

Abstract
Background
When the portion size and energy density (in kcal/g) of a food are varied simultaneously in a single meal, each influences energy intake independently.
Objective
We aimed to determine how the effects of portion size and energy density combine to influence energy intake and satiety over multiple meals for 2 d.
Design
In a crossover design, 24 young women were provided with meals and snacks for 2 consecutive days per week for 4 wk; all foods were consumed ad libitum. Across the 4 sessions, the subjects were served the same 2 daily menus, but all foods were varied in portion size and energy density between a standard level (100%) and a reduced level (75%).
Results
Reducing the portion size and energy density of all foods led to significant and independent decreases in energy intake over 2 d (P < 0.0001). A 25% decrease in portion size led to a 10% decrease in energy intake (231 kcal/d), and a 25% decrease in energy density led to a 24% decrease in energy intake (575 kcal/d). The effects on energy intake were additive and were sustained from meal to meal. Despite the large variation in energy intake, there were no significant differences in the ratings of hunger and fullness across conditions over the 2 d.
Conclusions
Reductions in portion size and energy density independently decreased ad libitum energy intake in women when commonly consumed foods were served over 2 d. Reductions in both portion size and energy density can help to moderate energy intake without increased hunger.
Keywords: Portion size, energy density, energy intake, obesity prevention and control, satiety, humans, adult, clinical trial, crossover studies
INTRODUCTION
The recent surge in the incidence of overweight and obesity may be related in part to the ease of access to large portions of energy-dense foods (1, 2). Such foods are not only widely available but are also often highly palatable and inexpensive (3). Evidence suggests that increases in both the portion size and energy density of foods encourage the overconsumption of energy (4, 5). Although such findings have indicated to policy makers that consumers should limit their portions of energy-dense foods (6, 7), more data are required to assess the effect of following this advice. The questions addressed in the present study are whether moderate reductions in both the portion size and energy density of commonly consumed foods combine to decrease energy intake and whether the decrease is sustained over a period of 2 d.
Variations in portion size have robust effects on energy intake across a range of different types of foods (8–11). As the portion size served is increased, both weight of food consumed and energy intake also increase. The effect of portion size is seen not only under controlled conditions in the laboratory but also in more naturalistic settings, such as a restaurant (12) and a movie theater (13). Furthermore, the effect persists beyond a single meal and is sustained from meal to meal over 2 d (14).
The influence of energy density on energy intake has also been shown in several studies (15–18). When foods were reduced in energy density while maintaining their palatability, the study participants tended to eat a consistent weight of the available foods (19–21). As a result, the decrease in energy density led to a decrease in energy intake. Of particular relevance to the present study is that the effect of reductions in energy density on intake was sustained over several days (19, 20).
Because both the portion size and energy density of foods can affect energy intake, a critical issue is to determine how they work together. One previous study showed that increases in both the portion size and energy density of a single food led to independent increases in energy intake during a meal (22). The present study investigated the combined effects of portion size and energy density on energy intake by extending the manipulations beyond a single food to a range of commonly consumed foods that were served across multiple meals for 2 d. We hypothesized that decreases in portion size and energy density would reduce energy intake and that these influences would act independently.
SUBJECTS AND METHODS
Experimental design
The present study used a crossover design; each subject participated in four different experimental conditions that were ≥1 wk apart. In each of the 4 sessions, the subjects were provided with all their meals and snacks for 2 consecutive days. Across the 4 sessions, all foods that were served were varied between a standard level (100%) and a reduced level (75%) of both portion size and energy density (Table 1). The same 2 daily menus with the same food items were served during each session; only the portion sizes and energy density of the foods were changed. Water was served as the only beverage at all meals, except for the additional choice of tea or coffee at breakfast; the portion size and energy density of these noncaloric beverages was not changed. Each daily menu included 3 main meals, which were served in the laboratory, and an evening snack, which was packaged for consumption at home. The order of presenting the 4 experimental conditions was counterbalanced across the subjects. In addition, the order of presenting the 2 daily menus within each condition was counterbalanced across the subjects. All foods and beverages were consumed ad libitum.
TABLE 1.
