

Abstract
The origin of the population health approach is an historic debate over the relationship between economic growth and human health.
In Britain and France, the Industrial Revolution disrupted population health and stimulated pioneering epidemiological studies, informing the early preventive public health movement. A century-long process of political adjustment between the forces of liberal democracy and propertied interests ensued.
The 20th-century welfare states resulted as complex political mechanisms for converting economic growth into enhanced population health. However, the rise of a “neoliberal” agenda, denigrating the role of government, has once again brought to the fore the importance of prevention and a population health approach to map and publicize the health impacts of this new phase of “global” economic growth.
THERE IS NO DEFINITIVE history of the population health approach. In living memory, the important epidemiological research published during World War II by Jerry Morris and Richard Titmuss is invoked as a seminal model of population health analysis.1–5 Morris and Titmuss carefully demonstrated that the incidence of such “individual” afflictions as juvenile rheumatism, rheumatic heart disease, and peptic ulcer all varied according to changing social conditions, such as the rate of unemployment. Along with others, they sought to widen the scope of traditional public health beyond disease prevention toward social medicine, anticipating to some extent the philosophy of the Lalonde Report and the World Health Organization’s concept of positive health.6,7 However, social medicine never successfully institutionalized itself and instead an academic and clinical epidemiology tended, if anything, to diverge from practical public health work during the postwar decades.8
The recent resurgence of the population health approach has developed from dissatisfaction with some of the limitations of a strongly individual-oriented methodology, which has characterized recent clinical epidemiology. This is a paradigm that has scored notable successes in identifying risk factors such as smoking and hypertension but that, it is argued, has become too rigid and all-pervasive, partly because of its convenience for the administrative and accounting approach of the managerial regime politically imposed on the health service sector during the 1980s.9–11 However, from a longer-term perspective, the claims of each of these methodologies can perhaps be helpfully located within a much wider-ranging debate over the relationship between economic growth and human well-being, which provides the historical context for the emergence of a concept of population health.
The modern origins of this debate lie in the late 18th century, when the focus of discussion was over the significance of the so-called “diseases of civilization,” such as gout, respiratory diseases and tuberculosis, “hysteria,” and neuroses.12 The privileged classes were becoming aware that they increasingly enjoyed a degree of freedom from some of the epidemics that continued to ravage the impoverished masses (confirmed by demographic historians, who have shown that the life expectancy from birth of the upper classes first began to exceed the average for Britain after 1750).13,14 Yet this seemed to bring the rich an increased tendency to chronic and mental diseases of “luxury.” Furthermore, the poor remained as mired in their misery as ever. What did this portend for the future health of civilization?
Sovereigns had, of course, long had a military interest in the relative populousness of their domains; with the rise of mercantilist thought from the 16th century, they were also increasingly aware of population as an index of economic strength. Towns also developed an early interest in population health, taking various measures to contain epidemics.15 But in the 18th century of progressive Enlightenment thought, the dual revolutions of republican liberty and expanding commerce in Europe and the Americas introduced a new rationalist and democratic agenda. It was increasingly coming to be assumed that the desirable goal of protection from disease should apply, in principle, equally to all citizens of a nation state. Secondly, the even more ambitious goal of positive health improvement for humans was becoming imaginable.16
Meanwhile, however, contemporaries were also faced with the contradictory evidence that the world’s first industrial revolution seemed to be having anything but obvious health benefits for the majority of the population. Enclosure and increasing farm sizes were creating rural unemployment while factory machinery rendered cottage industry redundant.17 The new industrial towns were overcrowded reception centers for destitute families seeking work. Previous efforts to devise scientific measures of health, pioneered by Graunt and Petty’s political arithmetic of London’s 17th-century bills of mortality, were now urgently redoubled, with medical men such as Dr John Heysham of Carlisle and Dr Thomas Percival of Warrington taking a lead, resulting in Joshua Milne’s first-ever accurate life table (the “Carlisle table”) in 1815.18 In the subsequent hands of William Farr, statistical superintendent in charge of Britain’s censuses and vital registration system from 1840 onwards, life table comparisons became the scientific gold standard of the Victorian public health movement in its attempts to publicize the nation’s urban health problems.19,20
We can talk of the emergence in early 19th-century France of a disciplinary school of public health and social epidemiology with its own journal (still published), Annales d’Hygiène publique et médécine légale, founded in 1829.21–24 The leading figures, such as Parent-Duchâtelet and Villermé, carefully documented the diverging incidence of mortality in different districts of Paris, relating them both to the wealth differentials of the inhabitants and to variation in sanitary facilities and services. They also demonstrated the poor health of sex workers and of child workers in the textiles industry. Their research showed that for the privileged inhabitants of salubrious areas, the march of civilization was probably a net health gain; but, equally, without careful attention to the regulation of the market economy and to the living conditions and opportunities of the masses, economic growth could have quite opposite consequences for the life chances of the populace in general. Material progress—or economic growth—apparently had ambivalent health effects.
From its origins, therefore, on both sides of the Channel, the population health approach has always been stimulated by concerns over the human costs of the excesses of economic and associated urban growth. There can be little doubt that part of the reason for the resurgence of interest in this approach during the last 2 decades has been the epidemic-scale health problems once again unleashed by unrestrained global economic and urban growth.
In England, no such academic school of public health medicine emerged (although Edinburgh University was a leading center throughout the period). This was partly because already by the 1830s several leading investigators, such as James Kay Shuttleworth, Thomas Southwood Smith, William Farr, and, above all, Edwin Chadwick, had direct access to government office.25–27 Edwin Chadwick, the éminence grise of the British central state in this period, aimed at an administrative and engineering solution to the problem of high urban death rates, the “sanitary idea.” Believing that miasma—the odors of organic decay—were the causes of epidemic disease, Chadwick created a national board of health to supervise the building of a sanitary infrastructure to ensure cleansing flows of water in and out of large cities.26,28 But in trying to force Britain’s towns to tax themselves for this purpose, Chadwick ran into a political firestorm of localist, libertarian opposition, which ended his career.29 Two decades later, the Royal Sanitary Commission of 1869 to 1871 found that no provincial cities in Britain had yet built the integrated sewers system that Chadwick’s landmark Public Health Act of 1848 had intended for them.30
Until the important franchise reforms of the period 1867 to 1884, Britain’s electorate was a “shopocracy” of small property holders, intent on low national and local property taxes. Despite the public health movement’s best efforts to publicize the appalling extent of preventable mortality in Britain’s towns, delay and prevarication was the order of the day.31 This was not helped by the capacity of key commercial interests, notably private water companies, to use the law to dispute any efforts to force them to supply adequate clean water, in an era before the germ theory and microscopic water analysis had established their scientific authority.32 There would seem to be something of a parallel here with the propensity today of wealthy tobacco companies and those dealing in other harmful products to dispute the evidence of the negative health effects of their products.33
As today’s public health movement has also found, vested interests and property rights form a formidable hydra of political and legal obstacles to the implementation of the protective measures indicated by a population health perspective. Because so many of the innovative practices and products, sanctioned by the criteria of profitability and shareholder value, can never be fully assessed in advance for the totality of their health implications, the public health movement inevitably finds itself in conflict with often-powerful commercial interests. An historical perspective shows that this is owing to the intrinsically ambivalent effects that economic growth has on population health.
