

Abstract
1 Treatment of angina pectoris with β-adrenoceptor antagonists and verapamil in combination is effective and increasingly common. The study reported here was designed to show whether the pharmacokinetics of verapamil are influenced by concurrent treatment with three different β-adrenoceptor blockers, and whether there is any pharmacodynamic interaction between these drugs.
2 Twelve healthy volunteers (eight men, four women) aged 21-25 years and weighing 48-82 kg consented to participate in the study. They received verapamil 50 mg three times daily for four 1-week periods, each separated by a 1 week `washout' period. During three of the four treatment periods, the subjects took either atenolol 100 mg once daily, metoprolol 100 mg twice daily or propranolol 80 mg twice daily; in the remaining period they took verapamil alone.
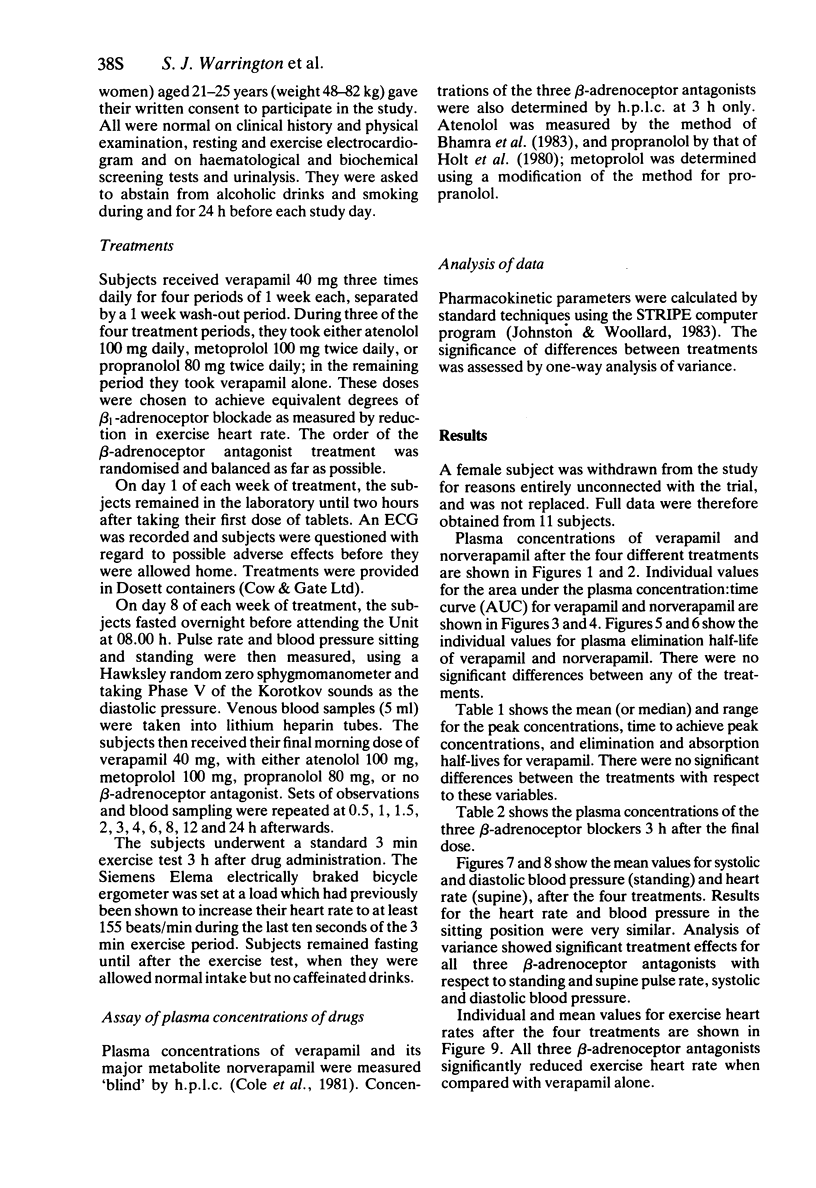
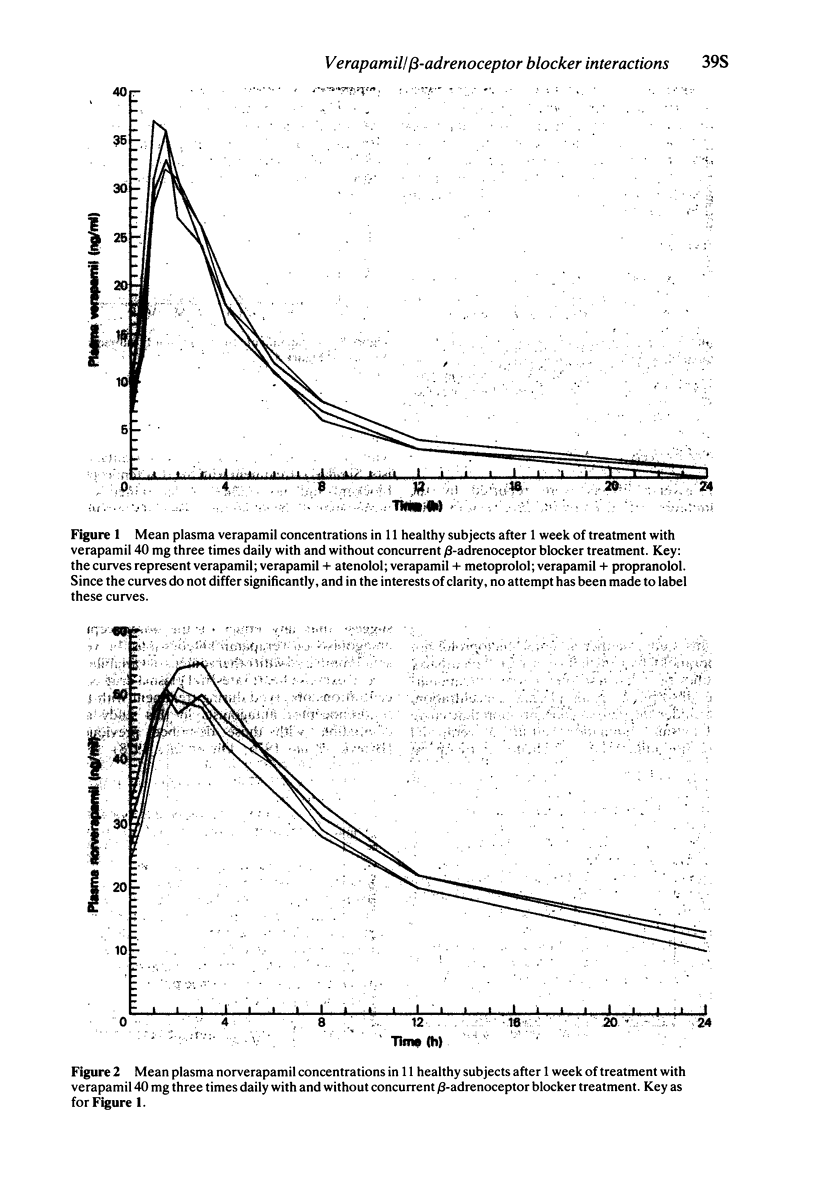
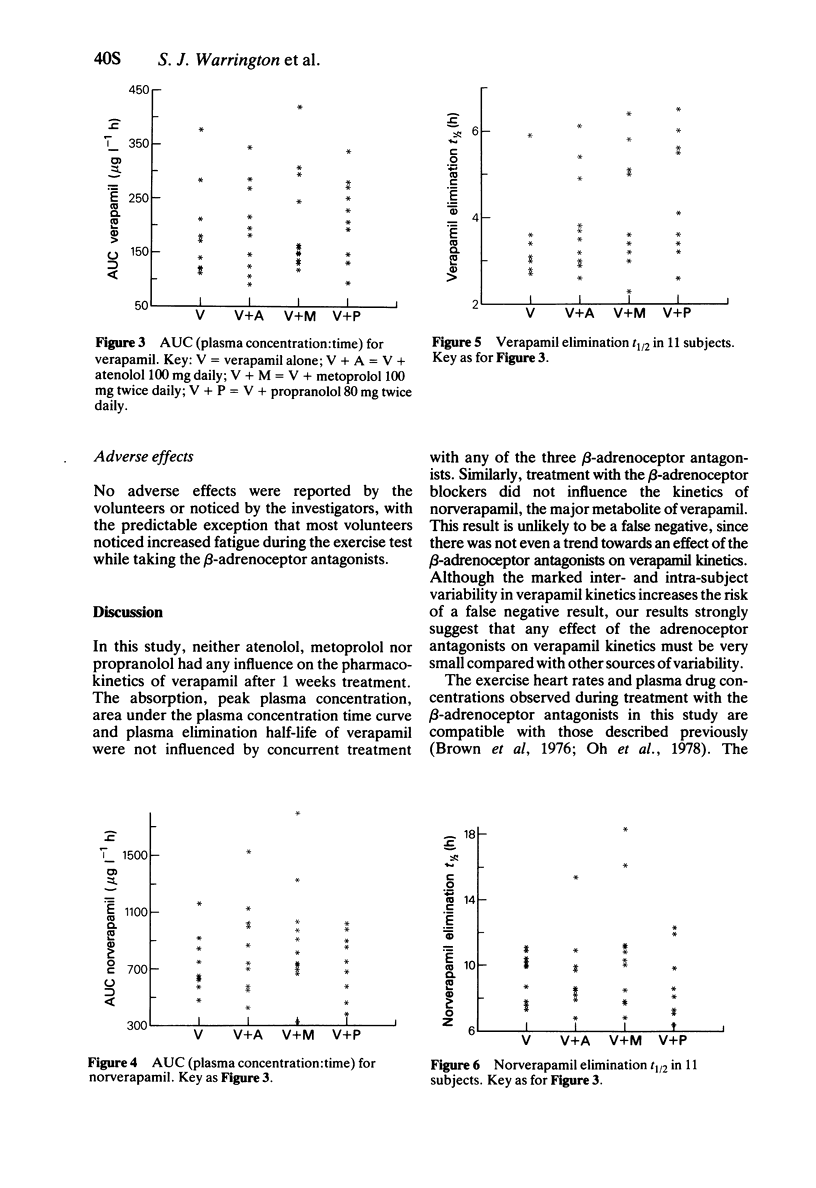
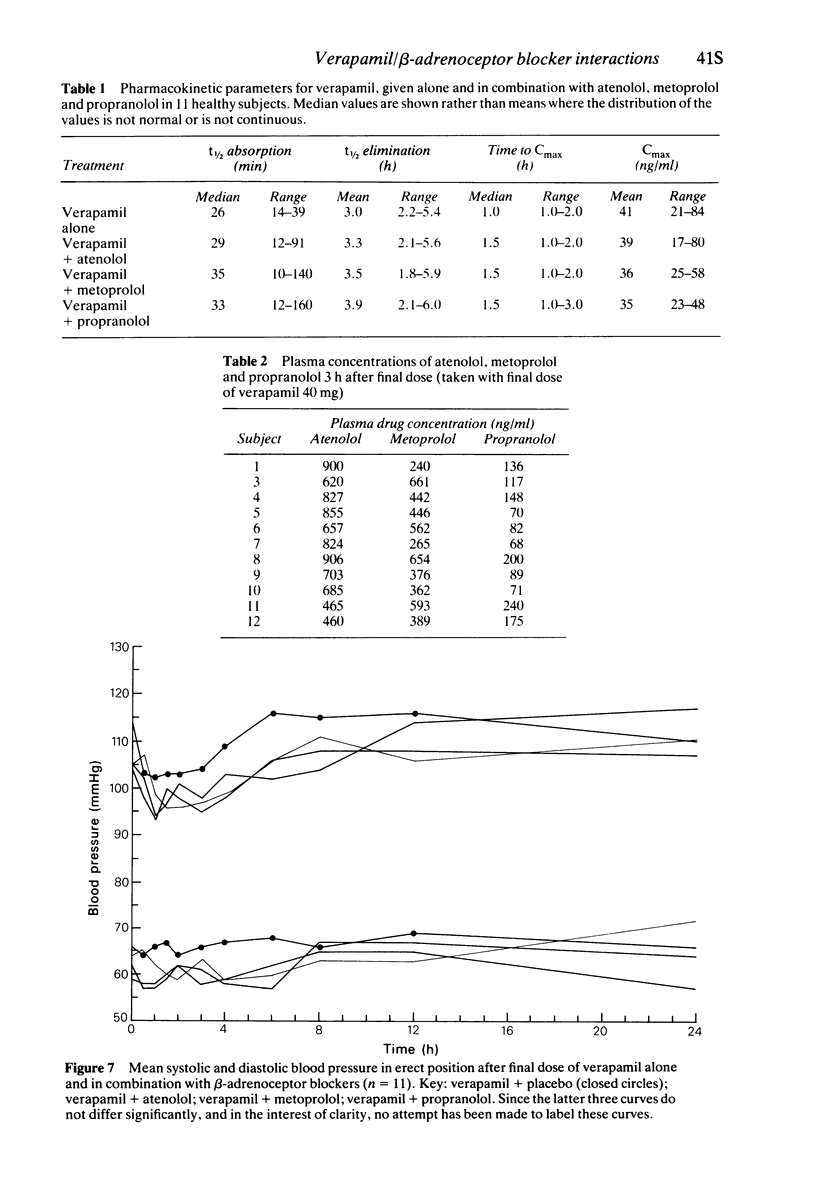
3 The concentration/time curve and plasma elimination half-life of verapamil and norverapamil, its major metabolite, were not influenced by 1 weeks co-administration atenolol, metoprolol or propranolol.
