

Abstract
The importance of incorporating patient and provider decision-making processes is in the forefront of the National Institute of Mental Health (NIMH) agenda for improving mental health interventions and services. Key concepts in patient decision making are highlighted within a simplified model of patient decision making that links patient-level/“micro” variables to services-level/“macro” variables via the decision-making process that is a target for interventions. The prospective agenda for incorporating decision-making concepts in mental health research includes (a) improved measures for characterizing decision-making processes that are matched to study populations, complexity, and types of decision making; (b) testing decision aids in effectiveness research for diverse populations and clinical settings; and (c) improving the understanding and incorporation of preference concepts in enhanced intervention designs.
Keywords: decision aids, decision making, interventions, preferences
INTRODUCTION
The importance of incorporating patient and provider decision-making processes in interventions research has come to the forefront of the National Institute of Mental Health (NIMH, 1999) agenda for improving mental health interventions and services and is currently identified as a key research direction for the NIMH Primary Care Research program. Patients/healthcare users1 are increasingly recognized as key decision makers in shared treatment decision making with healthcare providers, but relatively little research has been done in mental health regarding patient/provider treatment preferences and decision-making processes. Research in this area is high priority because of individual quality of life and autonomy reasons, but also in the context of the health services research agenda to improve population health outcomes. Most patients ultimately decide for themselves what they will or will not do in regard to treatment, and this autonomy right is also increasingly recognized in community mental health and other types of health care.2 Patients' decisions impact behaviors, such as treatment initiation and continuance, which in turn can influence individual and aggregate level clinical health status and health system outcomes.
How patients make decisions, the testing of interventions to support effective decision making, and the development of measures of patient decision making have only recently begun to be studied for mental health contexts. Interest in patient decision making for mental health contexts is timely given a general increase in interest in patient-centered interventions that focus on the patient perspective in health care (van Dulmen, 2003; Lauver et al., 2002).3 Recommendations 23, 24, and 26 of the NIMH Bridging Science and Service Report consider research needs and funding of research on patient/provider decision making; for example, additional study of decision-making theory, concepts, preference assessment, and strategies for incorporating and evaluating impacts on usual clinical care. These initiatives are the mental health expression of reform challenges articulated in the Institute of Medicine report Crossing the Quality Chasm (IOM, 2001), which addresses needs for health services quality improvements that enhance patient centeredness.
To improve mental health care quality, interventions research must better incorporate the patient/healthcare user perspective—not only in terms of more traditionally studied patient-centric concepts, such as symptoms, expectations, beliefs/attitudes, and preferences—but also in terms of decision making itself, as related to the process and outcomes of care. For example, a contemporary proposal for healthcare services redesign is embodied in the Chronic Care Model (E. Wagner, 1998) that has been applied to systemwide interventions to improve depression care (Von Korff, Unutzer, Katon, & Wells, 2001). The Chronic Care Model addresses strategies to improve self-care management support via “productive interactions” among “informed, activated” patients and “prepared, proactive practice” teams. Central to the self-management support dimension of the Wagner model is basic research on what creates the “productive interactions” at the heart of the model for improving outcomes. In this article, we propose that improving patient self-management requires better understanding of productive interactions, as can occur via the study of patient/provider decision making.
Aims of This Article
The overall aim of this article is to describe how patient decision-making concepts are being incorporated in recent mental health research. Following a brief historical overview of decision theory, we describe a decision-making model (Rothert et al., 1997) with its supporting empirical findings that link patient-level/“micro” variables to services-level/“macro” variables via the decision-making process that is a target for interventions. Next, we discuss the rapid growth of patient-centered decision aids (DAs), including presentation of an example research program involving descriptive and interventions research methods focused on testing the usefulness of DA technology in mental health. Finally, we discuss further challenges and future directions for incorporating patient preferences into interventions research designs.
DECISION THEORY: HISTORICAL BACKGROUND
Decision theory has evolved since the 1950s from the fields of psychology and economics and has been applied in healthcare research since the 1960s. Theoretical perspectives in decision-making research encompass a wide variety of prescriptive and descriptive approaches; for example, judgment and information processing analysis, decision analysis, and natural decision making. In-depth reviews of key approaches are found in representative texts and articles (Cooksey, 1996; Gigerenzer & Todd, 1999; Hammond, 1996; Hastie, 2001; Hastie & Dawes, 2001; Hunink & Glasziou, 2001; Zsambok & Klein, 1997). Clinical decision-making research has been most influenced by information processing theory (Newell & Simon, 1958), social judgment theory (Juslin & Montgomery, 1999), and expected utility (EU) theory (Schoemaker, 1982), and until the early 1980s, focused almost exclusively on clinician decision making. Prescriptive approaches to decision-making research are usually based in variations of the expected utility framework (Schoemaker, 1982) in which “best” decisions emphasize maximizing expected utility for outcomes. The EU is calculated by multiplying the probability (p) of an outcome by its value/utility (u) and summing up the products for each outcome. EU theory provides a systematic approach for dealing with trade-offs amongst multiple goals occurring in opposition to each other, such as the desire to feel better weighed against possible side effects of a treatment. Descriptive approaches focus on understanding how decisions are made, including testing if utility-maximizing choices are actually made. Descriptive research highlights specific areas to target interventions to improve the decision-making process to influence choices, behavior, and outcomes, and can also reveal variables that are less modifiable via current interventions.
SIMPLIFIED DECISION-MAKING MODEL
Key concepts in this article pertaining to patient-centered interventions are examined in relation to a simplified descriptive model of patient decision making (Figure 1), adapted from Rothert et al. (1997), that has been used to guide a long-term interdisciplinary research program on patient/provider decision making at Michigan State University, including more recent research on treatment decision making of depressed primary care patients (Wills & Holmes-Rovner, 2003b). The model highlights the patient as being at the center of research to improve mental health care and how individual-level variables are related to service-level outcomes via the conceptual lens of decision making. Double-headed arrows are shown between the key concepts in the model to reflect the dynamic interrelationship over time between the concepts. For example, the double arrow between preferences and decision can reflect the effect of hindsight in the form of decisional regret on later preferences. Likewise, a double arrow between behavior and decision occurs because behavior can influence subsequent choices.
Figure 1.
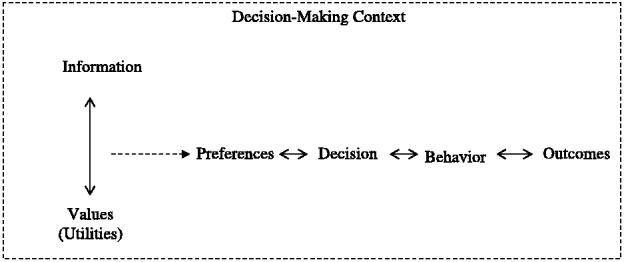
A simplified model of decision making, adapted from Rothert et al., (1997), which illustrates key concepts of relevance to patient decision making. In a given context, values and information interact to produce preferences, which in turn shape decisions, behavior, and subsequent outcomes. The double arrows between the concepts reflect the dynamic interactions among the concepts over time.
Information, Values, and Decision-Making Context
Information
Information refers to decision-relevant data inputs to decisions. For example, information can include the probabilities of risks, benefits, and lifestyle changes associated with taking a particular medication. For treatment decisions, concerns include the quality and accessibility of needed information. Information for patient decision making varies widely in its quality and comprehensibility (Wills & Holmes-Rovner, 2003a) and must be adequately accessible to patients to be useful for decision making (Feldman-Stewart, Brundage, McConnell, & Mackillop, 2000). Treatment and health condition information found in pamphlets and booklets available in clinics has often been found to be less than complete (Coulter, Entwistle, & Gilbert, 1999; Godolphin, Towle, & McKendry, 2001), as assessed by standardized instruments on information quality (Charnock, Shepperd, Needham, & Gann, 1999).4 Patients increasingly rely on the Internet for health information, and much of the “treatment” of mental health conditions such as depression takes place on the basis of self-help information and informal sources of care (Gask & Rogers, 1998). However, Internet-based information on depression has been found to yield still generally poor-quality information (Griffiths & Christenson, 2000; Lissman & Boehnlein, 2001). Proposed minimal elements sufficient for treatment decision making include treatment options, treatment descriptions, possible outcomes and their likelihoods, risks and side effects of treatments, and relevant conflict of interest issues in research-based information (Holmes-Rovner & Wills, 2002). Computer information technology could be used to provide these aspects of information for decision making via “patient choice modules” (Holmes-Rovner et al., 2001).
Values (Utilities)
Values reflect the importance that people place on information for decision making, as well as on various aspects of their experience and other factors in the broader context of their decision making. In formal decision theory, quantitative estimates of values are derived that represent attractiveness of health states in the context of negative aspects of treatments. For example, depressed patients often place high importance (value) on feeling better, but also value avoiding adverse treatment side effects. The relative strength of these values can significantly impact patient preferences for treatment options, subsequently affecting the choices that patients make about treatments. Values may be particularly interesting to study in mental health research, because issues such as depression often involve existential aspects that can benefit from personal values clarification. Values have rarely been directly measured in mental health research. An exception is the work of Cooper et al. (2000), who developed a measure based on eliciting patients' opinions of the importance of various aspects of depression care.