ECONOMIC GROWTH AND POPULATION HEALTH: AN Ambivalent Relationship
It is still commonly assumed that it is a primary lesson of history that the process of economic growth automatically brings with it improvements in population health—at least in the long run. The evidence would seem to be compelling. We all know that before the industrial revolution, life was “nasty, brutish and short,” to cite Thomas Hobbes’s celebrated dictum. In today’s advanced economies, we all live longer and healthier lives. QED: health has improved because of economic growth.
But the human record in fact shows no necessary, direct relationship between economic advance and population health, rather a more ambivalent and contingent relationship. During the millennia of prehistory, the skeletal record indicates that it is most probable that each of the periods of transitional shift—from hunter-gatherer to early settled agriculture, early to advanced agriculture, and then to ancient urban civilization—while representing economic advance and increased human population density, was also accompanied by greater susceptibility to disease and decreased average population health. It seems most probable that only with subsequent long-term adaptation did population health recover somewhat.34 In the early modern period, it was the economically advanced towns that had the highest mortality rates.35
But when we come to the “modern” industrial revolution, and the development of scientific medicine, isn’t everything different? Well, no. The most that can be said in favor of modern economic growth is that the wealth that it accumulates creates the longer-term potential for population health improvements. But whether or not this potential is realized depends entirely on a set of quite distinct social and political negotiations and decisions on how exactly that wealth is to be used and distributed. The historical record clearly shows that the process whereby this wealth is created—economic growth itself—has no direct, necessary positive implications for population health. Indeed, in almost every historical case, the first and most direct effect of rapid economic growth has been a negative impact on population health.
Thus, the latest historical research increasingly confirms that those populations directly affected by the transatlantic transformation in economic relations driven by the British industrial revolution during the period 1780 to 1870 endured a significant negative health impact. The “demographic footprint” of this trauma remains clearly visible in the historical record of every one of the countries where it has been researched, in the form of a generation-long, negative discontinuity in the historical trends of life expectancy, infant mortality, or height attainments.36–42 In cases of later industrializers, such as Germany,43,44 Australia,45 or Japan,46 the negative health impacts also occurred, but a little later. Nor were the populations of successful industrializing economies the only ones to suffer in this process. Ireland, for instance, providing cheap labor to British and American cities and coal fields, was devastated by a famine while the London government refused to intervene in “the market”; the Indian economy, on the other hand, was carefully managed in the interests of British industry and capital, with little regard for the health or livelihood of the Indians.47–49
The notion that economic growth can automatically or necessarily deliver rising population health is a comforting myth, but it is also an elementary fallacy, resulting from imputing sufficient causation to an underspecified model containing just 2 variables. It is true that to achieve the high levels of population health enjoyed today in the West, particularly the very low rates of infant and neonatal mortality, substantial economic wealth has been a necessary precondition. But there have also been many, many other factors necessarily involved, of a social, political, ideological, and cultural nature, to convert the wealth generated by the processes of economic growth into increased population health for all. Economic growth is an intrinsically disruptive process. The history of almost all successful economies of the West shows that, in the absence of a sufficient political response at both national state and local government levels, this disruption will result in deprivations, disease, and death—the 4 D’s.50 While economic growth may be necessary, it is never a sufficient condition for improved population health.
In Britain’s case, the discontinuity in population health was extensive, lasting half a century from the 1820s until the 1870s; it contained an epicenter of epidemiological disaster during the 1830s and 1840s in the central districts of the new industrial cities, where expectation of life at birth plummeted to levels not seen since the crisis years of the Black Death (Figure 1 ▶).39
FIGURE 1—
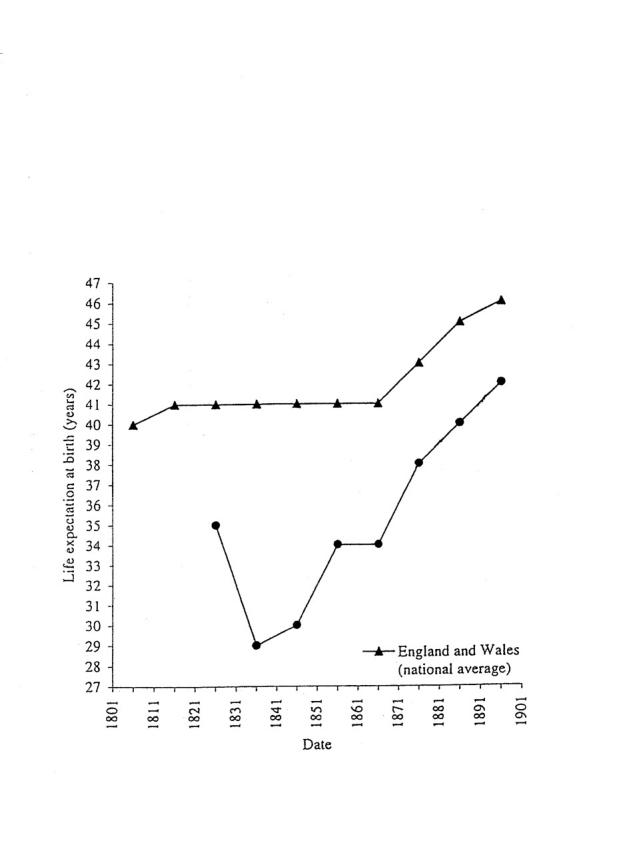
Life expectancies at birth in major British provincial cities, 1801 to 1901, compared with the national aggregate trend.
Source. Derived from Szreter and Mooney.39
Note. Britain’s industrial cities were significantly less healthy than the national average at the beginning of the 19th century. Thereafter, they were plunged into an abyss of high mortality during the 1830s and 1840s, which prompted much social comment and a Royal Commission on the Health of Towns during the 1840s. There was some recovery in the 1850s, but no real improvements above the level of the 1820s until the 1870s and the era of “the civic gospel” and municipal “gas and water socialism.”
Significant health improvements only began to appear when the increasing political voice and selforganization of the growing urban masses finally made itself heard, increasingly gaining actual voting power from the late 1860s onwards (a process not completed until 1928). The civic gospel, originating in the nonconformist pulpits of Birmingham’s more well-heeled congregations, was a bold response from neo-patrician networks of families within the new urban elites. It snowballed into a social movement promulgated throughout Britain’s proud provincial cities.51 Recognizing the need for an extensive program of investment in municipal health amenities and social services, this new generation of civic leaders devised new sources of funding from the massive revenues of local utility monopolies.
Enjoying working-class support, this political program was a prime historical example of cross-class bridging and linking social capital (i.e., relationships of respect, trust, and cooperation).52,53 Several of those campaigning in hard-fought electoral battles on the hustings, such as Joseph Chamberlain in Birmingham, were among the most successful managing directors of leading global businesses. They were assisted by the newly consolidating cadres of public service professionals, notably Medical Officers of Health.51,54–56 By the first decade of the 20th century, major British cities like Birmingham, Liverpool, and Manchester were virtually welfare states in miniature.
