. [DOI] [PubMed] [Google Scholar]
- 31.Ellickson PL, Saner H, McGuigan KA. Profiles of violent youth: substance use and other concurrent problems. Am J Public Health. 1997;87:985–991. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Breslau N, Feen N, Peterson EL. Early smoking initiation and nicotine dependence in a cohort of young adults. Drug Alcohol Depend. 1993;33:129–137. [DOI] [PubMed] [Google Scholar]
- 33.Chassin L, Presson CC, Sherman SJ, Edwards DA. The natural history of cigarette smoking: predicting young-adult smoking outcomes from adolescent smoking patterns. Health Psychol. 1990;9:701–716. [DOI] [PubMed] [Google Scholar]
- 34.Ellickson PL, Tucker JS, Klein DJ. High-risk behaviors associated with early smoking: results from a 5-year follow-up. J Adolesc Health. 2001;28:465–473. [DOI] [PubMed] [Google Scholar]
- 35.Tailoi E, Wynder EL. Effect of the age at which smoking begins on frequency of smoking in adulthood. N Engl J Med. 1991;325:968–969. [DOI] [PubMed] [Google Scholar]
- 36.Choi WS, Farkas AJ, Pierce JB, Berry CC, Gilpin EA. Which adolescent experimenters progress to established smoking in the United States? Am J Prev Med. 1997;13:385–391. [PubMed] [Google Scholar]
- 37.Griesler PC, Kandel DB, Davies M. Ethnic differences in predictors of initiation and persistence of adolescent cigarette smoking in the National Longitudinal Survey of Youth. Nicotine Tob Res. 2002;4:79–93. [DOI] [PubMed] [Google Scholar]
- 38.Griffin KW, Botvin GJ, Doyle MM, Diaz T, Epstein JA. A six-year follow-up study of determinants of heavy cigarette smoking among high-school seniors. J Behav Med. 1999;22:271–284. [DOI] [PubMed] [Google Scholar]
- 39.Ellickson PL. Getting and keeping schools and kids for evaluation studies [special issue]. J Community Psychol. 1994:102–116.
- 40.Collins RL, Ellickson PL, Bell RM. Simultaneous polydrug use among teens: prevalence and predictors. J Subst Abuse. 1999;10:233–253. [DOI] [PubMed] [Google Scholar]
- 41.Ellickson PL, McGuigan KA, Adams V, Bell RM, Hays RD. Teenagers and alcohol misuse in the United States: by any definition, it’s a big problem. Addiction. 1996;91:1489–1503. [DOI] [PubMed] [Google Scholar]
- 42.Summary of Findings From the 1999 National Household Survey on Drug Abuse. Rockville, Md: Substance Abuse and Mental Health Services Administration; 2000.