Decision-Making Context
The decision-making context concerns influences on decision making from the broader context of an individual's life, which may sometimes be powerful influences on the choices that patients make. Context includes various aspects of a person's day-to-day life and functioning, the healthcare system structure and process, and the broader sociocultural milieu that shapes people's experiences. For example, patients take into account, both mindfully and less deliberatively, a host of contextual factors in evaluating treatment options, such as the severity of condition, lifestyle impact of treatments, and key barriers to particular options such as the social stigma associated with seeking professional mental health services (Cooper-Patrick et al., 1997; Link, Struening, Neese-Todd, Asmussen, & Phelan, 2001; Rost, Smith, & Taylor, 1993; Wills, 1997). For mental health, social stigma is a key contextual variable affecting what patients do about seeking help for mental health problems (Sirey et al., 2001), as are cultural variables and other access barriers to mental health care such as lack of insurance and poorly structured systems of care (Mental Health: A Report of the Surgeon General, 1999). Roeloffs et al. (2003), for example, found a high frequency of stigma concerns in depressed primary care patients that was related to a variety of other contextual variables, such as chronic medical conditions and social support. Race differences in depression symptoms, such as higher rates of depression symptoms in Black people compared to White people, have been hypothesized to be related to differences in exposure to stress and vulnerability to stressors, as a function of life context (George & Lynch, 2003; Schulz et al., 2000). The study of contextual factors also links decision making to broader models of health behavior and adherence, in which noncognitive factors are modeled as behavioral influences.
Preferences
Preferences, representing a relatively greater liking of one alternative as compared to (an) other alternative(s), recently have begun to be studied in mental health research. As shown in Figure 1, preferences are the product of the interaction between decision-related information and values (utilities). Thus, information and values are key inputs to preferences, which, in turn, within a given decision-making context, shape decisions (choices). There is an extensive body of theoretical literature on preference assessment in psychology and medical decision making that recently has begun to be applied in mental health research. Theoretical debates have focused on the extent to which preferences are “revealed” versus “constructed” during the elicitation process (for alternative views on this debate, see Dowie, 2002; Payne, Bettman, & Johnson, 1992), as well as which elicitation methods to use. Different methods of assessing preferences often yield different results. Research on individual preferences also often reveals differences in how people of varying characteristics and in different contexts approach health-related decisions.
Although basic research on preferences in laboratory settings has yielded important theoretical insights about the nature of preferences, this research has been critiqued on its lack of generalizability to research and clinical practice in “real-world” settings. There is no one fully agreed-upon way to measure a preference. In mental health interventions and services research, some published reports of studies of preference assessments have begun to appear, most often based on rating scale measures. Preferences assessments have been done within mental health treatment needs assessments, as well as in interventions studies in order to guide selection of treatment options. For example, Alvidrez and Azocar (1999) surveyed psychologically distressed women at public gynecology clinics about their preferences for and barriers to use of psychologic services. Most women were interested in services, especially individual counseling and psychoeducational classes, but they reported substantial barriers to accessing preferred services. In a telephone survey, Cooper et al. (2003) assessed preferences for treatment of depression of depressed White people, Hispanics, and Black people. Both Black and Hispanic study participants preferred antidepressant medication less compared to White participants, and the study also highlighted the importance of understanding the social and cultural context in which treatment decisions are made. Dwight-Johnson, Unutzer, Sherbourne, Tang, and Wells (2001) found that a primary care depression quality improvement intervention that incorporated patients' preferred treatment choices increased the likelihood that patients would enter treatment and receive their preferred treatment. Dwight-Johnson, Sherbourne, Liao, and Wells (2000) also found that most depressed primary care patients wanted depression treatment, especially counseling, but that preferences varied by gender, income, treatment knowledge, and ethnicity. Patients who preferred treatment were more affluent, knowledgeable about medication, and Black people more strongly preferred counseling compared to White people. Patients in the intervention condition were more likely to receive their preferred treatments, but regardless of study condition, fewer than 50% of patients who preferred counseling reported that they received it. Finally, some research has examined the relationship between preferences and health status. For example, Sherbourne, Sturm, and Wells (1999) found that patient preferences were almost as strongly related to their mental and social health as their physical health.
Decisions and the Decision-Making Process
Decisions
As shown in Figure 1, decisions are choices that are shaped by preferences, and preferences in turn shape patient behaviors. The behavioral implementation of choices in the form of treatment adherence has most often been studied in relation to mental health interventions. For example, Mojtabai, Olfson, and Mechamic (2002) found that perceived need and help seeking (defined as any voluntary contact with health professionals) were associated, among adults with commonly occurring primary care mental health problems who were included in the National Comorbidity Survey. Decisions have often been inferred retrospectively on the basis of behaviors, but behavior is influenced to varying degrees by mindful decision making.
Decision-Making Process
The decision-making process refers to how information and values are combined to form preferences and to arrive at decisions. To better understand the linkages between patient characteristics and outcomes, there is a need to examine key elements of the decision-making process itself. The decision-making process itself can also be the focus of testing patient-centered interventions to improve decision making and subsequent choices and outcomes (A. M. O'Connor, Fiset et al., 1999; Rothert et al., 1997). The process of how patients make decisions has rarely been studied in mental health research until recently.
Currently there are significant conceptual and methodologic challenges concerning the measurement of patient decision-making processes in mental health. Key concepts and measurement approaches developed in psychology, economics, and medicine do not always carry over well to the mental health interventions, populations, and settings. For example, the concept of “decision making” may or may not be relevant for various populations experiencing mental health problems, such as patients who have often experienced involuntary mental health treatment for acute psychosis (Pescosolido, Brooks Gardner, & Lubell, 1998), or patient populations for whom personal control of choices is not perceived as reality. Highly quantitative approaches to modeling decisions via techniques, such as formal decision analysis, have been applied with success in some areas of medicine, such as decision making about high-risk acute treatments. In decision making about chronic disease management in nonacute care settings with diverse populations, however, these same approaches have been criticized for being overly cognitive and decontextualized. For example, decision analytic models have often focused on one-time treatment choices, such as surgery, which do not necessarily take into account key factors such as patient lifestyle and culture. Other criticisms of basic science approaches to the study of decision making include the lack of generalizability of results from the use of healthy volunteer samples to study health-related decision making with hypothetical scenarios/vignettes. Clinical decision-making research now routinely incorporates multiple methods going beyond the laboratory setting, which is also consistent with calls to study mental health phenomena and interventions under lessthan-controlled real-world conditions (Hohmann & Shear, 2002).
Outcomes
Outcomes are, in part, the end result of patient behavior and can be considered at both the individual and system levels. Examples include individual and population health status and costs of health care. For example, mental health interventions researchers have most often studied the mental health status of patients, such as improvement in depression attributable to an intervention. Likewise, services researchers have studied structural aspects of health care that can impact and be influenced by the decision making of patients, such as insurance coverage for mental health care influencing decision making, and patient decision making influencing costs of care. In addition, services researchers have studied population-based outcomes, such as morbidity and mortality from inadequately treated depression. Outcomes such as these represent the “ultimate” end results of care, but have yet to be studied in relation to the mental treatment decision-making process itself.
AIDING DECISION MAKING: PATIENT-CENTERED DECISION AIDS/INTERVENTIONS
Background
Patient-centered DAs are an emerging area of interventions research that incorporates decision-making concepts. DAs are interventions to help people make deliberative, effective choices about health treatment options (including maintaining a status quo position) for complex decisions (A. M. O'Connor, Drake et al., 1999). DAs have been developed in a variety of formats, such as booklets, interactive group discussions, decision boards, interactive videodiscs, audiotapes, audio-guided workbooks, and interactive computer-based support guides. Patients may use DAs for a variety of initial and continuance decisions regarding discrete health interventions (screening and treatment). The timing and length of engagement with a DA varies depending on the content of the DA, but is intended to be feasible for a given patient or patient population. The largest growth in DAs is in regard to computer-based formats. DAs are tools for more actively engaging patients in shared treatment decision making. Thus, DAs have been differentiated from passive education materials, such as booklets about health conditions and their treatment, generic education that does not focus on a specific decision, or which are intended to promote compliance with a recommendation instead of a supporting choice based on personal values (Deyo, 2001; Fagerlin et al., 2004; A. M. O'Connor, Drake et al., 1999).
The overall intent of DAs is to assist in the “translation task” of helping patients to make evidence-based decisions (A. O'Connor, 2001), but DAs are intended to enhance and not replace or fix all problems with usual care. Effective decision-making criteria include the decision being adequately informed, consistent with personal values, behaviorally implemented, and associated with favorable outcomes such as patient satisfaction (A. M. O'Connor, Drake et al., 1999). The distal goals of effective decision making include improving individual and health system outcomes. DAs are primarily intended as enhancements to formal counseling approaches, such as cognitive behavioral (CBT) and problem-solving therapy (PST) approaches. By contrast to the cognitive restructuring and problem-managing skills foci of CBT and PST (Nezu, 2004; Nezu, D'Zurilla, Zwick, & Nezu, 2004), DAs focus on improving the quality of treatment decision making. To the extent that patient preferences are incorporated and informed by the best available evidence about treatment options, patient outcomes may be improved.