This is not just history. The recent transformation in salubrity of the large Indian city of Surat, hit by plague in September 1994, illustrates many of the same key factors regarding local political leadership and cross-class alliances.57 Similarly, current developments in the Brazilian city of Porto Alegre demonstrate how the political mobilization of the poor and of cross-class bridging and linking social capital can change a city’s environment and health58; in this latter case, the change may be all the more secure than in Surat because of more thoroughgoing mobilization and participation of the population.59
A not dissimilar pattern is visible in late 19th-century US history, where the franchise was already a wide one and the more broadly based middle classes played a more central role in the sanitarian and urban reform movements, led by medical and other professionals.53,60–64 The net result, in the United States, Britain, and Europe (where such reform tended to be more exclusively elite and state led),24,44,65 was that the urban middle classes agreed to greater taxes on their wealth and property, while the working classes often incurred increased indirect taxes (through their use of monopoly municipal services such as gas and tramways, for instance) to make the necessary hefty investments in enhancing and maintaining the overall urban environment. This included sanitary systems and public housing, paved and cleansed roads, and health promotion services, from food inspectors to universal education, maternity services to public baths.50,62,65–70
In an era when self-help, laissez-faire, and suspicion of central government was still the ideological order of the day in the Anglo-Saxon polities on both sides of the Atlantic, the central state’s role was primarily exhortatory, restricted to providing information about death rates and some financial carrots and inspectional sticks—and even this was more true of Britain than of the United States.19,20,61,71,72 In both countries, the role of municipal government was critical. Elsewhere, on the crowded continent of Europe and in Japan, national security fears and imperial rivalries had already been conducive to a more precocious interest on the part of the state in both the quality and the quantity of the nation’s supply of manpower—famously so in the case of Bismarck’s innovative, early German social insurance legislation of the 1880s, the efficiency of Japan’s military medicine,46 and the French state’s policies aimed at promoting high birth rates after its defeat in the Franco-Prussian war of 1870 to 1871.73 Eventually, also motivated by military fears, the early 20th-century British state under the “New Liberals” began to enact Bismarckian-style, centrally funded measures aimed at improving the health and physique of its urban industrial work-force.74 Even the US federal government finally followed suit in the New Deal and post–World War II era.
For the liberal, democratic industrialized nations, the 20th century has exhibited a substantial embedding and institutionalization of a widening range of mainly state-organized and tax-funded preventive health, educational, and social services, which between them consume a substantial proportion of the growing national income. It has been these extensive “welfare states” that have primarily provided the crucial mechanism enabling these societies to continue to experience relatively rapid rates of economic growth throughout long periods of the 20th century, while minimizing the disruptive impacts on people’s livelihoods that rapid economic change necessarily entails. Where welfare principles have been most thoroughly institutionalized and devolved (in terms of their management), as in corporate Japan or universalist Scandinavia, these societies have succeeded in routinely transforming such growth into enhanced bodily health and ever-increasing longevity for the majority of their citizens, resulting in the highest average life expectancies in the world.
Indeed, the Swedish historical case is in a sense the exception that proves the rule. Industrialization came very late in the 19th century to Sweden, and it appears to have avoided the worst consequences of the “4 D’s.” However, this was because Sweden was a state that had been carefully monitoring its population health since 1749, and it was used to working through devolved, local initiative, an administrative necessity in such a large country of scattered settlements. Sweden passed comprehensive public health legislation in 1874, at exactly the same time as Britain’s important second Public Health Act.75 But in Sweden’s case, this was in anticipation of, not following the ravages of, industrial urban growth. Thus, in Sweden, as in the 20th century more generally, economic growth was carefully politically regulated and managed—in a devolved and not centralized fashion—to ensure that population health was improved, not compromised.
FORGETTING HISTORY: THE WASHINGTON CONSENSUS
The importance and difficulty of this extraordinary political and administrative achievement of creating effective welfare institutions, so as to consistently convert raw, intrinsically disruptive economic growth into enhanced population health for the majority of the citizenry, have been profoundly underestimated, if not completely ignored, in the policy priorities of the international development orthodoxy of the late 20th century. Instead, there has emerged, under the auspices of the neoliberal “Washington consensus,” a relentless overemphasis on the promotion of free trade and rapid economic growth, first and foremost, and even at the expense of government investment in welfare and health services. To understand how such a misleading “commonsense” position could have become so dominant, we need to review briefly the main ideas that continue to inform that consensus, insofar as it relates to population health issues.
From the outset of the postwar era, the overarching theory of demographic transition always strongly implied that economic growth alone was the ultimate source of benevolent demographic change. According to this theory, nations one after another have moved from the undesirable, premodern “high-pressure” equilibrium of high birth rates and high death rates to the more efficient and rational “lowpressure” regime of low vital rates, exemplified in the modernized West.76,77 Economic growth is posited as the beneficent motor force standing behind all this. It effected reductions in mortality by increasing per capita incomes and food supply and by placing ever-greater resources in the hands of increasingly scientific and professional medicine, facilitating the release of mankind from the historic burden of infectious disease and poor nutrition; transition theory posited that fertility decline then followed in response to increased child survival.
The postwar international public health, family planning, demographic, and development communities took it as their humanitarian mission to bring about this demographic transition in as many other countries as possible.78 From the end of the 1950s, they found themselves the beneficiaries of plentiful resources for these activities from Western governments and from US philanthropic foundations, as the Cold War rivalry with the world’s communist states intensified.79–81
Demographic transition theory was, in fact, the projection onto earlier history of the seemingly miraculous experience of the generation in the West who came to maturity in the interwar decades of the 20th century. They and their children were the first generations to truly benefit from the multiple life-preserving and therapeutic practical applications of the sequence of profound late 19th-century scientific breakthroughs upon which modern medical science is based: evolutionary theory, germ theory, microscopy, bacteriology, and nutritional physiology.56,82
But as a theory to account for mortality change in the 2 previous centuries, the demographic transition theory rested on slender historical evidence.83 The rigorous historical demographic research of the Cambridge Group for the History of Population and Social Structure (analyzing data from hundreds of English parish registers dating from the 1540s) has conclusively shown that for the key case of England, it was not, after all, declining mortality that was primarily responsible for the massive population growth during the period 1750 to 1850 but rising fertility brought about by falling age at marriage.14,84 In Britain, mortality did not fall significantly until 1870, two decades after the industrial revolution was completed. In fact, the demographic transition, as a general theory, has been refuted time and again—for instance, it has long been known that in the 2 substantial cases of France and the United States, fertility fell before mortality.85,86
In addition to transition theory, the separate historical epidemiological research of Thomas McKeown on Britain’s detailed civil registers of deaths for the period after 1850 has been very influential in giving sustenance to the view that economic growth has a directly benevolent effect on population health. McKeown is rightly celebrated as a great iconoclast, who accurately aimed an important blow at the status and power of clinical, scientific medicine, which he saw as abrogating far too much of the nation’s resources to its own professional agenda.87 McKeown conclusively demonstrated that medical science could not have accounted for more than a tiny fraction of any improvement in mortality that had occurred before the 1930s, when sulfonamides and antibacterial agents finally arrived.
McKeown’s work, however, also had the effect of further reinforcing the simplistic economic determinism of demographic transition theory. This was because he explicitly demoted public health medicine—which he termed “municipal sanitation”—to a lowly second place, an also-ran in his account, while concluding that improved living standards, notably rising nutrition, had been primarily responsible for most mortality reduction before the 1930s.88,89 This left the impression of an even more direct link between economics and health than in classic transition theory, which had assumed that medical science also performed an essential role.
McKeown’s message was highly convenient for the neoliberal ascendancy within the field of economics during the late 1970s and 1980s. Johansson has pointed out the significance of the fact that at this time McKeown’s interpretation received endorsement from an influential intermediary, Robert Fogel, the Chicago-based Nobel laureate in economics, in his initial historical anthropometric work (on trends in heights and weights).90 The strategy of the neoliberal Washington consensus was to maximize the scope for free market economic growth, reducing all government-provided, tax-funded public services, including free health and allied social services. McKeown had supposedly shown these to be of far less value than a booming economy where health improvements were concerned.
