

Abstract
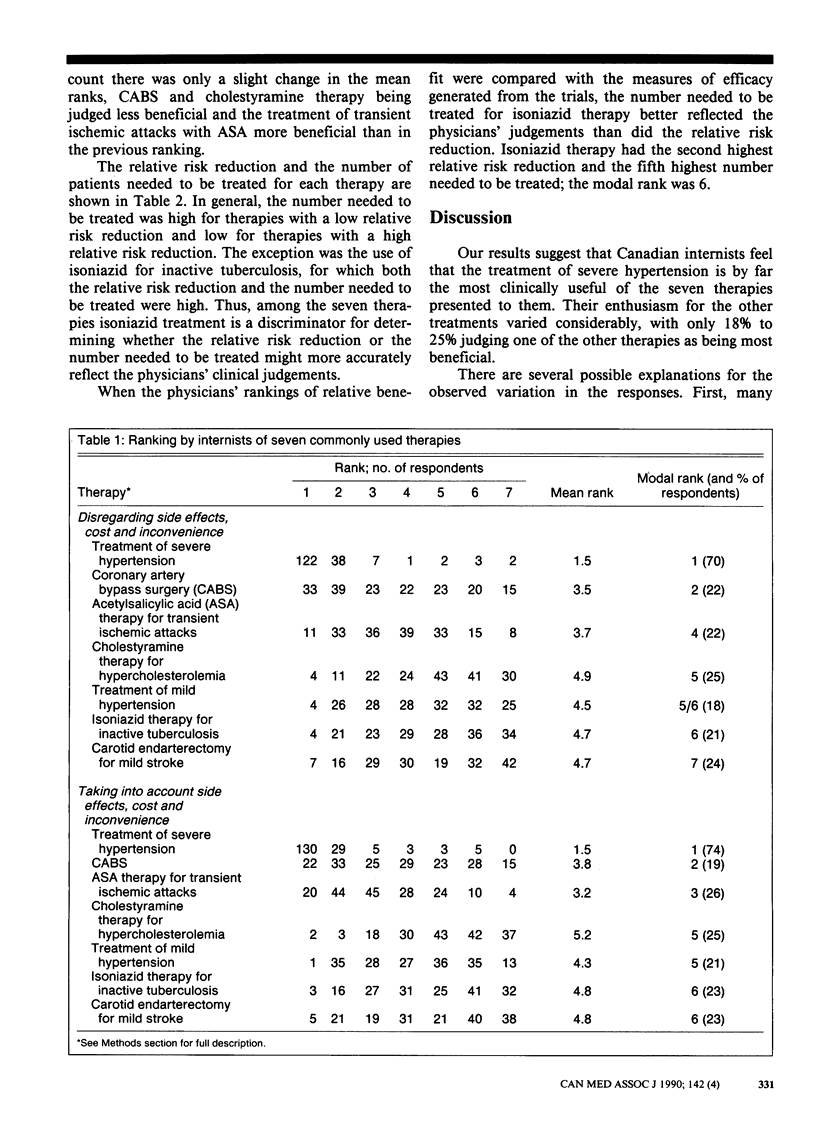
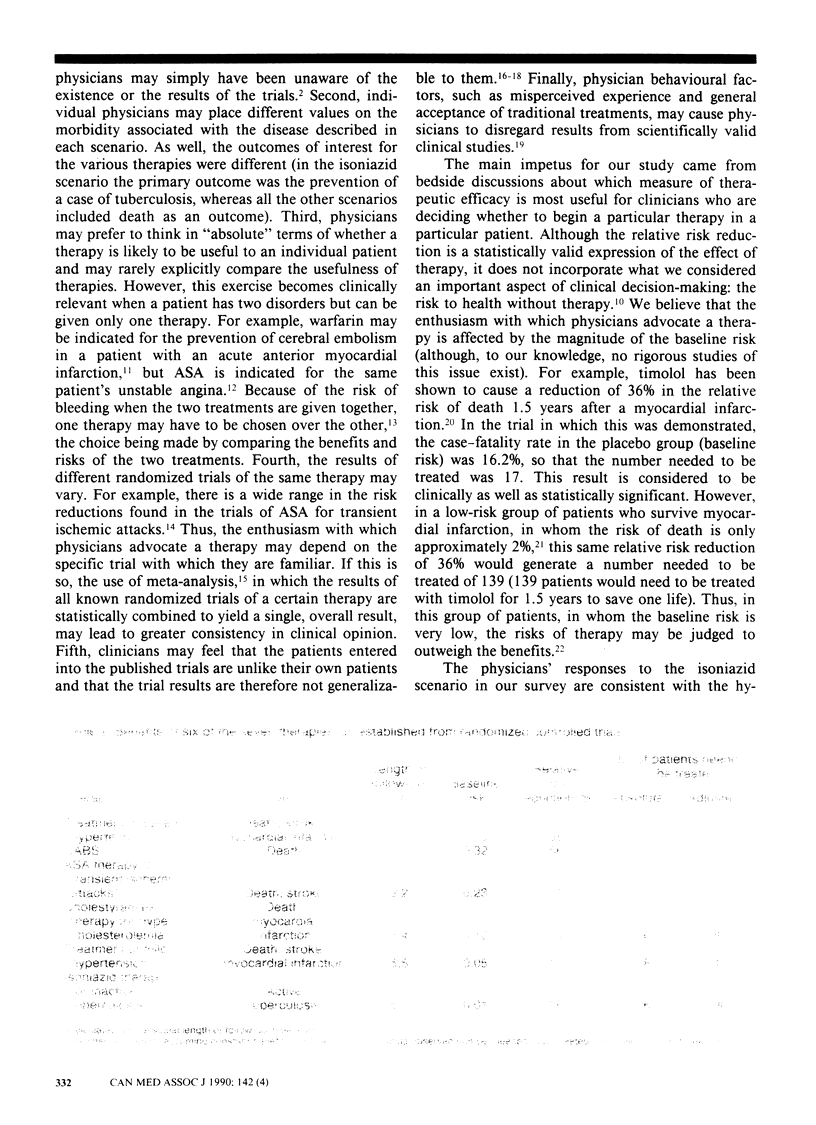
We surveyed 175 members of the Canadian Society of Internal Medicine to determine how they would rank seven commonly used treatments as to their clinical usefulness. A total of 70% of the respondents judged that the treatment of severe hypertension was the most beneficial. Coronary artery bypass surgery and treatment with acetylsalicylic acid for transient ischemic attacks were ranked next most useful. Cholestyramine therapy for hypercholesterolemia, the treatment of mild hypertension, isoniazid therapy for inactive tuberculosis and carotid endarterectomy in patients with mild stroke formed the final cluster. Except for treatment of severe hypertension there was a wide variation in the physicians' enthusiasm for the various treatments. Possible explanations for this variation include physicians' lack of awareness of the results of clinical trials, the wide range of risk reductions found in various trials of the same therapy, an unwillingness by physicians to generalize from clinical trials to individual patients, individual physicians' placement of different values on the morbidity associated with various diseases, and the fact that physicians may rarely explicitly compare the usefulness of therapies. In general, the number of patients needed to be treated to save one life better reflected the physicians' judgements than did the relative risk reduction.