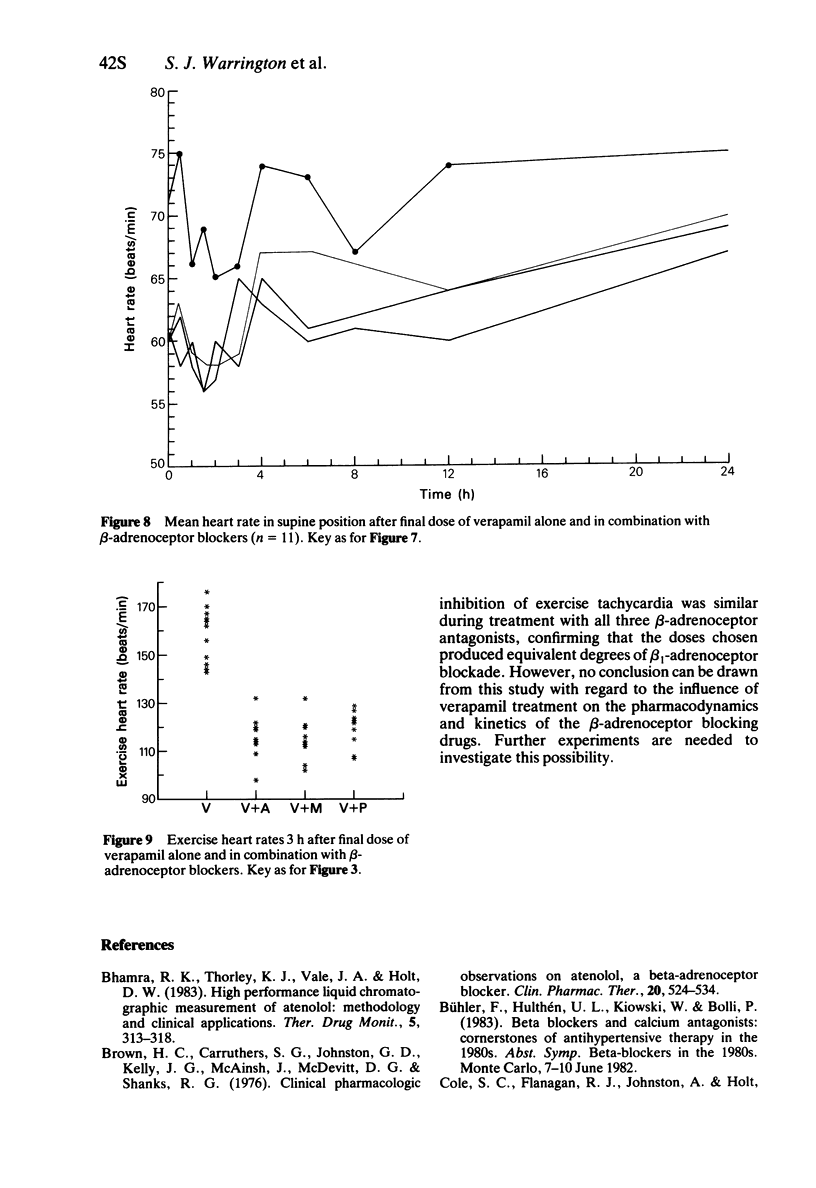
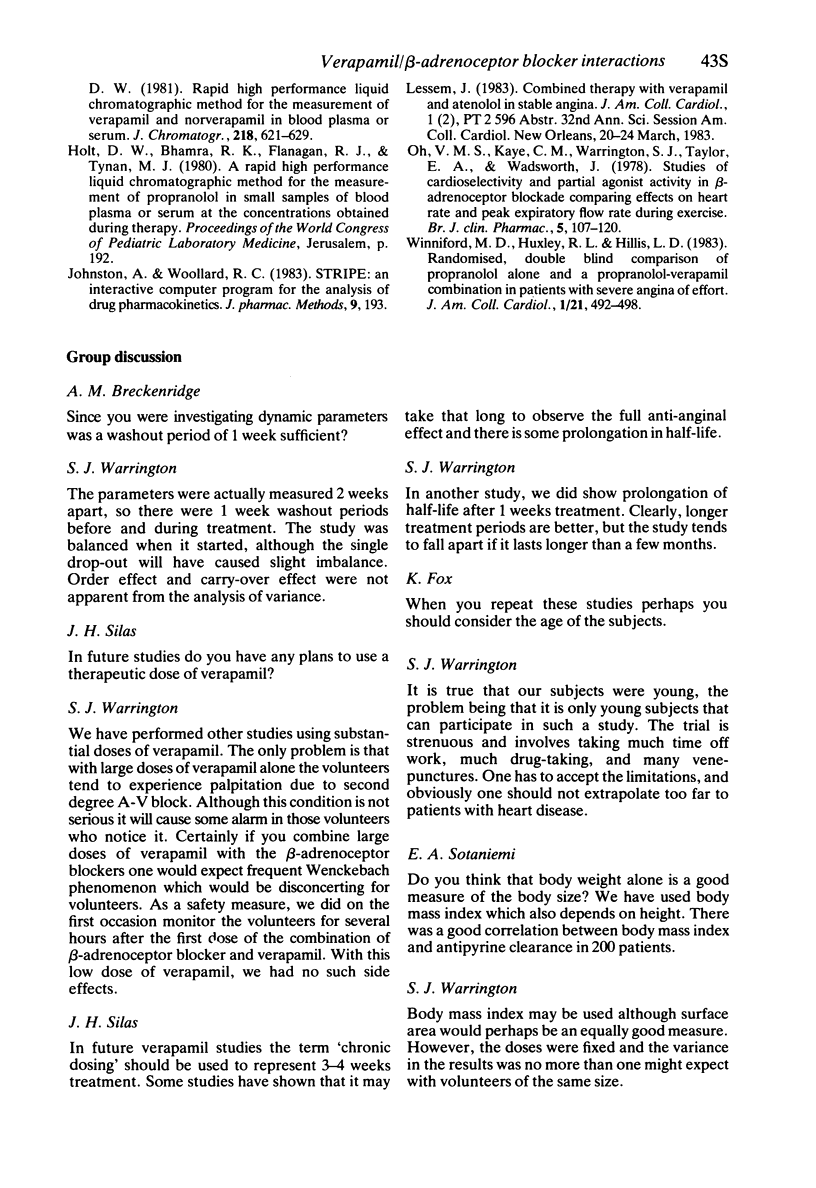
4 As expected, co-administration of each of the β-adrenoceptor blockers significantly reduced exercise heart rate when compared with verapamil alone.