Larger ideological and geopolitical forces were clearly at play here. The rising ascendancy of the New Right benefited politically from a widespread practical disengagement from policy issues during the 1980s by the intellectual left, which became preoccupied with more abstract issues of philosophical relativism—“postmodernism.” One of its most influential figures, Michel Foucault, focused his relativist assault on both the authority of medicine and the legitimacy of the nation-state and its “official” forms of knowledge, through an examination of the 19th-century history of its treatment of insanity and the procedures of the clinic.91,92 With its suspicion of “the state,” the capacity of the postmodernist position to provide a political challenge to the agenda of the New Right has been rather limited, especially as one of the legitimating rhetorics of the market is to extol its capacity to offer unlimited individual “choice.” The anti-authoritarian, relativist left and the radical libertarian right have thus concurred, for rather different reasons, on a vision of an anarchist utopia.
McKeown’s interpretation was taken by the New Right as meaning that “It’s the economy, stupid”; to reduce global mortality, the number one priority was to produce as much economic growth as possible. Concerns over the distribution of material wealth were papered over by free market apologists’ talk of the “trickle-down” effect—a surprisingly casual notion, lacking theoretical elaboration or empirical confirmation. Sam Preston, the doyen of US demography, launched a timely state-of-the-art, cross-national statistical demonstration to refute this aspect of McKeown’s case, arguing that medical technology, in the form of public health, had been of most importance in enhancing life expectancy, especially in the 20th century. His analysis, however, was powerless to stem the ideological flood tide in the economics profession.93,94
Poverty reduction and welfare as priorities disappeared from the international development agenda for an entire decade, in favor of “structural adjustment programs” and “conditional” loans, which slashed public spending and services in the evangelical belief that free markets could best supply most goods and services. Only in the 1990s, thanks principally to the influence of Amartya Sen’s concepts of entitlements, capabilities, and functionings,95 did explicit ethical concerns about the health and welfare outcomes of economic growth reemerge with the launching of the United Nations Development Program’s human development indicators.
A further significant step has been the recognition in the World Bank’s World Development Report for 2000/2001, Part III, and in several associated World Bank publications entitled Voices of the Poor, that empowerment—the political voice of the world’s poor—and social capital—social networks and relations of mutual respect and support—are both crucial. However, it should be noted that after the acrimonious dismissal of the World Bank’s controversial chief economist, Joe Stiglitz, who openly attacked the neoliberal Washington consensus polices of the previous decade,96,97 the bank’s 2002 report appeared to display less enthusiasm for this emphasis.
The tragedy of all this is that, during the last 2 decades of structural adjustment and conditionality, there has never been any strong historical evidence for believing in either the demographic transition theory or the McKeown thesis view that maximizing economic growth can itself produce health benefits. A discriminating evaluation of the historical evidence indicates, quite to the contrary, that without a strongly interventionist role for local government, supported with the resources of the central state, economic growth will seriously compromise population health.
Many who have accepted McKeown’s thesis still do not realize that he never presented any positive historical evidence about food and nutrition in British history. By contrast, all the historical work reviewed here has carefully shown, through primary source documentation, that a complex and continually expanding range of social and political interventions has been vital in securing widespread health benefits from the mere accumulation of material wealth. This includes watering, sewerage, the sealing and cleansing of roads, better housing, regulation of the urban food supply and environment, enhanced social security measures, the provision of widely accessible health services, and the fostering of a more democratic spread of knowledge about health and hygiene98 (for reviews, see references 69, 99, and 100).
THE POPULATION HEALTH APPROACH TODAY
Epidemiologists and public health policymakers are engaged in a reappraisal of the models that they use to investigate health problems. They have argued that methodologies have often been too narrow: “medical care is but one of many socioeconomic ‘institutions’ (e.g. income maintenance, social security, education) that affect health.”101 There has, in fact, always been a significant stream of important work since Morris and Titmuss—such as that by Graham, Susser, Marmot, Syme, and Berkman—that has explored the wider social and cultural sources of epidemiological variation.102 A number of large compilations of new research have recently appeared that begin to suggest a return to this line of investigation.103–106 Furthermore, a range of important editorial and opinion-forming contributions are now calling for a disciplinary generalization of the new approaches and for much greater environmental, ideological, and global political awareness on the part of the public health discipline.107–115
At the beginning of the third millennium, massive disruption due to rapid and relatively unregulated economic growth is once again upon us. A wide-ranging vision will be needed to produce the compelling arguments from ethical first principles and the effective strategies and policies that can cope with the health challenges it poses. Such a new alternative synthesis, embracing ethics, politics, the importance of social capital, human security, the ecological and biological sciences, and new approaches to economic affairs and their measurement, appears to be emerging, one that acknowledges that market economic growth may not, in and of itself, be the prime mover of all that is of value, especially where health is concerned.95,116–131 The public health field and epidemiological science therefore need to be formulated as a population health approach, capable of engaging with these related global, ecological, and local problems.
In these circumstances, the first, essential duty of public health epidemiologists is to measure and publicize the dimensions of damage being done to the health of populations. This activity is an essential informational prerequisite for mobilizing public opinion, and it tugs as sharply as possible on the consciences of the powerful elites, making clear to them the human costs of the wealth accumulation from which they believe they profit. It is precisely this role that a highly committed, small set of public health practitioners, in both central and local government, played in Britain during the mid-19th-century era of laissez-faire.19,20,132,133
One of the most unfortunate consequences of the Washington consensus policies of structural adjustment imposed on less advanced economies has been a weakening of essential state capacity to collect reliable vital statistics covering the most marginal sections of the population—child workers, low-paid workers, black market workers, migrants, refugees, and remote rural communities. These are the very people who are paying the principal health price for the global market economy’s “successful” growth rates, achieved through shareholder capital’s ceaseless search for the lowest labor, production, and fiscal costs.134,135 Thus, overzealous application of free market policies can even unintentionally commit “the perfect crime,” removing the epidemiological evidence of the health problems it creates. It is a primary duty of the international public health community to insist on the continuing right of all citizens to be registered and counted and the duty of all governments to collect and publicize correct, comprehensive vital statistics on all persons within their borders.
The irony of the long-term history of economic growth, the march of science, and the expansion of markets is that, as we become ever more independent from the vagaries of untamed nature, so we have become ever more intimately interdependent on ourselves, on the consequences of our collective actions, and on the enormous, complex network of relationships that we call “the market.”136 That interdependence is now more evidently global in scope than ever. The series of spectacular national financial crises that characterized the 1990s and that show no sign of abating, as much as the events and still-reverberating sequelae of September 11th, have made this painfully obvious.
However, far more insidious threats to our collective security and health are posed by the continuous and accumulating social inequality and environmental degradation produced by unregulated free market growth; these may, in the long run, be even more devastating to global population health. There is a stark contrast between the highly energetic response of the world’s power elite—in the form of the actions of the International Monetary Fund, the White House, and the Pentagon—to some of the more visible and acute political disruptions and these same institutions’ acquiescence to rising global social inequality and environmental damage, exemplified by the US president’s unilateral abandonment of the Kyoto Protocols on climate change.137
The population health approach may have a particularly important role to play in demonstrating and sensitizing public opinion to the epidemiological early warning signs of important, though gradual, environmental and ecological changes that manifest themselves only at the population level. An epidemiological approach that prefers to focus only on individuals’ bodies, lifestyles, and personal risks is less likely to detect and correctly diagnose the causes of the early effects of these gradual changes in the world’s living conditions. There is, therefore, much research that needs to be done today from a population health perspective.