To date, DAs have been developed and tested for a wide variety of complex health screening and treatment decisions, which often have represented “one-time” decisions (see Cochrane Inventory of Existing Patient Decision Aids Identified Using Cochrane Review Methods, available online at http://decisionaid.ohri.ca/cochinvent.php; Stacey & O'Connor, 2004). As of early 2004, the Cochrane Inventory included 481 DAs, with 316 currently verified via the Cochrane definition of a DA (see CREDIBLE Criteria at http://decisionaid.ohri.ca/cred.html). Currently, there are no widely accepted minimal standards for what constitutes a DA, but an international consensus on standards for developing and evaluating patient decision aids (IPDAS) has developed inclusion and exclusion criteria that were voted upon in 2005 by a diverse set of stakeholders (see http://ipdas.ohri.ca/ for additional information). The current criteria for key DA elements include information about options, presentation of probabilities of outcomes, values clarification, use of patient stories/testimonials, guidance/coaching, disclosure of conflicts of interest, balanced information, use of plain language, use of current scientific information, and assessment of decision quality and effectiveness (IPDAS, 2005).
DAs may be keys to better interventions, either at the individual or the systems level, but given the newness of the field, there are limited data so far explaining how DAs work (Bekker, Hewison, & Thornton, 2003). Limited information exists currently about the overall value of patient health informatics tools, including DAs (Agency for Health Care Research and Policy, 1998). Recent research has shown that DAs can increase knowledge, reduce intrapersonal conflict in decision making, foster more active participation among patients in making health-related decisions, have little impact on patient satisfaction, and have variable effects on the specific decision made (A. M. O'Connor, Rostom et al., 1999). DAs may also increase consistency with decision analytic models (Holmes-Rovner et al., 1999) and enhance the likelihood of choices being based on realistic information and expectations about outcomes (A. M. O'Connor, Fiset et al., 1999).
Prospects and Challenges for Improving Usual Mental Health Care
DAs are essentially a healthcare reform proposal for empowering patients to make more effective health treatment decisions. They are a potential means of achieving goals of health services reform (such as the Chronic Care Model) regarding supporting, informing, and activating patients. In this context, interest is currently high, related to the potential for improving care as usual, that is, targeted improvements in information quality, specific strategies to improve the patient/provider interaction, values clarification exercise, and other strategies for empowerment regarding health system access issues that are currently not often well addressed in usual care. However, with the exception of a DA regarding depression medication decision making from Healthwise Incorporated (www.healthwise.org), no publicly available DAs currently exist for mental health topics, although this situation is changing. The first and second International Shared Decision Making conferences (representing leading groups working on DAs and shared decision-making approaches for health care) took place in Oxford, England (July 2001) and Swansea, Wales (August 2003). The 2003 conference included a “Decision Making in Mental Health Care” article session with five presentations of research on mental health topics, regarding depressed primary care patient treatment decision making (Bunn, Jacobsen, Whitelaw, McIntosh, & Fox, 2003; Loh, Giersdorf, Simon, & Harter, 2003; Simon, Loh, Giersdorf, & Harter, 2003; Wills, 2003a) and schizophrenia treatment decision making (Harmann & Kissling, 2003). Results of research were reported within plans to develop patient-centered DAs/interventions for these mental health treatment contexts.
Shared Decision Making and Patient-Centered DAs
DAs may be best incorporated in a shared decision-making process that is strongly patient centered, involving a philosophy of providing information for specific decisions that puts the patient's objectives first (Bridson, Hammond, Leach, & Chester, 2003; Charles, Gafni, & Whelan, 1997; Charles, Whelan, & Gafni, 1999). Understanding the patient and the patient's priorities via effective communication is central to high-quality mental and other health care (Cruz & Pincus, 2002; Gask, 1997; D. Roter, 2000), especially for preference-driven treatment decisions (Barry, 1999). For mental health clinicians, patient centeredness has always been important to mental health intervention, but not necessarily the philosophy of more active patient involvement, as envisioned in the current shared treatment decision-making literature. Shared decision making holds the prospect of better matching of treatments to patients, improved patient satisfaction, and improved outcomes of care (Trede & Higgs, 2003).
Patient Involvement in Shared Decision Making
In the mental health interventions research literature, shared decision making is starting to be incorporated to enhance patient involvement in care. “Empowering” or “activating” patients in usual care settings has been identified as a key strategy for reducing barriers to depression care (Von Korff, Katon, Unutzer, Wells, & Wagner, 2001). For example, in a randomized clinical trial of a primary care–based intervention for prevention of depression relapse, Ludman and colleagues tested an approach to providing depression education and shared decision making about use of pharmacotherapy and cognitive behavioral strategies designed to enhance patient self-management of depression care (Ludman et al., 2003). The results showed a statistically significant improvement for the intervention group patients for self-efficacy, tracking of depression symptoms and early warning signs, and planning for coping with high-risk situations. Likewise, Bleyen, Vertommen, and Van Audenhove (1998) found a “treatment negotiation approach” was associated with a significant positive impact on treatment dropout rates for the intervention group compared to a control group.
Techniques such as motivational interviewing have been proposed as ways to foster patient involvement in decision making and behavior change (Britt, Hudson, & Blampied, 2004). The extent of decision-making involvement that is necessary to a shared decision-making process is currently debated, however. For example, Van Audenhove and Vertommen (2000) recently proposed that the psychotherapeutic intake strategy involves four key elements: exploring the client's perspective (with explicit attention to the client's preferences), information exchange, negotiation, and the client ultimately making a choice between proposed treatment alternatives. In some instances, however, especially for “high-stakes” decisions, patients want more information but not to necessarily be responsible for making treatment decisions (Deber, Kraetschmer, & Irvine, 1996). There is currently a lack of research-based information about the psychologic impact of patient participation in making complex and stressful decisions (Pierce & Hicks, 2001).
It has been argued that the enhancement of patient involvement in decision making must be in appropriate balance with clinicians' being able to make recommendations or provide guidance to patients (Ubel, 2002). It is unclear if DAs increase anxiety or other psychologic distress in some situations, and additional research is needed to understand conflicting study reports. For example, it has been found that some palliative cancer patients may have a preference for avoiding information about prognosis and deferring decision making to key others (de Haes & Koedoot, 2003). In a clinical trial of a DA for counseling about the prenatal diagnosis for Down's syndrome, it was found that a DA elicited greater expression of negative affect (Bekker, Hewison, Thornton, 2003). However, Bekker Legare, Stacey, O'Connor, and Lemyre (2003), in a systematic review of literature on anxiety measures to assess DA effectiveness represented in 10 randomized controlled trials, found mixed results regarding anxiety: anxiety was not greater based on exposure to DAs, but varied with the characteristics of the decision. Decisions involving invasive screening or treatment were associated with higher anxiety, and women had higher anxiety scores than men. In a systematic review of the effects of patient DAs, O'Connor, Rostom et al. (1999) found that use of DAs did not increase patient anxiety, and Kennedy, Robinson, and Rogers (2003), in a test of a DA with patients with ulcerative colitis, also found that anxiety did not increase in response to the intervention.
Effective patient-clinician communication is at the heart of shared decision making, but the research literature on communication during patient-provider exchanges about health care is limited in regard to the study of the patient perspective and contextual factors that impact the quality of the interaction with the health care provider (D. L. Roter, 2003). Patient perceptions of participation and communication with clinicians have been found to be associated with patient characteristics and treatment behavior. For example, Cooper-Patrick et al. (1999) operationalized participation via patient ratings on the physician participatory decision-making (PDM) style scale (Kaplan, Gandek, Greenfield, Rogers, & Ware, 1995) and found that Black patients related their visits as less participatory compared to White patients. In a recent review of interventions focused on improving patient communication with physicians, Harrington, Noble, and Newman (2004) found that outcomes that were improved by the interventions included perceived health control, adherence, appointment keeping, clinical outcomes, recall of information, and preferences for more active involvement in own health care.
Information Technology Potential
Information technology enhancements, such as the availability of computer support groups for various health issues, have good potential for improving access to interpersonal support and improving patient empowerment related to treatment decision making (Masi, Suarez-Balcazar, Cassey, Kinney, & Piotrowski, 2003) and can be accessed outside of the time-limited healthcare visit. An increasing number of primary care patients do use the Internet to obtain health information to inform their decision making (Diaz et al., 2002; T. Wagner & Hibbard, 2001). Many DAs are available online, and mental health interventions are also being tested in online formats (Christensen, Griffiths, & Jorm, 2004). The full potential of computerized decision support systems for primary care settings (for patients and healthcare providers alike) has yet to be realized (Delaney, Fitzmaurice, Riaz, & Hobbs, 1999), and there is limited information about the effects of Internet interventions for various health promotion and rehabilitation issues, based on poor methodologic quality of reported studies (Bessell et al., 2002). Privacy issues in context of social stigma of mental illness may deter many patients from achieving the benefits that potentially could be gained from Internet-based interventions (Wright & Bell, 2003), and there are incompletely resolved ethical concerns about the use of Internet-based interventions in mental health, such as informed consent and safety issues (NIMH, 2000), and uncertain uptake and outcomes for high-need target populations (NIMH, 2003).