Full text
PDF

Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Ahumada G. G. Identification of patients who do not require beta antagonists after myocardial infarction. Am J Med. 1984 May;76(5):900–904. doi: 10.1016/0002-9343(84)91006-4. [DOI] [PubMed] [Google Scholar]
- Cairns J. A., Gent M., Singer J., Finnie K. J., Froggatt G. M., Holder D. A., Jablonsky G., Kostuk W. J., Melendez L. J., Myers M. G. Aspirin, sulfinpyrazone, or both in unstable angina. Results of a Canadian multicenter trial. N Engl J Med. 1985 Nov 28;313(22):1369–1375. doi: 10.1056/NEJM198511283132201. [DOI] [PubMed] [Google Scholar]
- Covell D. G., Uman G. C., Manning P. R. Information needs in office practice: are they being met? Ann Intern Med. 1985 Oct;103(4):596–599. doi: 10.7326/0003-4819-103-4-596. [DOI] [PubMed] [Google Scholar]
- DeBusk R. F., Blomqvist C. G., Kouchoukos N. T., Luepker R. V., Miller H. S., Moss A. J., Pollock M. L., Reeves T. J., Selvester R. H., Stason W. B. Identification and treatment of low-risk patients after acute myocardial infarction and coronary-artery bypass graft surgery. N Engl J Med. 1986 Jan 16;314(3):161–166. doi: 10.1056/NEJM198601163140307. [DOI] [PubMed] [Google Scholar]
- Frick M. H., Elo O., Haapa K., Heinonen O. P., Heinsalmi P., Helo P., Huttunen J. K., Kaitaniemi P., Koskinen P., Manninen V. Helsinki Heart Study: primary-prevention trial with gemfibrozil in middle-aged men with dyslipidemia. Safety of treatment, changes in risk factors, and incidence of coronary heart disease. N Engl J Med. 1987 Nov 12;317(20):1237–1245. doi: 10.1056/NEJM198711123172001. [DOI] [PubMed] [Google Scholar]
- Fuster V., Halperin J. L. Left ventricular thrombi and cerebral embolism. N Engl J Med. 1989 Feb 9;320(6):392–394. doi: 10.1056/NEJM198902093200610. [DOI] [PubMed] [Google Scholar]
- Hartley R. M., Charlton J. R., Jarman B., Harris C. M. Case history questionnaires in the study of doctors' use of resources. Are they measuring what we want? Med Care. 1985 Oct;23(10):1163–1170. doi: 10.1097/00005650-198510000-00005. [DOI] [PubMed] [Google Scholar]
- L'Abbé K. A., Detsky A. S., O'Rourke K. Meta-analysis in clinical research. Ann Intern Med. 1987 Aug;107(2):224–233. doi: 10.7326/0003-4819-107-2-224. [DOI] [PubMed] [Google Scholar]
- Laupacis A., Sackett D. L., Roberts R. S. An assessment of clinically useful measures of the consequences of treatment. N Engl J Med. 1988 Jun 30;318(26):1728–1733. doi: 10.1056/NEJM198806303182605. [DOI] [PubMed] [Google Scholar]
- Resnekov L., Chediak J., Hirsh J., Lewis H. D., Jr Antithrombotic agents in coronary artery disease. Chest. 1989 Feb;95(2 Suppl):52S–72S. doi: 10.1378/chest.95.2_supplement.52s. [DOI] [PubMed] [Google Scholar]
- Sackett D. L. Rules of evidence and clinical recommendations on the use of antithrombotic agents. Chest. 1986 Feb;89(2 Suppl):2S–3S. [PubMed] [Google Scholar]
- Spodick D. H. Randomized controlled clinical trials: The behavioral case. JAMA. 1982 Apr 23;247(16):2258–2260. [PubMed] [Google Scholar]
- Stross J. K., Harlan W. R. The dissemination of new medical information. JAMA. 1979 Jun 15;241(24):2622–2624. [PubMed] [Google Scholar]
- Sundt T. M., Jr Was the international randomized trial of extracranial-intracranial arterial bypass representative of the population at risk? N Engl J Med. 1987 Mar 26;316(13):814–816. doi: 10.1056/NEJM198703263161318. [DOI] [PubMed] [Google Scholar]