Figure 2.
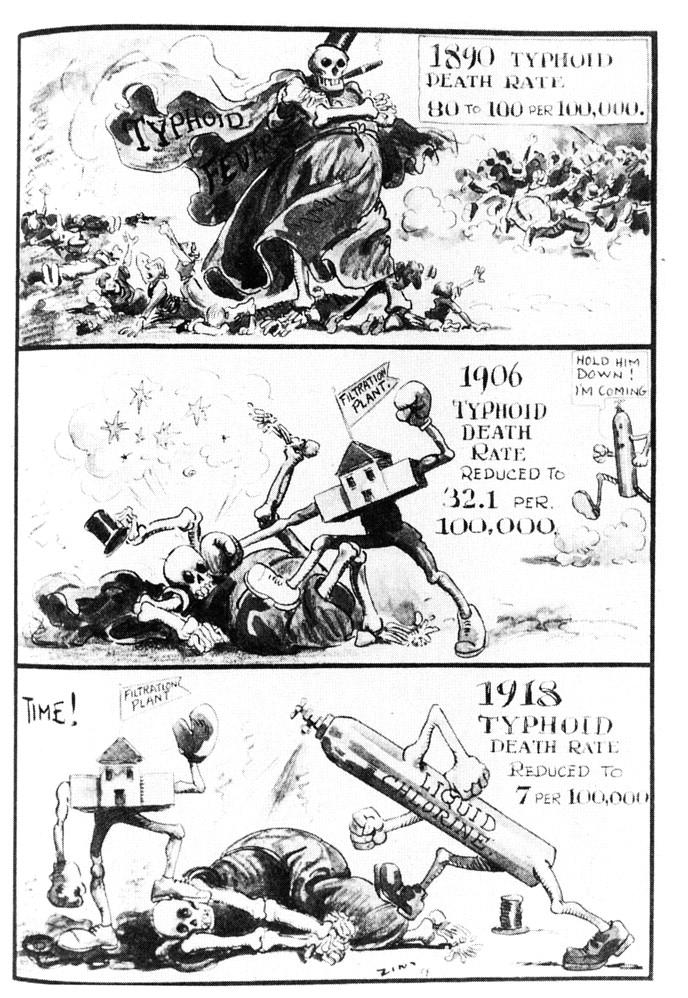
Cartoon from the September 1919 issue of the journal American City depicting the defeat of typhoid fever by the large-scale municipal measures of water filtration and chlorination. (American City. 1919;21:247.)
Figure 3.
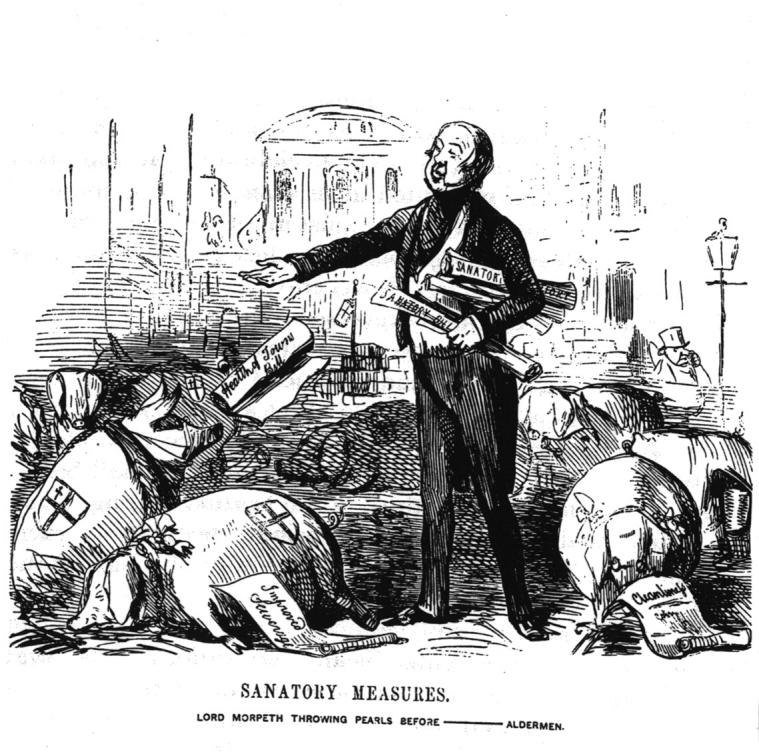
A Punch cartoon from June 1848 of Lord Morpeth, the central government’s representative, promoting the bill for Chadwick’s Public Health Act. The legislation is depicted as “sanatory” pearls being thrown in vain by the enlightened national statesman to the unappreciative “swine”: the lazy, ignorant, and venal councilors of the nation’s cities, content to wallow in their own filth.
Figure 4.
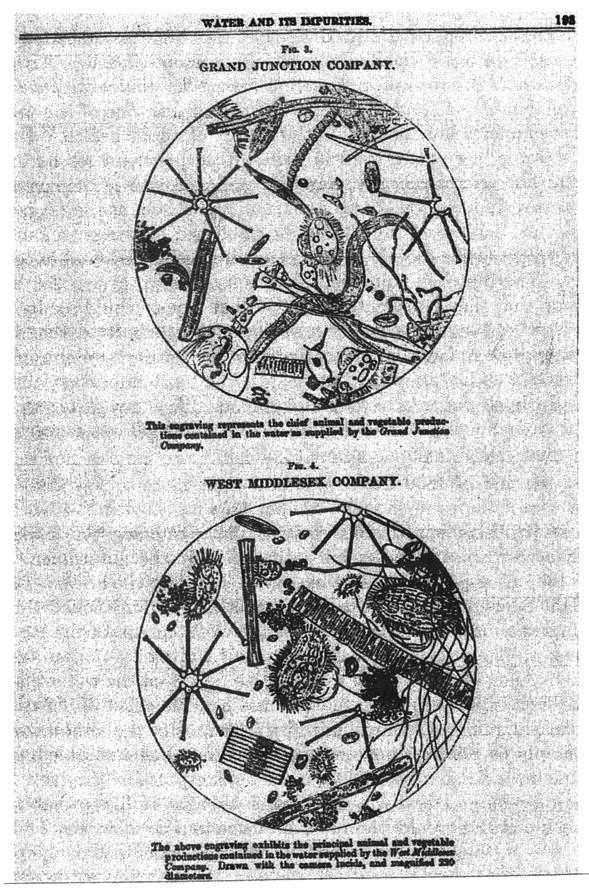
Illustrations from The Lancet of water impurity in London’s commercial supplies. By 1851, the microscope enabled water analysts to make precise drawings such as these depicting the organic contents of the drinking water supplied by London’s increasingly notorious private companies. Some of these companies’ defective systems were clearly implicated by pioneering epidemiological research into the major cholera epidemics of the period.
Figure 5.
Joseph Chamberlain, wearing his trademark monocle and occupying the moral “high ground,” fighting the 1878 Birmingham municipal election. Three decades after the failed Public Health Act, Chamberlain led the Liberal caucus, a highly organized party machine, to a series of municipal electoral victories on an ambitious platform of civic spending and improvement. These programs were to be financed from long-term loans, revenue-raising municipal services such as gas and water, and rising tax rates on property.