Research Example: Aiding Patient Decision Making About Depression Treatment
Research examples of decision-aiding approaches for mental health treatment contexts are only recently receiving research attention. As part of a Mentored Clinical Scientist Career Development (K08) Award (MH01721), the first author of this article has begun a program of research focused on aiding decision making of depressed primary care patients about depression treatment. This pilot interventions research builds upon an existing long-term interdisciplinary research program at Michigan State University on patient/provider decision making for various treatment contexts. Several sequentially related projects have been constructed to build a descriptive base of research toward the design and testing of a decision-aiding intervention for depressed primary care patients making choices about depression treatment. The goal of this research program is to develop new knowledge about how to achieve optimal shared decision making of patients and providers for depression and other types of mental health treatment. In addition, methodologic innovations developed for assessing and informing patient preferences and approaches to shared decision making have the potential to enhance other types of mental health interventions research designs.
Project #1: Preliminary Validation of Standardized Decision-Making Measures
With one exception (Bunn & O'Connor, 1996), no published evaluations of standardized decision-making measures for the mental health context had been reported prior to the start of this research program that were deemed appropriate for use in the planned research projects. Therefore, an initial study was undertaken with 97 depressed adult-age primary care patients who reported making a new, at least initial, decision about use of antidepressant medication, as suggested or prescribed by their primary care providers who were not mental health specialists. The goal of the study was to do a preliminary validation of standardized decision-making measures to be used in Project #2. Standardized decision-making measures adapted for the depression treatment context included the Satisfaction With Decision (SWD) scale (Holmes-Rovner et al., 1996), Decisional Conflict Scale (DCS) (A. M. O'Connor, 1995), and an investigator-developed scale regarding knowledge about depression and its treatment. Satisfactory psychometric properties were established for the scales (see Wills & Holmes-Rover, 2003b for additional details).
Project #2: Population-Based Needs Assessment of Patient Preferences and Decision Support Needs
Building on the results of Project #1, the aim of this project was to describe patient decision-making needs and preferences for depression treatment choices, in relation to a comprehensive health profile of a selected patient population. The initial phase of the study included in-depth semistructured telephone interviews and administrative claims audit data collection with 133 depressed patients enrolled in a large HMO in an urban area of Michigan. The results from this comprehensive profile of depressed patients recruited from a population-based sampling approach revealed a variety of specific needs and preferences for decision support (Wills, 2003b, 2004), which were used to inform the design of Project #3.
Project #3: Design and Feasibility Testing of a Patient-Centered Decision Support Intervention for Choices about Depression Treatment (in Process)
The aim of Project #3 is to use the results of the initial research projects to inform the design and feasibility-testing approach for a patient-centered decision support intervention. Based on patient preferences and needs expressed in Project #2, the initial feasibility testing is being done based on a telephone support and coaching intervention, augmented by a patient decision support booklet for making choices about depression treatment. The booklet formats include print and web-based versions, drafted in consultation with clinicians, researchers with expertise in DAs, literacy experts, and web graphics design experts. To maximize the range of patient views, feedback on the intervention will be sought from a diverse population of depressed patients, both with and without prior experience making decisions about depression treatment. Adjustments will be made to the intervention based on feedback obtained from all stakeholders involved in the research. The next step will be a randomized trial of the decision support intervention to test the efficacy of the intervention for increasing the likelihood of effective decision making and improved depression treatment outcomes.
BROADER CHALLENGES AND FUTURE DIRECTIONS
Additional Challenges for the Design and Implementation of DAs
In addition to the newness of decision-aiding research in mental health contexts, some general challenges remain for designing and implementing DAs. Feldman-Stewart and Brundage summarized these challenges as clustering into several key areas: (a) defining the content of the DA, (b) formatting the information presentation, (c) incorporating the DA into “usual” decision making and health-care processes, and (d) evaluating the effects of the DAs (2004).
Content
What information on which options to present in DAs is controversial. In mental health, although cognitive behavioral therapy and antidepressant medication are well-examined professional therapies for treatment of major depression, many patients may not find these options acceptable or may, initially or later or both, prefer other options over the professionally recommended interventions. For minor depression, for example, patients have a “rational” choice among treatment options and medication may reasonably not be a first-choice option (Ackermann & Williams, 2002; Chilvers et al., 2001). Unutzer et al. (2000) found that individuals with depression and panic disorder used alternative treatments more often compared to those without these disorders, in a national survey of use of complementary and alternative medicine. Black and Hispanic primary care patients have been found to find antidepressant medication less acceptable compared to White people (L. A. Cooper et al., 2003). Therefore, it is important that DAs address not only the interventions that are supported by the most evidence, but also provide patients with information and support for evaluating alternative and complementary approaches that may be preferred but which lack a strong base of empirical support (Barrett, Kiefer, & Rabago, 1999). The need of patients to have information about treatment options they think they prefer is an important aspect of the treatment counseling and decision-support process. The overall goal of a DA is to present balanced information about what is and is not known about the treatment options, such that patient preferences are adequately informed.
Formatting
Much research remains to be done on how to best present the content of DAs. Aside from the general content standards that have been proposed for informed decisions (Holmes-Rovner & Wills, 2002), presentations must be appropriately tailored to the needs and preferences of specific patients and populations.
Interface with Usual Care
There is currently limited information on how patients and healthcare providers perceive shared decision making in practice (Davis et al., 2003). Some key issues in need of additional research include cost, availability, complexity, time, and selective appropriateness issues (Graham et al., 2003). Knowledge, skills, and values of clinicians and patients regarding shared decision making also need additional study (Say & Thomson, 2003; Sepucha & Mulley, 2003; Stevenson, 2003; Towle & Godolphin, 1999). This is the most challenging area in which individual interventions must be tested in specific systems contexts, complicating the design of efficacy trials.
Evaluation
There is a need to develop standardized measures for evaluating the effects of patient-centered decision support interventions or aids (A. M. O'Connor, 1999). In addition, the linkage of decision-making variables with clinical and other outcomes remains a largely unresearched area, but one which could foster the more meaningful linkage of interventions and services research agendas. The largest publicly available free-of-charge set of health decision evaluation measures is available via the Ottawa Health Research Institute (OHRI) Health Decision Centre (OHDEC) web site at http://decisionaid.ohri.ca/eval.html. Tools to evaluate healthcare provider communication skills and implementation of decision support in consultations to foster shared decision making, such as the Decision Support Analysis Tool (DSAT) (Guimond et al., 2003) are also being developed and tested. Studies by Bunn and O'Connor (1996) and Wills and Holmes-Rovner (2003b) provide the first preliminary validation information for mental health populations for earlier versions of the Ottawa decisional conflict measure, as well as other decision-relevant measures such as the SWD scale (Holmes-Rovner et al., 1996). In addition, Cooper et al. (2000) reported the preliminary validation of the patient attitudes toward and ratings of care for depression (PARC-D).
Preference-Based Enhancements to Standard Intervention Designs
RCTs and Preference-Driven Treatment Decisions
Standard randomized clinical trials (RCTs) have increasingly been criticized in regard to their usefulness for “real-world” deployment and assessment of intervention effectiveness (for additional information about the positions taken in this debate, see Conn, Rantz, Wipke-Tevis, & Mass, 2001; Fogg & Gross, 2000; Gross & Fogg, 2001; Ward, Donovan, & Serlin, 2003). RCTs are widely acknowledged as the “gold standard” for efficacy research because of their design features that foster high internal validity to enable strong causal inferences. The logic of random assignment as a critical condition of a true experimental design is that it serves as an all-purpose mechanism for control of preexisting differences between individuals enrolled in various study conditions. In a traditional RCT, random assignment of participants to study conditions assumes that patients either have equal preference for study condition assignment (such as they are truly willing to be randomly assigned to study conditions) or that patient preferences can or should be set aside in favor of random assignment to study conditions. The incorporation of decision-making concepts into mental health intervention designs has the potential to improve certain types of traditional interventions, especially those that can be viewed as involving “preference-driven” treatment decision making.