Total weight and mean energy density of food items served in the 4 experimental conditions
| Energy density condition
|
||
|---|---|---|
| Portion size condition | 75% | 100% |
| 75% | ||
| Food weight (g/d) | 1530 | 1530 |
| Food energy density (kcal/g) | 1.61 | 2.11 |
| 100% | ||
| Food weight (g/d) | 2040 | 2040 |
| Food energy density (kcal/g) | 1.61 | 2.11 |
Subjects
Women aged 19–45 y were recruited by flyers and advertisements in local newspapers. Potential subjects were interviewed by telephone to determine whether they met the following inclusion criteria for the study: they were not following a diet to lose or gain weight, were not in athletic training, were not pregnant or breastfeeding, were not receiving medications known to affect appetite or food intake, did not smoke, regularly ate 3 meals daily, and had no food allergies or restrictions. Potential subjects came to the laboratory to have their height and weight measured and to complete the following questionnaires: the short form of the Eating Attitudes Test (23), which evaluates symptoms of disordered eating; the Zung self-rating scale (24), which assesses indicators of depression; and the Eating Inventory (25), which evaluates dietary restraint, disinhibition, and hunger. Subjects who had a body mass index (in kg/m2) <18 or >40, scored ≥40 on the Zung self-rating scale or ≥20 on the Eating Attitudes Test, or disliked any of the entrées to be served at the meals were not included in the study. Twenty-five women were enrolled in the study, but one was excluded for not attending a scheduled meal. Thus, a total of 24 women completed the study; their characteristics are shown in Table 2. All study procedures were approved by the Office for Research Protections of The Pennsylvania State University. The subjects were paid for their participation.
TABLE 2.
Subject characteristics1
| Characteristic | Values |
|---|---|
| Age (y) | 21.9 ± 0.7 (19–35) |
| Height (m) | 1.66 ± 0.01 (1.5–1.8) |
| Weight (kg) | 62.4 ± 1.8 (49–88) |
| BMI (kg/m2) | 22.6 ± 0.6 (18–32) |
| Energy requirement (kcal/d)2 | 2215 ± 29 (1970–2550) |
| Dietary restraint score3 | 6.5 ± 1.0 (0–17) |
| Disinhibition score3 | 4.7 ± 0.6 (0–10) |
| Hunger score3 | 4.3 ± 0.5 (1–9) |
Menus and foods
For the study, we developed 2 daily menus (Table 3) consisting of commonly consumed foods that could be manipulated in energy density. The energy density of the standard versions of the foods was chosen to be similar to commercially available items; the energy density of the reduced versions of the foods was decreased by a mean of 25% from the standard versions. Energy density was reduced either by substituting one version of a commercial product for another or by changing the ingredients in recipes (ie, by replacing full-fat ingredients with low-fat ingredients, reducing the amount of fat, and increasing the proportion of vegetables or fruit). Because dietary fat makes a substantial contribution to energy density, the energy density manipulation for most of the foods involved a reduction in fat content. The mean fat content for all foods served over the 2-d sessions was 42% of energy in the standard energy density condition and 26% of energy in the reduced energy density condition. The respective mean protein contents were 13% and 16%, and the respective carbohydrate contents were 45% and 58%.
TABLE 3.
Portion size and energy density of food items served in the 2 daily menus1
| Energy density
|
Energy density
|
||||
|---|---|---|---|---|---|
| Menu A (100% portion sizes)2 | 75% condition | 100% condition | Menu B (100% portion sizes)2 | 75% condition | 100% condition |
| kcal/g | kcal/g | ||||
| Breakfast | Breakfast | ||||
| Blueberry muffin (184 g) | 2.03 | 2.60 | Coffee cake (165 g) | 2.83 | 3.60 |
| Strawberry yogurt (227 g) | 0.50 | 1.00 | Canned peaches (140 g) | 0.48 | 0.79 |
| Lunch | Lunch | ||||
| Vegetable pizza (466 g) | 1.85 | 2.34 | Turkey sandwich (350 g) | 2.04 | 2.63 |
| Tossed salad (200 g) | 0.80 | 1.04 | Potato chips (42 g) | 4.29 | 5.71 |
| Chocolate chip bar (67 g) | 3.74 | 4.68 | Brownie (67 g) | 3.22 | 4.07 |
| Dinner | Dinner | ||||
| Mexican casserole (700 g) | 1.09 | 1.44 | Baked pasta (700 g) | 1.19 | 1.64 |
| Tortilla chips (42 g) | 3.93 | 4.64 | Green beans (115 g) | 0.36 | 0.44 |
| Salsa (90 g) | 0.33 | 0.44 | Garlic bread (51 g) | 2.70 | 3.40 |
| Ice cream (160 g) | 1.64 | 2.21 | Blueberry pie (133 g) | 2.21 | 2.87 |
| Evening snack | Evening snack | ||||
| Cheese and crackers (89 g) | 3.55 | 4.38 | Cheese and crackers (89 g) | 3.55 | 4.38 |
| Grapes (245 g)3 | 0.67 | — | Grapes (245 g)3 | 0.67 | — |
| Raisins (50 g)3 | — | 3.25 | Raisins (50 g)3 | — | 3.25 |
n = 24 women. Details of recipes, foods, and commercial sources are available from the authors on request. For beverages, 1 L water was served at all meals, and a choice of tea or coffee was also served at breakfast.