Acknowledgments
This article was completed while the author was an Economic and Social Research Council (ESRC) fellow (award no. R000271041).
The article benefited from the many helpful comments of Theodore M. Brown, Elizabeth Fee, Daniel Fox, Daniel J. Friedman, John Lynch, Steve Kunitz, John Powles, George Davey Smith, Barbara Starfield, and the 4 anonymous journal referees.
References
- 1.Morris JN, Titmuss RM. Epidemiology of juvenile rheumatism. Lancet. 18July1942:59–65.
- 2.Morris JN, Titmuss RM. Health and social change, I: the recent history of rheumatic heart disease. Medical Officer. August 26, September 2 and 9, 1944.
- 3.Morris JN, Titmuss RM. Epidemiology of peptic ulcer: vital statistics. Lancet. 30December1944:841–856.
- 4.Oakley A. Eugenics, social medicine and the career of Richard Titmuss in Britain 1935–50. Br J Sociol. 1991;42:165–194. [Google Scholar]
- 5.Oakley A. Man and Wife: Richard and Kay Titmuss: My Parents’ Early Years. London, England: Harper Collins; 1996.
- 6.Cochrane A. Effectiveness and Efficiency: Random Reflections on Health Services. London, England: Nuffield Provincial Hospitals Trust; 1972.
- 7.Lalonde M. A New Perspective on the Health of Canadians. Ottawa, Ontario: Canada Dept of National Health and Welfare; 1974.
- 8.Porter D, ed. Social Medicine and Medical Sociology in the Twentieth Century. Amsterdam, The Netherlands: Rodopi; 1997. [PubMed]
- 9.Rose G. Sick individuals and sick populations. Int J Epidemiol. 1985;14:32–38. [DOI] [PubMed] [Google Scholar]
- 10.Loomis D, Wing S. Is molecular epidemiology a germ theory for the end of the twentieth century? Int J Epidemiol. 1990;19:1–3. [DOI] [PubMed] [Google Scholar]
- 11.Rose G. The Strategy of Preventive Medicine. Oxford, England: Oxford University Press; 1992.
- 12.Bynum WF. Darwin and the doctors: evolution, diathesis, and germs in nineteenth-century Britain. Gesnerus. 1983;40:43–53. [PubMed] [Google Scholar]
- 13.Woods R, Williams N. Must the gap widen before it can be narrowed? Long-term trends in social class mortality differentials. Continuity and Change. 1995;10:105–137. [Google Scholar]
- 14.Wrigley EA, Davies RS, Oeppen JE, Schofield RS. English Population History From Family Reconstitution. Cambridge, England: Cambridge University Press; 1997:206.
- 15.Cipolla CM. Public Health and the Medical Profession in the Renaissance. Cambridge, England: Cambridge University Press; 1976.
- 16.Riley J. The Eighteenth Century Campaign to Avoid Disease. London, England: Macmillan; 1987.
- 17.Thompson EP. The Making of the English Working Class. Harmondsworth, England: Penguin Books; 1968.
- 18.Glass DV. The Development of Population Statistics. Farnborough, England: Greg International; 1973.
- 19.Eyler JM. Victorian Social Medicine. Baltimore, Md: Johns Hopkins University Press; 1979.
- 20.Szreter S. The GRO and the public health movement 1837–1914. Soc Hist Med. 1991;4:435–463. [DOI] [PubMed] [Google Scholar]
- 21.Ackernecht EH. Hygiene in France, 1815–48. Bull Hist Med. 1948;22:117–155. [PubMed] [Google Scholar]
- 22.Coleman W. Death Is a Social Disease: Public Health and Political Economy in Early Industrial France. Madison: University of Wisconsin Press; 1982.
- 23.La Berge AF. The early nineteenth-century French public health movement: the disciplinary development and institutionalisation of Hygiène Publique. Bull Hist Med. 1984;58:363–379. [PubMed] [Google Scholar]
- 24.La Berge AF. Mission and Method: The Early Nineteenth-Century French Public Health Movement. Cambridge, England: Cambridge University Press; 1992.
- 25.La Berge AF. Edwin Chadwick and the French connection. Bull Hist Med. 1988;62:23–41. [PubMed] [Google Scholar]
- 26.Flinn MW, ed. Report on the Sanitary Condition of the Labouring Population of Great Britain by Edwin Chadwick 1842. Edinburgh, Scotland: Edinburgh University Press; 1965.
- 27.Cullen MJ. The Statistical Movement in Early Victorian Britain. Hassocks, England: Harvester Press; 1975.
- 28.Hamlin C. Public Health and Social Justice in the Age of Chadwick: Britain, 1800–1854. Cambridge, England: Cambridge University Press; 1998.
- 29.Prest J. Liberty and Locality: Parliament, Permissive Legislation, and Ratepayers’ Democracies in the Mid-Nineteenth Century. Oxford, England: Clarendon Press; 1990.
- 30.Szreter S. The importance of social intervention in Britain’s mortality decline c. 1850–1914: a reinterpretation of the role of public health. Soc Hist Med. 1988;1:1–37. [Google Scholar]
- 31.Hamlin C. Muddling in Bumbledon: on the enormity of large sanitary improvements in four British towns, 1855–1885. Victorian Stud. 1988;32:55–83. [PubMed] [Google Scholar]
- 32.Hamlin C. A Science of Impurity: Water Analysis in Nineteenth-Century Britain. Bristol, England: Adam Pilger; 1990.
- 33.Berlinguer G. Everyday Bioethics: Reflections on Bioethical Choices in Daily Life. New York, NY: Baywood; 2002:chap 5.
- 34.Cohen MN. Health and the Rise of Civilisation. London, England: Yale University Press; 1989:chap 7.
- 35.Wrigley EA. A simple model of London’s importance in the changing British society and economy, 1650–1750. Past and Present. 1967;37:44–70. [Google Scholar]
- 36.Bourdelais P, Demonet M. The evolution of mortality in an industrial town: Le Creusot in the nineteenth century. Hist Fam. 1996;1:183–204. [DOI] [PubMed] [Google Scholar]
- 37.Pelletier F, Legare J, Bourbeau R. Mortality in Quebec during the nineteenth century: from state to the cities. Popul Stud. 1997;51:93–103 (Table 2). [DOI] [PubMed] [Google Scholar]
- 38.Weir DR. Economic welfare and physical well-being in France 1750–1990. In: Steckel RH, Floud R, eds. Health and Welfare During Industrialization. Chicago, Ill: University of Chicago Press; 1997:161–200 (Fig 5.8, 5.10).
- 39.Szreter S, Mooney G. Urbanisation, mortality and the standard of living debate: New estimates of the expectation of life at birth in nineteenth-century British cities. Econ Hist Rev. 1998;50:84–112. [Google Scholar]
- 40.Horlings E, Smit J-P. The quality of life in the Netherlands 1800–1913. In: Komlos J, Baten J, eds. The Biological Standard of Living in Comparative Perspective. Stuttgart, Germany: Steiner Verlag; 1998:321–343.
- 41.Haines MR. The urban mortality transition in the United States, 1800–1940. Annales de Démographie Historique. 2001:33–64.
- 42.Bengtsson T, Dribe M. New Evidence on the Standard of Living in Sweden During the 18th and 19th Centuries: Long-Term Development of the Demographic Response to Short-Term Economic Stress Among Landless in Western Scania. Danish Center of Demographic Research; September 2000. Research Report 16. Available at: http://www.ekh.lu.se/ekhmdr/workpap.htm. Accessed December 5, 2002.