A preference-driven decision is a choice that is (or should be) based on personal values about treatment options. The impact of patient preferences on the process and outcomes of mental health interventions has begun to receive heightened research attention in recent years. For example, Dwight-Johnson et al. (2001) found that a primary care depression quality improvement intervention that incorporated patients' preferred treatment choices increased the likelihood that patients would enter treatment and receive their preferred treatment. Preference-driven decision making occurs in two types of situations. With reference to Figure 1, information, values, or both types of variables can shape the nature of preferences. The first situation occurs when information about which treatment option is most likely to be effective or best in other respects is believed to be equivalent, or the efficacy of the options is uncertain. In this instance, a state of “therapeutic equipoise” is said to be present for the treatment decision-making situation. For example, all other things being equal, a patient with mild to moderate depression may have an approximately equal likelihood of benefiting from medication, psychotherapy, or both options, for treatment of a major depressive episode. The second type of situation occurs when the patient's values about the benefits (pros) and downsides (cons) of particular options are (or can be) well defined, assuming that adequate information is available to the patient about the alternative treatment options. For example, when making an initial decision about treatment options for depression, one person may be strongly opposed to the use of medication for religious reasons and prefer counseling appointments instead, but another person may prefer medication to attending weekly psychotherapy appointments. These types of values can strongly influence the nature of patient preferences for the treatment options.
Equipoise-Stratified Randomization
Recent innovations in mental health interventions research designs have begun to address the information and value aspects of patient preference-driven decision making, within a goal of improving the process and outcomes of interventions. One approach is to combine considerations of therapeutic equipoise and patient and clinician values embodied in an equipoise-stratified randomization approach to conducting clinical trials of mental health treatment (Lavori et al., 2001). Lavori et al. discussed features of this design innovation using the NIMH-sponsored Sequenced Treatment Alternatives to Relieve Depression (STAR*D) trial for treatment-resistant depression.
Other Preference-Based Enhancements
Several other key approaches have been proposed for enhancing intervention designs that incorporate patient preferences. Particularly when patient preferences are well defined for treatment options, partial randomization and delayed intervention designs may also be useful enhancements to the standard RCT. These approaches may be useful in instances where at least some patients are unwilling to accept random assignment to study conditions. In a partial randomization design, there are standard arms of the trial in which patients are randomly assigned to study conditions. In addition, however, there are “preference” arms of the study design in which patients can be assigned to study conditions based on their preferred treatments. Partial randomization designs are becoming increasingly common in the clinical research literature (Chilvers et al., 2001). Dwight-Johnson et al. (2001) concluded that intervention designs supporting patient preferences for treatment can improve the likelihood of patients entering treatment. The preference arm analysis, however, must take into account that patients self-selected into treatments. In a delayed intervention approach, patients who prefer particular treatments can have the option of receiving their preferred treatment later on. Like partial randomization trials, delayed intervention approaches are also becoming more common in the clinical research literature. If offering a treatment option later on is both feasible and ethical, it may produce an incentive for patients to initially accept random assignment to a nonpreferred treatment option.
CONCLUSIONS
The incorporation of decision-making variables into mental health interventions research has both exciting prospects as well as issues in need of further consideration and systematic research. Much descriptive work remains to be done, as well as testing the circumstances for which interventions focused on decision making can potentially improve mental health care as usual. Other types of enhancements to standard RCT design are also promising routes to better linking of efficacy and effectiveness research. There remain significant challenges to implementing optimal shared decision making in routine care settings (Edwards, Evans, & Elwyn, 2003), and additional research is needed on best practices in ordinary, high-volume care. In addition, a more radical reform agenda will mean reconceptualizing the system to include the community, the public health information system, and the health system as supporting patients and care teams in dynamic interaction.
Key challenges for future research designed to integrate decision making and mental health interventions research include needs for (a) improved measures for characterizing decision-making processes that are matched to study populations, complexity, and types of decision making; (b) testing DAs in effectiveness research for diverse populations and clinical settings; and (c) improving the understanding and incorporation of preference concepts in enhanced intervention designs. This research agenda will take place at the traditional patient level of services research. In addition, interventions research should be conducted that cuts across the person, medical system, and community levels and brings public sector enhancements to information to bear on system- and patient-level decisions.
ACKNOWLEDGMENT
The authors express appreciation to the special issue editors (H. Ringeisen, J. Sherrill, M. Southam-Gerow) and anonymous reviewers for very helpful feedback on earlier drafts of this article.
Footnotes
In this article, we use the terms patient and health-care user interchangeably. The term patient has been used most often in the clinical decision-making literature, but the term healthcare user designates a more active consumer role that is often better matched with the shared treatment decision-making paradigm.
We recognize that there are some mental health treatment contexts in which the patient does not make a fully autonomous choice. Also, competence of patients with more significant forms of mental illness to consent to treatment and research participation has been the subject of debate for a number of years (Appelbaum, Grisso, Frank, O'Donell, & Kupfer, 1999). However, these situations are comparatively rare in the primary care setting treatment context, and lack of fully voluntary choice does not necessarily preclude the incorporation of patient perspectives in decisions about care. See also the work of Pescosolido et al. (1998) that provides a critique of the concept of decision making in mental health treatment contexts in which there is a lack of fully voluntary choice.
There are now a plethora of “decision-making” terms evident in the literature, which are often unclearly and inconsistently defined, such as shared decision making, patient-centered, patient involvement or participation, empowerment, and patient activation. The terms empowerment (Roberts, 1999), patient activation, and shared decision making have also been used somewhat interchangeably in the literature—see Rodwell (1996) for an analysis of the concept of empowerment—but empowerment essentially refers to patient-centered activation, whereas shared decision making more centrally considers the exchange of information and values between the patient and provider. Involving patients as more active participants in shared decision making has often been referred to as being “patient-centered,” or fostering “patient participation” (Cahill, 1996), but overall, key terms have often not been well defined or operationalized to date in the literature (Elwyn, Edwards, Kinnersley, & Grol, 2000). For additional definitions of some of these terms, see the recent summary by Trevena and Barratt (2003).
For a review of three standardized tools to assess the quality of health information on the Internet, see Ademiluyi, Rees, & Sheard (2003).
REFERENCES
- Ackermann R, Williams J. Rational treatment choices for non-major depressions in primary care. Journal of General Internal Medicine. 2002;17:293–301. doi: 10.1046/j.1525-1497.2002.10350.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ademiluyi G, Rees CE, Sheard CE. Evaluating the reliability and validity of three tools to assess the quality of health information on the Internet. Patient Education and Counseling. 2003;50:151–155. doi: 10.1016/s0738-3991(02)00124-6. [DOI] [PubMed] [Google Scholar]
- Agency for Health Care Research and Policy Consumer health informatics and patient decision making. http://www.ahcpr.gov/research/rtisumm.htm. 1998 Retrieved from.