Keywords: atenolol, metoprolol, pharmacology, propranolol, verapamil
Full text
PDF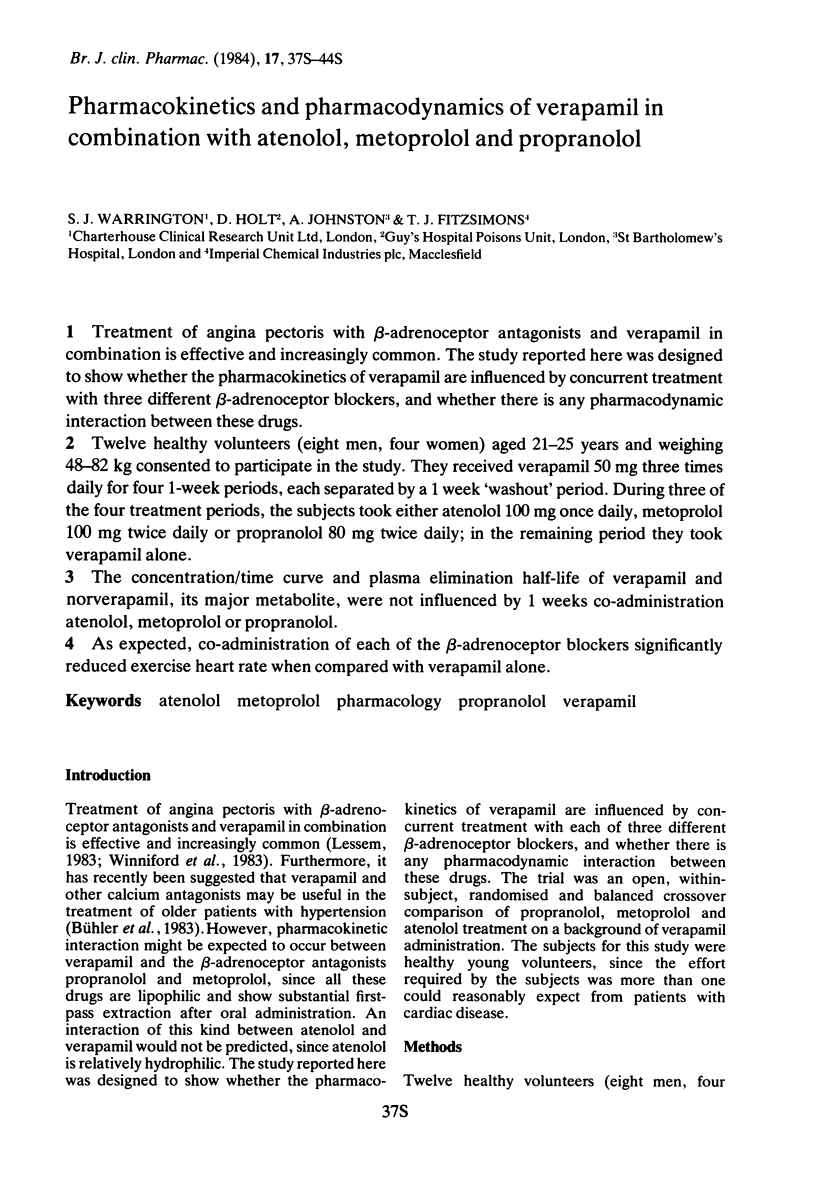
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Bhamra R. K., Thorley K. J., Vale J. A., Holt D. W. High-performance liquid chromatographic measurement of atenolol: methodology and clinical applications. Ther Drug Monit. 1983;5(3):313–318. doi: 10.1097/00007691-198309000-00012. [DOI] [PubMed] [Google Scholar]
- Brown H. C., Carruthers S. G., Johnston G. D., Kelly J. G., McAinsh J., McDevitt D. G., Shanks R. G. Clinical pharmacologic observations on atenolol, a beta-adrenoceptor blocker. Clin Pharmacol Ther. 1976 Nov;20(5):524–534. doi: 10.1002/cpt1976205524. [DOI] [PubMed] [Google Scholar]
- Johnston A., Woollard R. C. STRIPE: an interactive computer program for the analysis of drug pharmacokinetics. J Pharmacol Methods. 1983 May;9(3):193–199. doi: 10.1016/0160-5402(83)90038-4. [DOI] [PubMed] [Google Scholar]
- Oh V. M., Kaye C. M., Warrington S. J., Taylor E. A., Wadsworth J. Studies of cardioselectivity and partial agonist activity in beta-adrenoceptor blockade comparing effects on heart rate and peak expiratory flow rate during exercise. Br J Clin Pharmacol. 1978 Feb;5(2):107–120. doi: 10.1111/j.1365-2125.1978.tb01609.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Winniford M. D., Huxley R. L., Hillis L. D. Randomized, double-blind comparison of propranolol alone and a propranolol-verapamil combination in patients with severe angina of effort. J Am Coll Cardiol. 1983 Feb;1(2 Pt 1):492–498. doi: 10.1016/s0735-1097(83)80078-3. [DOI] [PubMed] [Google Scholar]