- 43.Twarog S. Heights and living standards in Germany, 1850–1939: the case of Wurtemberg. In: Steckel RH, Floud R, eds. Health and Welfare During Industrialization. Chicago, Ill: University of Chicago Press; 1997:285–330.
- 44.Vogele J. Urban Mortality Change in England and Germany, 1870–1914. Liverpool, England: Liverpool University Press; 1998.
- 45.Whitwell G, de Souza C, Nicholas S. Height, health and economic growth in Australia 1860–1940. In: Steckel RH, Floud R, eds, Health and Welfare During Industrialization. Chicago, Ill: University of Chicago Press; 1997:379–422.
- 46.Johansson SR, Mosk C. Exposure, resistance and life expectancy: disease, and death during the economic development of Japan, 1900–60. Popul Stud. 1987;41:207–235. [DOI] [PubMed] [Google Scholar]
- 47.Neal F. Black ’47: Britain and the Irish Famine. Basingstoke, England: Macmillan; 1998.
- 48.Watts S. Epidemics and History: Disease, Power and Imperialism. London, England: Yale University Press; 1997.
- 49.Davis M. Late Victorian Holocausts. El Nino Famines and the Making of the Third World. London, England: Verso; 2001.
- 50.Szreter S. Economic growth, disruption, deprivation, disease and death: on the importance of the politics of public health for development. Popul Dev Rev. 1997;23:693–728. [Google Scholar]
- 51.Hennock EP. Fit and Proper Persons. Montreal, Quebec: McGill-Queen’s University Press; 1973.
- 52.Woolcock M. Managing risk, shocks, and opportunity in developing economies: the role of social capital. In: Ranis G, ed. Dimensions of Development. New Haven, Conn: Yale Center for International and Area Studies; 2000:197–212.
- 53.Szreter S. The state of social capital: bringing back in power, politics and history. Theory Soc. 2002;31:573–620. [Google Scholar]
- 54.Wohl AS. Endangered Lives. Public Health in Victorian Britain. London, England: J.|M. Dent; 1983.
- 55.Hardy A. Public health and the expert: the London Medical Officers of Health, 1856–1900. In: MacLeod R, ed. Government and Expertise. Specialists, Administrators, and Professionals, 1860–1919. Cambridge, England: Cambridge University Press; 1988:128–142.
- 56.Hardy A. Health and Medicine in Britain Since 1860. London, England: Palgrave; 2001.
- 57.Shah G. Public Health and Urban Development: The Plague in Surat. London, England: Sage; 1997.
- 58.Abers R. From clientalism to cooperation: local government, participatory policy, and civic organising in Porto Alegre, Brazil. Politics Soc. 1998;26:511–537. [Google Scholar]
- 59.Chaplin SE. Cities, sewers and poverty: India’s politics of sanitation. Environment and Urbanisation. 1999;11:145–158. [Google Scholar]
- 60.Wiebe RH. The Search for Order 1877–1920. New York, NY: Hill and Wang; 1967:chap 5.
- 61.Rosenkrantz BG. Public Health and the State: Changing Views in Massachusetts, 1842–1936. Cambridge, Mass: Harvard University Press; 1972.
- 62.Leavitt JW. The Healthiest City: Milwaukee and the Politics of Health Reform. Madison: University of Wisconsin Press; 1982.
- 63.Duffy J. The Sanitarians: A History of American Public Health. Urbana: University of Illinois Press; 1990.
- 64.Cain LP, Rotella EJ. Death and spending: urban mortality and municipal expenditure on sanitation. Annales de Démographie Historique. 2001:139–154.
- 65.Evans R. Death in Hamburg: Society and Politics in the Cholera Years 1830–1910. Oxford, England: Oxford University Press; 1987.
- 66.Preston SH, Van de Walle E. Urban French mortality in the nineteenth century. Popul Stud. 1978;32:275–297. [PubMed] [Google Scholar]
- 67.Condran G, Williams H, Cheney RA, The decline of mortality in Philadelphia from 1870 to 1930: the role of municipal services. In: Leavitt JW, Numbers RL, eds. Sickness and Health in America. 2nd ed. Madison: University of Wisconsin Press; 1986:422–436.
- 68.Hardy A. The Epidemic Streets: Infectious Disease and the Rise of Preventive Medicine 1856–1900. Oxford, England: Clarendon Press; 1993.
- 69.Melosi MV. The Sanitary City: Urban Infrastructure in America From Colonial Times to the Present. Baltimore, Md: Johns Hopkins University Press; 2000.
- 70.Sheard S. Profit is a dirty word: the development of public baths and wash-houses in Britain 1847–1915. Soc Hist Med. 2000;13:63–85. [DOI] [PubMed] [Google Scholar]
- 71.Bellamy C. Administering Local–Central Relations 1871–1919: The Local Government Board in Its Fiscal and Cultural Context. Manchester, England: Manchester University Press; 1988.
- 72.Anderson M. The US Bureau of the Census in the nineteenth century. Soc Hist Med. 1991;4:497–513. [DOI] [PubMed] [Google Scholar]
- 73.Teitelbaum MS, Winter JM. The Fear of Population Decline. New York, NY: Academic Press; 1985:18–30.
- 74.Hennock EP. British Social Reform and German Precedents: The Case of Social Insurance 1880–1914. Oxford, England: Clarendon Press; 1987.
- 75.Nelson MC, Rogers J. Cleaning up the cities: application of the first comprehensive public health law in Sweden. Scand J Hist. 1994;19:17–39. [Google Scholar]
- 76.Thompson WS. Population. Am J Sociol. 1929;39:959–975. [Google Scholar]
- 77.Notestein FW. Population—the long view. In: Schultz TW, ed. Food for the World. Chicago, Ill: Chicago University Press; 1945:36–57.
- 78.Notestein FW. Economic problems of population change. In: Proceedings of the Eighth International Conference of Agricultural Economists. Oxford, England: Oxford University Press; 1953:3–31.
- 79.Hodgson D. Demography as social science and policy science. Popul Dev Rev. 1983;9:1–34. [Google Scholar]
- 80.Szreter S. The idea of demographic transition: a critical intellectual history. Popul Dev Rev. 1993;19:659–701. [Google Scholar]
- 81.Greenhalgh S. The social construction of population science: an intellectual, institutional and political history of twentieth-century demography. Comp Stud Soc Hist. 1996;38:26–66. [Google Scholar]
- 82.Bynum WF. Science and the Practice of Medicine in the Nineteenth Century. Cambridge, England: Cambridge University Press; 1994.
- 83.Szreter S. Fertility, Class and Gender in Britain 1860–1940. Cambridge, England: Cambridge University Press; 1996:9–21.
- 84.Wrigley EA, Schofield RS. The Population History of England, 1541–1871. London, England: Arnold; 1981.
- 85.Bourgeois-Pichat J. The general development of the population of France since the eighteenth century. In: Glass DV, Eversley DEC, eds. Population in History: Essays in Historical Demography. London, England: Arnold; 1965:474–506.
- 86.Degler CN. At Odds: Women and the Family in America From the Revolution to the Present. Oxford, England: Oxford University Press; 1980:chap IX.
- 87.McKeown T. The Role of Medicine: Dream, Mirage, or Nemesis? London, England: Nuffield Provincial Hospitals Trust; 1976.