- Alvidrez J, Azocar F. Distressed women's clinic patients: Preferences for mental health treatments and perceived obstacles. General Hospital Psychiatry. 1999;21:340–347. doi: 10.1016/s0163-8343(99)00038-9. [DOI] [PubMed] [Google Scholar]
- Appelbaum PS, Grisso T, Frank E, O'Donell S, Kupfer DJ. Competence of depressed patients for consent to research. American Journal of Psychiatry. 1999;156:1380–1384. doi: 10.1176/ajp.156.9.1380. [DOI] [PubMed] [Google Scholar]
- Barrett B, Kiefer D, Rabago D. Assessing the risks and benefits of herbal medicine: An overview of scientific evidence. Alternative Therapies. 1999;5(4):40–49. [PubMed] [Google Scholar]
- Barry MJ. Involving patients in medical decisions. How can physicians do better? Journal of the American Medical Association. 1999;282(24):2356–2357. doi: 10.1001/jama.282.24.2356. [DOI] [PubMed] [Google Scholar]
- Bekker HL, Hewison J, Thornton JG. Understanding why decision aids work: Linking process with outcome. Patient Education and Counseling. 2003;50:323–329. doi: 10.1016/s0738-3991(03)00056-9. [DOI] [PubMed] [Google Scholar]
- Bekker HL, Legare F, Stacey D, O'Connor A, Lemyre L. Is anxiety a suitable measure of decision aid effectiveness? A systematic review. Patient Education and Counseling. 2003;50:255–262. doi: 10.1016/s0738-3991(03)00045-4. [DOI] [PubMed] [Google Scholar]
- Bessell T, McDonald S, Silagy C, Anderson J, Hiller J, Sansom L. Do Internet interventions for consumers cause more harm than good? A systematic review. Health Expectations. 2002;5:25–37. doi: 10.1046/j.1369-6513.2002.00156.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bleyen K, Vertommen H, Van Audenhove C. A negotiation approach to systematic treatment selection: An evaluation of its impact on the initial phase of psychotherapy. European Journal of Psychological Assessment. 1998;14(1):14–25. [Google Scholar]
- Bridson J, Hammond C, Leach A, Chester M. Making consent patient centred. British Medical Journal. 2003;327(15):1159–1161. doi: 10.1136/bmj.327.7424.1159. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Britt E, Hudson SM, Blampied NM. Motivational interviewing in health care settings: A review. Patient Education and Counseling. 2004;53(2):147–155. doi: 10.1016/S0738-3991(03)00141-1. [DOI] [PubMed] [Google Scholar]
- Bunn H, Jacobsen MJ, Whitelaw C, McIntosh A, Fox JC. Decision making in clinical depression: A Canadian perspective; Paper presented at the 2nd International Shared Decision Making Conference; Swansea, Wales. 2003. [Google Scholar]
- Bunn H, O'Connor A. Validation of client decision-making instruments in the context of psychiatry. Canadian Journal of Nursing Research. 1996;28(3):13–27. [PubMed] [Google Scholar]
- Cahill J. Patient participation: A concept analysis. Journal of Advanced Nursing. 1996;24:561–571. doi: 10.1046/j.1365-2648.1996.22517.x. [DOI] [PubMed] [Google Scholar]
- Charles C, Gafni A, Whelan T. Shared decision-making in the medical encounter: What does it mean? (Or it takes at least two to tango) Social Science and Medicine. 1997;44(5):681–692. doi: 10.1016/s0277-9536(96)00221-3. [DOI] [PubMed] [Google Scholar]
- Charles C, Whelan T, Gafni A. What do we mean by partnership in making decisions about treatment? British Medical Journal. 1999;319:780–782. doi: 10.1136/bmj.319.7212.780. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Charnock D, Shepperd S, Needham G, Gann R. DISCERN: An instrument for judging the quality of written consumer health information on treatment choices. Journal of Epidemiology and Community Health. 1999;53:105–111. doi: 10.1136/jech.53.2.105. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Chilvers C, Dewey M, Fielding K, Gretton V, Miller P, Palmer B, et al. Antidepressant drugs and generic counselling for treatment of major depression in primary care: Randomised trial with patient preference arms. British Medical Journal. 2001;322:772–775. doi: 10.1136/bmj.322.7289.772. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Christensen H, Griffiths KM, Jorm AF. Delivering interventions for depression by using the Internet: Randomised controlled trial. British Medical Journal. 2004;328(7434):265–260. doi: 10.1136/bmj.37945.566632.EE. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Conn VS, Rantz MJ, Wipke-Tevis DD, Mass ML. Designing effective nursing interventions. Research in Nursing & Health. 2001;24:433–442. doi: 10.1002/nur.1043. [DOI] [PubMed] [Google Scholar]
- Cooksey RW. Judgment analysis: Theory, methods, and applications. Academic Press; San Diego, CA: 1996. [Google Scholar]
- Cooper L, Brown C, Vu HT, Palenchar D, Gonzales JJ, Ford D, et al. Primary care patients' opinions regarding the importance of various aspects of care for depression. General Hospital Psychiatry. 2000;22:163–173. doi: 10.1016/s0163-8343(00)00073-6. [DOI] [PubMed] [Google Scholar]
- Cooper LA, Gonzales JJ, Gallo JJ, Rost KM, Meredith LS, Rubenstein LV, et al. The acceptability of treatment for depression among African-American, Hispanic, and white primary care patients. Medical Care. 2003;41(4):479–489. doi: 10.1097/01.MLR.0000053228.58042.E4. [DOI] [PubMed] [Google Scholar]
- Cooper-Patrick L, Gallo JJ, Gonzales JJ, Vu HT, Nelson C, Ford DE. Race, gender, and partnership in the patient–physician relationship. Journal of the American Medical Association. 1999;282(6):583–589. doi: 10.1001/jama.282.6.583. [DOI] [PubMed] [Google Scholar]
- Cooper-Patrick L, Powe NR, Jenckes MW, Gonzales JJ, Levine DM, Ford DE. Identification of patient attitudes and preferences regarding treatment of depression. Journal of General Internal Medicine. 1997;12:431–438. doi: 10.1046/j.1525-1497.1997.00075.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Coulter A, Entwistle V, Gilbert D. Sharing decisions with patients: Is the information good enough? British Medical Journal. 1999;318:318–322. doi: 10.1136/bmj.318.7179.318. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cruz M, Pincus H. Research on the influence that communication in psychiatric encounters has on treatment. Psychiatric Services. 2002;53(10):1253–1265. doi: 10.1176/appi.ps.53.10.1253. [DOI] [PubMed] [Google Scholar]
- Davis R, Dolan G, Mead D, Atwell C, Nehammer S, Moseley L, et al. Exploring doctor and patient views about risk communication and shared decision-making in the consultation. Health Expectations. 2003;6:198–207. doi: 10.1046/j.1369-6513.2003.00235.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Deber RB, Kraetschmer N, Irvine J. What role do patients wish to play in treatment decision making? Archives of Internal Medicine. 1996;156:1414–1420. [PubMed] [Google Scholar]
- Delaney BC, Fitzmaurice DA, Riaz A, Hobbs FDR. Can computerised decision support systems deliver improved quality in primary care? British Medical Journal. 1999;319:1281. doi: 10.1136/bmj.319.7220.1281. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Deyo RA. A key medical decision maker: The patient. British Medical Journal. 2001;323:466–467. doi: 10.1136/bmj.323.7311.466. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Diaz J, Griffith R, Ng J, Reinert S, Friedmann P, Moulton A. Patients' use of the Internet for medical information. Journal of General Internal Medicine. 2002;17:180–185. doi: 10.1046/j.1525-1497.2002.10603.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dowie J. The role of patients' meta-preferences in the design and evaluation of decision support systems. Health Expectations. 2002;5:16–27. doi: 10.1046/j.1369-6513.2002.00160.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- van Dulmen S. Patient-centerdness. Patient Education and Counseling. 2003;51(3):195–196. [Google Scholar]
- Dwight-Johnson M, Sherbourne CD, Liao D, Wells KB. Treatment preferences among depressed primary care patients. Journal of General Internal Medicine. 2000;15:527–534. doi: 10.1046/j.1525-1497.2000.08035.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dwight-Johnson M, Unutzer J, Sherbourne C, Tang L, Wells K. Can quality improvement programs for depression in primary care address patient preferences for treatment? Medical Care. 2001;39(9):934–944. doi: 10.1097/00005650-200109000-00004. [DOI] [PubMed] [Google Scholar]
- Edwards A, Evans R, Elwyn G. Manufactured but not imported: New directions for research in shared decision making support and skills. Patient Education and Counseling. 2003;50:33–38. doi: 10.1016/s0738-3991(03)00077-6. [DOI] [PubMed] [Google Scholar]
- Elwyn G, Edwards A, Kinnersley P, Grol R. Shared decision making and the concept of equipoise: The competences of involving patients in healthcare choices. British Journal of General Practise. 2000;50:892–897. [PMC free article] [PubMed] [Google Scholar]
- Fagerlin A, Rovner DR, Stableford S, Wei JT, Jentoft C, Holmes-Rovner M. Patient education materials about the treatment of early-stage prostate cancer: A critical review. Annals of Internal Medicine. 2004;140(9):721–728. doi: 10.7326/0003-4819-140-9-200405040-00012. [DOI] [PubMed] [Google Scholar]
- Feldman-Stewart D, Brundage MD. Challenges for designing and implementing decision aids. Patient and Education Counseling. 2004;54(3):265–273. doi: 10.1016/j.pec.2003.09.007. [DOI] [PubMed] [Google Scholar]
- Feldman-Stewart D, Brundage MD, McConnell BA, Mackillop WJ. Practical issues in assisting shared decision making. Health Expectations. 2000;3:46–54. doi: 10.1046/j.1369-6513.2000.00082.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fogg L, Gross D. Threats to validity in randomized clinical trials. Research in Nursing. 2000;23:79–87. doi: 10.1002/(sici)1098-240x(200002)23:1<79::aid-nur9>3.0.co;2-r. [DOI] [PubMed] [Google Scholar]