- 88.McKeown T. An interpretation of the decline of mortality in England and Wales during the twentieth century. Popul Stud. 1975;29:391–422. [PubMed] [Google Scholar]
- 89.McKeown T. The Modern Rise of Population. New York, NY: Academic Press; 1976.
- 90.Johansson SR. Food for thought: rhetoric and reality in modern mortality history. Hist Methods. 1994;27:101–125. [Google Scholar]
- 91.Foucault M. Madness and Civilisation. Howard R, trans. London, England: Routledge; 1971.
- 92.Foucault M. The Birth of the Clinic. London, England: Tavistock; 1973.
- 93.Preston SH. The changing relation between mortality and level of economic development. Popul Stud. 1975;34:231–248. [PubMed] [Google Scholar]
- 94.Preston SH. Mortality Patterns in National Populations: With Special Reference to Recorded Causes of Death. New York, NY: Academic Press; 1976.
- 95.Sen A. Development as Freedom. Oxford, England: Oxford University Press; 1999.
- 96.Chang H-J. Joseph Stiglitz and the World Bank: The Rebel Within. London, England: Anthem Press; 2001.
- 97.Stiglitz JE. Globalization and Its Discontents. New York, NY: Norton; 2002.
- 98.Tomes N. The Gospel of Germs: Men, Women and the Microbe in American Life. Cambridge, Mass: Harvard University Press; 1998. [PubMed]
- 99.Easterlin RA. How beneficent is the market? A look at the modern history of mortality. Eur Rev Econ Hist. 1999;3:257–294. [DOI] [PubMed] [Google Scholar]
- 100.Powles J. Healthier progress: historical perspectives on the social and economic determinants of health. In: Eckersley R, Dixon J, eds. The Social Origins of Health and Well-Being: From the Planetary to the Molecular. Melbourne, Australia: Cambridge University Press; 2001.
- 101.Evans RG, Barer ML, Marmor TR. Why Are Some People Healthy and Others Not? The Determinants of Health of Populations. New York, NY: Aldine de Gruyter; 1994:xiii.
- 102.Berkman LF, Kawachi I. A historical framework for social epidemiology. In: Berkman LF, Kawachi I, eds. Social Epidemiology. Oxford, England: Oxford University Press; 2000:3–12.
- 103.Marmot M, Wilkinson RG, eds. Social Determinants of Health. Oxford, England: Oxford University Press; 1999.
- 104.Kawachi I, Kennedy BP, Wilkinson RG. The Society and Population Health Reader: Income Inequality and Health. New York, NY: The New Press; 1999.
- 105.Leon DA, Walt G, eds. Poverty, Inequality and Health. Oxford, England: Oxford University Press; 2000.
- 106.Eckersley R, Dixon J, eds. The Social Origins of Health and Well-Being: From the Planetary to the Molecular. Melbourne, Australia: Cambridge University Press; 2001.
- 107.Farmer P. Social inequalities and emerging infectious diseases. Emerg Infect Dis. 1996;2:259–269. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 108.Beaglehole R, Bonita R. Public Health at the Crossroads: Achievements and Prospects. Cambridge, England: Cambridge University Press; 1997.
- 109.Labonte R. Healthy policy and the World Trade Organisation: a proposal for an international health presence in future world trade/investment talks Health Promot Int. 1998;13:245–256. [Google Scholar]
- 110.Breslow L. From disease prevention to health promotion. JAMA. 1999;281:1030–1033. [DOI] [PubMed] [Google Scholar]
- 111.Kunitz SJ. Globalization, states, and the health of indigenous peoples. Am J Public Health. 2000;90:1531–1539. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 112.Krieger N. Epidemiology and social sciences: towards a critical reengagement in the 21st century. Epidemiol Rev. 2000;11:155–163. [DOI] [PubMed] [Google Scholar]
- 113.Coburn D. Income inequality, social cohesion and the health status of populations: the role of neo-liberalism. Soc Sci Med. 2000;51:139–150. [DOI] [PubMed] [Google Scholar]
- 114.McMichael AJ, Beaglehole R. The changing global context of public health. Lancet. 2000;356:495–499. [DOI] [PubMed] [Google Scholar]
- 115.Baum F. Health, equity, justice and globalisation: some lessons from the People’s Health Assembly. J Epidemiol Community Health. 2001;55:613–616. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 116.Evans RG, Stoddart GL. Producing health, consuming health care. Soc Sci Med. 1990;31:1347–1363. [DOI] [PubMed] [Google Scholar]
- 117.Dasgupta P. An Inquiry Into Well-Being and Destitution. Oxford, England: Clarendon Press; 1993.
- 118.Rice T. Can markets give us the health we want? J Polit Policy Law. 1997;22:383–426. [DOI] [PubMed] [Google Scholar]
- 119.Woolcock M. Social capital and economic development: toward a theoretical synthesis and policy framework. Theory Soc. 1998;27:151–208. [Google Scholar]
- 120.Miringoff M, Miringoff M. The Social Health of the Nation: How America Is Really Doing. Oxford, England: Oxford University Press; 1999.
- 121.Keating DP, Hertzman C, eds. Developmental Health and the Wealth of Nations. New York, NY: Guldford Press; 1999.
- 122.Farmer P. Infections and Inequalities: The Modern Plagues. Berkeley: University of California Press; 1999.
- 123.Dasgupta P, Sergageldin I, eds. Social Capital: A Multifaceted Perspective. Washington, DC: World Bank; 2000.
- 124.Putnam RD. Bowling Alone: The Collapse and Revival of American Community. New York, NY: Simon and Schuster; 2000.
- 125.Wilkinson RG. Mind the Gap: Hierarchies, Health and Human Evolution. London, England: Weidenfeld and Nicholson; 2000.
- 126.Baum F. Social capital, economic capital and power: further issues for a public health agenda. J Epidemiol Community Health. 2000;54:409–410. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 127.Kickbusch I. The development of international health policies—accountability intact? Soc Sci Med. 2000;51:979–989. [DOI] [PubMed] [Google Scholar]
- 128.Dasgupta P. Human Well-Being and the Natural Environment. Oxford, England: Oxford University Press; 2001.
- 129.Bettcher D, Lee K. Globalisation and public health. J Epidemiol Community Health. 2002;56:8–17. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 130.Galbraith JK. A perfect crime: global inequality. Daedalus. 2002;131:11–25. [Google Scholar]
- 131.King G, Murray C. Rethinking human security. Polit Sci Q. 2002;116:585–610. [Google Scholar]
- 132.Laxton P. Fighting for public health: Dr Duncan and his adversaries, 1847–63. In: Sheard S, Power H, eds. Body and City: Histories of Urban Public Health. Aldershot, England: Ashgate; 2000:59–88.
- 133.Kearns G. Town hall and Whitehall: sanitary intelligence in Liverpool 1840–63. In: Sheard S, Power H, eds. Body and City: Histories of Urban Public Health. Aldershot, England: Ashgate; 2000:89–108.
- 134.Klein N. No Logo. London, England: Flamingo; 2000.
- 135.Hertz N. The Silent Takeover: Global Capitalism and the Death of Democracy. London, England: Heinemann; 2001.
- 136.Kula W. The Problems and Methods of Economic History. Szreter R, trans. Aldershot, England: Ashgate; 2001:371–372.
- 137.Samet JM, Burke TA. The Bush administration, the environment and public health: warnings from the first 100 days. Int J Epidemiol. 2001;30:658–660. [DOI] [PubMed] [Google Scholar]