- Gask L. Listening to patients. British Journal of Psychiatry. 1997;171:301–302. doi: 10.1192/bjp.171.4.301. [DOI] [PubMed] [Google Scholar]
- Gask L, Rogers A. Bridging the gap: Mapping a new generation of primary mental health care research. Journal of Mental Health. 1998;7(6):539–541. [Google Scholar]
- George LK, Lynch SM. Race differences in depressive symptoms: A dynamic perspective on stress exposure and vulnerability. Journal of Health and Social Behavior. 2003;44(3):353–369. [PubMed] [Google Scholar]
- Gigerenzer G, Todd PM. Simple heuristics that make us smart. Oxford University Press; New York: 1999. [Google Scholar]
- Godolphin W, Towle A, McKendry R. Evaluation of the quality of patient information to support informed shared decision-making. Health Expectations. 2001;4:235–242. doi: 10.1046/j.1369-6513.2001.00144.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Graham ID, Logan J, O'Connor A, Weeks KE, Aaron S, Cranney A, et al. A qualitative study of physicians' perceptions of three decision aids. Patient Education and Counseling. 2003;50(3):279–283. doi: 10.1016/s0738-3991(03)00050-8. [DOI] [PubMed] [Google Scholar]
- Griffiths KM, Christenson H. Quality of web based information on treatment of depression: Cross sectional survey. British Medical Journal. 2000;321:1511–1515. doi: 10.1136/bmj.321.7275.1511. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gross D, Fogg L. Clinical trials in the 21st century: The case for participant-centered research. Research in Nursing & Health. 2001;24(6):530–539. doi: 10.1002/nur.10010. [DOI] [PubMed] [Google Scholar]
- Guimond P, Bunn H, O'Connor AM, Jacobsen MJ, Tait VK, Drake ER, et al. Validation of a tool to assess health practitioners' decision support and communication skills. Patient Education and Counseling. 2003;50(3):235–245. doi: 10.1016/s0738-3991(03)00043-0. [DOI] [PubMed] [Google Scholar]
- de Haes H, Koedoot N. Patient centered decision making in palliative cancer treatment: A world of paradoxes. Patient Education and Counseling. 2003;50:43–49. doi: 10.1016/s0738-3991(03)00079-x. [DOI] [PubMed] [Google Scholar]
- Hammond KR. Human judgment and social policy: Irreducible uncertainty, inevitable error, unavoidable injustice. Oxford University Press; New York: 1996. [Google Scholar]
- Harmann J, Kissling W. Shared decision making for inpatients with schizophrenia; Paper presented at the 2nd International Shared Decision Making Conference; Swansea, Wales. 2003. [Google Scholar]
- Harrington J, Noble LM, Newman SP. Improving patients' communication with doctors: A systematic review of intervention studies. Patient Education and Counseling. 2004;52:7–16. doi: 10.1016/s0738-3991(03)00017-x. [DOI] [PubMed] [Google Scholar]
- Hastie R. Problems for judgment and decision making. Annual Review of Psychology. 2001;52:653–683. doi: 10.1146/annurev.psych.52.1.653. [DOI] [PubMed] [Google Scholar]
- Hastie R, Dawes RM. Rational choice in an uncertain world: The psychology of judgment and decision making. Sage; Thousand Oaks, CA: 2001. [Google Scholar]
- Hohmann A, Shear K. Community-based interventions research: Coping with the “noise” of real life in study design. The American Journal of Psychiatry. 2002;159(2):201–207. doi: 10.1176/appi.ajp.159.2.201. [DOI] [PubMed] [Google Scholar]
- Holmes-Rovner M, Kroll J, Rovner DR, Schmitt N, Rothert M, Padonu G, et al. Patient decision support intervention: Increased consistency with decision analytic models. Medical Care. 1999;37(3):270–284. doi: 10.1097/00005650-199903000-00007. [DOI] [PubMed] [Google Scholar]
- Holmes-Rovner M, Kroll J, Schmitt N, Rovner DR, Breer ML, Rothert ML, et al. Patient satisfaction with health care decisions: The Satisfaction With Decision Scale. Medical Decision Making. 1996;16:58–64. doi: 10.1177/0272989X9601600114. [DOI] [PubMed] [Google Scholar]
- Holmes-Rovner M, Llewellyn-Thomas H, Entwistle V, Coulter A, O'Connor A, Rovner DR. Patient choice modules for summaries of clinical effectiveness: A proposal. British Medical Journal. 2001;322:664–667. doi: 10.1136/bmj.322.7287.664. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Holmes-Rovner M, Wills CE. Improving informed consent: Insights from behavioral decision research. Medical Care. 2002;40(Suppl 9):V30–V38. doi: 10.1097/01.MLR.0000023953.55783.4A. [DOI] [PubMed] [Google Scholar]
- Hunink M, Glasziou P, editors. Decision making in health and medicine: Integrating evidence and values. Cambridge University Press; Cambridge, UK: 2001. [Google Scholar]
- Institute of Medicine . Crossing the quality chasm: A new health system for the 21st century/Committee on Quality Health Care in America. Author; Washington, DC: 2001. [Google Scholar]
- IPDAS IPDAS 2005: Criteria for development and evaluation of patient decision aids; Paper presented at the International Shared Decision Making Conference; Ottawa, Canada. 2005. [Google Scholar]
- Juslin P, Montgomery H. Judgment and decision making: Neo-Brunswikian and process-tracing approaches. Lawrence Erlbaum Associates; Mahwah, NJ: 1999. [Google Scholar]
- Kaplan SH, Gandek B, Greenfield S, Rogers W, Ware JE. Patient and visit characteristics related to physicians' participatory decision-making style: Results from the Medical Outcomes Study. Medical Care. 1995;33:1176–1187. doi: 10.1097/00005650-199512000-00002. [DOI] [PubMed] [Google Scholar]
- Kennedy A, Robinson A, Rogers A. Incorporating patients' views and experiences of life with IBS in the development of an evidence based self-help guidebook. Patient Education and Counseling. 2003;50(3):303–310. doi: 10.1016/s0738-3991(03)00054-5. [DOI] [PubMed] [Google Scholar]
- Lauver D, Ward S, Heidrich S, Keller M, Bowers B, Brennan P, et al. Patient-centered interventions. Research in Nursing & Health. 2002;25:246–255. doi: 10.1002/nur.10044. [DOI] [PubMed] [Google Scholar]
- Lavori PW, Rush AJ, Wisniewski SR, Alpert JE, Fava M, Kupfer DJ, et al. Strengthening clinical effectiveness trials: Equipoise-stratified randomization. Biological Psychiatry. 2001;50:792–801. doi: 10.1016/s0006-3223(01)01223-9. [DOI] [PubMed] [Google Scholar]
- Link B, Struening E, Neese-Todd S, Asmussen S, Phelan J. The consequences of stigma for the self-esteem of people with mental illness. Psychiatric Services. 2001;52(12):1621–1626. doi: 10.1176/appi.ps.52.12.1621. [DOI] [PubMed] [Google Scholar]
- Lissman T, Boehnlein J. A critical review of Internet information about depression. Psychiatric Services. 2001;52(8):1046–1050. doi: 10.1176/appi.ps.52.8.1046. [DOI] [PubMed] [Google Scholar]
- Loh A, Giersdorf N, Simon D, Harter M. Shared decision making in primary care of depression: General practitioners' clinical management and patients' perception of decision making process; Paper presented at the 2nd International Shared Decision Making Conference; Swansea, Wales. 2003. [Google Scholar]
- Ludman E, Katon W, Bush C, Rutter C, Lin E, Simon G, et al. Behavioural factors associated with symptom outcomes in primary care-based depression prevention intervention trial. Psychological Medicine. 2003;33:1061–1070. doi: 10.1017/s003329170300816x. [DOI] [PubMed] [Google Scholar]
- Masi CM, Suarez-Balcazar Y, Cassey MZ, Kinney L, Piotrowski H. Internet access and empowerment: A community-based health initiative. Journal of General Internal Medicine. 2003;18:525–530. doi: 10.1046/j.1525-1497.2003.20344.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mental Health . Office of the U.S. Surgeon General; Washington, DC: 1999. A Report of the Surgeon General. [Google Scholar]
- Mojtabai R, Olfson M, Mechanic D. Perceived need and help-seeking in adults with mood, anxiety, or substance use disorders. Archives of General Psychiatry. 2002;59(1):77–84. doi: 10.1001/archpsyc.59.1.77. [DOI] [PubMed] [Google Scholar]
- Newell A, Simon HA. Elements of a theory of human problem solving. Psychological Review. 1958;65(3):151–166. [Google Scholar]
- Nezu AM. Problem solving and behavior therapy revisited. Behavior Therapy. 2004;35(1):1–33. [Google Scholar]
- Nezu AM, D'Zurilla TJ, Zwick ML, Nezu CM. Problem-solving therapy for adults. In: D'Zurilla TJ, Chang C, editors. Social problem solving: Theory, research, and training. American Psychological Association; Washington, DC: 2004. pp. 171–191. [Google Scholar]
- National Institute of Mental Health . Bridging science and service: A report by the National Advisory Mental Health Council Clinical Treatment and Services Research Workgroup. Author; Washington, DC: 1999. [Google Scholar]
- National Institute of Mental Health . Consider this: Cyber interventions in mental health—Ethical considerations. Internet Ethics Workshop; Bethesda, MD: 2000. [Google Scholar]
- National Institute of Mental Health . Internet-based research interventions in mental health: How are they working? Bethesda, MD: 2003. [Google Scholar]
- O'Connor A. Using patient decision aids to promote evidence-based decision making. ACP Journal Club. 2001;135:A11–A12. [PubMed] [Google Scholar]
- O'Connor AM. Validation of a decisional conflict scale. Medical Decision Making. 1995;15:25–30. doi: 10.1177/0272989X9501500105. [DOI] [PubMed] [Google Scholar]
- O'Connor AM. A call to standardize measures for judging the efficacy of interventions to aid patients' decision making. Medical Decision Making. 1999;19(4):504–505. doi: 10.1177/0272989X9901900420. [DOI] [PubMed] [Google Scholar]
- O'Connor AM, Drake ER, Fiset V, Graham ID, Laupacis A, Tugwell P. The Ottawa patient decision aids. Effective Clinical Practice. 1999;2:163–170. [PubMed] [Google Scholar]
- O'Connor AM, Fiset V, DeGrasse C, Graham I, Evans W, Stacey D, et al. Decision aids for patients considering health care options: Evidence of efficacy and policy implications. Journal of the National Cancer Institute Monographs. 1999;25:67–80. doi: 10.1093/oxfordjournals.jncimonographs.a024212. [DOI] [PubMed] [Google Scholar]
- O'Connor AM, Rostom A, Fiset V, Tetroe J, Entwistle V, Llewellyn-Thomas H, et al. Decision aids for patients facing health treatment or screening decisions: Systematic review. British Medical Journal. 1999;319:731–734. doi: 10.1136/bmj.319.7212.731. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Payne JW, Bettman JR, Johnson EJ. Behavioral decision research: A constructive processing perspective. Annual Review of Psychology. 1992;43:87–131. [Google Scholar]
- Pescosolido BA, Brooks Gardner C, Lubell KM. How people get into mental health services: Stories of choice, coercion and “muddling through” from “first-timers.”. Social Science and Medicine. 1998;46(2):275–286. doi: 10.1016/s0277-9536(97)00160-3. [DOI] [PubMed] [Google Scholar]
- Pierce PF, Hicks FD. Patient decision-making behavior: An emerging paradigm for nursing science. Nursing Research. 2001;50(5):267–274. doi: 10.1097/00006199-200109000-00003. [DOI] [PubMed] [Google Scholar]
- Roberts KJ. Patient empowerment in the United States: A critical commentary. Health Expectations. 1999;2:82–92. doi: 10.1046/j.1369-6513.1999.00048.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rodwell CM. An analysis of the concept of empowerment. Journal of Advanced Nursing. 1996;23:305–313. doi: 10.1111/j.1365-2648.1996.tb02672.x. [DOI] [PubMed] [Google Scholar]
- Roeloffs C, Sherbourne C, Unutzer J, Fink A, Tang L, Wells K. Stigma and depression among primary care patients. General Hospital Psychiatry. 2003;25:311–315. doi: 10.1016/s0163-8343(03)00066-5. [DOI] [PubMed] [Google Scholar]
- Rost K, Smith GR, Taylor JL. Rural-urban differences in stigma and the use of care for depressive disorders. Journal of Rural Health. 1993;9(1):57–62. doi: 10.1111/j.1748-0361.1993.tb00495.x. [DOI] [PubMed] [Google Scholar]
- Roter D. The medical visit context of treatment decision-making and the therapeutic relationship. Health Expectations. 2000;3:17–25. doi: 10.1046/j.1369-6513.2000.00073.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Roter DL. Observations on methodological and measurement challenges in the assessment of communication during medical exchanges. Patient Education and Counseling. 2003;50:17–21. doi: 10.1016/s0738-3991(03)00074-0. [DOI] [PubMed] [Google Scholar]
- Rothert ML, Holmes-Rovner M, Rovner D, Kroll J, Breer L, Talarczyk G, et al. An educational intervention as a decision support for menopausal women. Research in Nursing & Health. 1997;20:377–387. doi: 10.1002/(sici)1098-240x(199710)20:5<377::aid-nur2>3.0.co;2-l. [DOI] [PubMed] [Google Scholar]
- Say R, Thomson R. The importance of patient preferences in treatment decisions-challenges for doctors. British Medical Journal. 2003;327(6):542–545. doi: 10.1136/bmj.327.7414.542. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Schoemaker PJ. The expected utility model: Its variants, purposes, evidence and limitations. Journal of Economic Literature. 1982;20:529–563. [Google Scholar]
- Schulz A, Williams D, Israel B, Becker A, Parker E, James S, et al. Unfair treatment, neighborhood effects, and mental health in the Detroit metropolitan area. Journal of Health and Social Behavior. 2000;41:314–332. [PubMed] [Google Scholar]
- Sepucha KR, Mulley AG. Extending decision support: Preparation and implementation. Patient Education and Counseling. 2003;50:269–271. doi: 10.1016/s0738-3991(03)00048-x. [DOI] [PubMed] [Google Scholar]
- Sherbourne CD, Sturm R, Wells KB. What outcomes matter to patients? Journal of General Internal Medicine. 1999;14:357–363. doi: 10.1046/j.1525-1497.1999.00354.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Simon D, Loh A, Giersdorf N, Harter M. The process of communication and decision-making between physician and patient in primary care of depressive disorders; Paper presented at the 2nd International Shared Decision Making Conference; Swansea, Wales. 2003. [Google Scholar]
- Sirey J, Brue M, Alexopoulos G, Perlick D, Friedman S, Meyers B. Perceived stigma and patient-rated severity of illness as predictors of antidepressant drug adherence. Psychiatric Services. 2001;52(12):1615–1620. doi: 10.1176/appi.ps.52.12.1615. [DOI] [PubMed] [Google Scholar]
- Stacey D, O'Connor A. http://decisionaid.ohri.ca/cochinvent.php. Cochrane inventory of existing patient decision aids identified using Cochrane review methods. 2004 Retrieved from Ottawa Health Decision Centre Web site. [Google Scholar]
- Stevenson FA. General practitioners' views on shared decision making: A qualitative analysis. Patient Education and Counseling. 2003;50(3):291–293. doi: 10.1016/s0738-3991(03)00052-1. [DOI] [PubMed] [Google Scholar]
- Towle A, Godolphin W. Framework for teaching and learning informed shared decision making. British Medical Journal. 1999;319:766–771. doi: 10.1136/bmj.319.7212.766. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Trede F, Higgs J. Re-framing the clinician's role in collaborative clinical decision making: Re-thinking practice knowledge and the notion of clinician–patient relationships. Learning in Health and Social Care. 2003;2(2):66–73. [Google Scholar]
- Trevena L, Barratt A. Integrated decision making: Definitions for a new discipline. Patient Education and Counseling. 2003;50(3):265–268. doi: 10.1016/s0738-3991(03)00047-8. [DOI] [PubMed] [Google Scholar]
- Ubel P. What should I do, doc? Archives of Internal Medicine. 2002;162:977–980. doi: 10.1001/archinte.162.9.977. [DOI] [PubMed] [Google Scholar]
- Unutzer J, Klap R, Sturm R, Young A, Marmon T, Shatkin J, et al. Mental disorders and the use of alternative medicine: Results from a national survey. American Journal of Psychiatry. 2000;157(11):1851–1857. doi: 10.1176/appi.ajp.157.11.1851. [DOI] [PubMed] [Google Scholar]
- Van Audenhove C, Vertommen H. A negotiation approach to intake and treatment choice. Journal of Psychotherapy Integration. 2000;10(3):287–299. [Google Scholar]
- Von Korff M, Katon W, Unutzer J, Wells K, Wagner EH. Improving depression care: Barriers, solutions, and research needs. The Journal of Family Practice. 2001;50(6):529. [PubMed] [Google Scholar]
- Von Korff M, Unutzer J, Katon W, Wells K. Improving care for depression in organized health care systems: A conference report. The Journal of Family Practice. 2001;50(6):530–531. [PubMed] [Google Scholar]
- Wagner EH. Chronic disease management: What will it take to improve care for chronic illness? Effective Clinical Practice. 1998;1:2–4. [PubMed] [Google Scholar]
- Wagner T, Hibbard J. Who uses self-care books, advice nurses, and computers for health information? International Journal of Technology Assessment in Health Care. 2001;17(4):590–600. [PubMed] [Google Scholar]
- Ward S, Donovan HS, Serlin RC. Commentary: An alternative view on “an alternative paradigm.”. Research in Nursing & Health. 2003;26:256–259. doi: 10.1002/nur.10088. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wills CE. Young adult medication decision making: Similarities and differences among mental versus physical health treatment contexts. Journal of Nursing Science. 1997;2(34):59–72. [Google Scholar]
- Wills CE. Primary care patient depression treatment decision-making: Needs, preferences, and sources of decisional conflict; Paper presented at the 2nd International Shared Decision Making Conference; Swansea, Wales. 2003a. [Google Scholar]
- Wills CE. Primary care patient depression treatment decision-making: Needs, preferences, and sources of decisional conflict; Paper presented at the NIH Mental Health Services Research Conference; Washington, DC. 2003b. [Google Scholar]
- Wills CE. Migraine headache and psychiatric co-morbidity: Survey versus claims data; Paper presented at the NIH Mental Health Services Research Conference; Washington, DC. 2004. [Google Scholar]
- Wills CE, Holmes-Rovner M. Patient comprehension of information for shared treatment decision making: State of the art and future directions. Patient Education & Counseling. 2003a;50:285–290. doi: 10.1016/s0738-3991(03)00051-x. Special Issue on Shared Decision Making. [DOI] [PubMed] [Google Scholar]
- Wills CE, Holmes-Rovner M. Preliminary validation of the Satisfaction With Decision Scale with depressed primary care patients. Health Expectations. 2003b;6:149–159. doi: 10.1046/j.1369-6513.2003.00220.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wright KB, Bell SB. Health-related support groups on the internet: Linking empirical findings to social support and computer-mediated communication theory. Journal of Health Psychology. 2003;8(1):39–54. doi: 10.1177/1359105303008001429. [DOI] [PubMed] [Google Scholar]
- Zsambok CE, Klein G, editors. Naturalistic decision making. Lawrence Erlbaum; Mahwah, NJ: 1997. [Google Scholar]