In the 75% portion size conditions, the weight of the food served was reduced by 25%.
The weight and energy density of the grapes and raisins were not included in the analyses.
For the mixed dishes, it was relatively straightforward to change the recipes to achieve a 25% reduction in energy density. The 6 entrées, which provided 59% of the total energy served to the subjects, had reductions in energy density that ranged from 21–27%. For some commercial products, however, no alternate versions with a 25% difference in energy density were available; thus, for 3 foods (tortilla chips, canned peaches, and yogurt), the product with a reduction in energy density closest to 25% was used. For the evening snack, the subjects were provided with raisins in the standard energy density conditions and grapes in the reduced energy density conditions. Because these 2 items differed greatly in energy density (3.25 compared with 0.67 kcal/g), the same portion sizes could not be used for both. Instead, equivalent amounts of energy of the 2 items were provided to the subjects (160 kcal in the standard portion size conditions, corresponding to 4% of the total energy served). The weight and energy density of the raisins and grapes were not included in the analyses of 2-d intakes.
The standard portion size of each food item was selected so that a 25% reduction would still provide an adequate weight of food. We ensured that in the condition with both reduced portion size and reduced energy density, sufficient energy was served to meet the estimated daily requirements of all subjects. The amount of energy served in a given condition depended on the magnitude of both portion size and energy density (Table 1). In 2 of the conditions (standard portions with reduced energy density and reduced portions with standard energy density), the subjects were served the same amount of energy (3250 kcal/d). A comparison of the intakes in these 2 conditions allowed an examination of the effects of energy density and portion size without variation in the amount of energy served.
Daily procedures and data collection
During each of the 2-d sessions, the subjects were instructed to eat only the foods provided by the laboratory and to drink nothing else except water or noncaloric beverages. The subjects were asked to keep their activity level similar across the 4 test sessions. Main meals were served in the laboratory and were scheduled at a specified time for each subject. Evening snacks were packaged for consumption outside of the lab; the packages and any remaining snacks were returned to the laboratory the next morning. All foods and beverages were weighed before and after meals to measure the amount consumed by the subjects to the nearest 0.1 g. Food weights were converted to nutrient intakes with the use of food-composition data from a standard reference (27) and from food manufacturers.
Immediately before and after each main meal in the laboratory, the subjects rated their hunger, fullness, and prospective consumption (how much food they thought they could eat) by using visual analog scales. For example, the subjects answered the question “How hungry are you right now?” by marking a 100-mm line that was anchored on the left by “Not at all hungry” and on the right by “Extremely hungry”. At each main meal, the subjects also used visual analog scales to rate the characteristics of the entrée and dessert (including the peaches and fruit yogurt at breakfasts). After observing the item and taking one bite, the subjects rated the serving size (compared with their usual portion), pleasantness of taste, amount of fat, and amount of energy. At each main meal, the subjects completed a brief report that asked whether they had felt ill, received any medications, or consumed any foods or caloric beverages other than those provided by the laboratory since the previous meal. Any subject who answered in the affirmative had their 2-d test session rescheduled (in practice, only one subject had a session rescheduled). At the end of the study, the subjects completed a discharge questionnaire that asked whether they noticed any differences between the sessions and what they thought the purpose of the study was.
Statistical analyses
Data were analyzed with a mixed linear model with repeated measures (SAS 9.1 for Windows; SAS Institute Inc, Cary, NC). The outcomes that were analyzed were food intake (in g), energy intake (in kcal), food energy density (in kcal/g), and ratings of food characteristics (in mm) for the entire 2-d session. A summary measure of the hunger and satiety ratings over time was produced by calculating the area under the curve for each rating across the 2 d. The fixed-factor effects in the main analyses were portion size condition and energy density condition (standard or reduced); the interaction of these 2 factors was tested for significance before examination of the main effects of the factors. A predefined comparison was made between the intakes from the 2 conditions in which equal energy was served (standard portions with reduced energy density and reduced portions with standard energy density). The factors of session order and menu order were also assessed. An analysis of covariance was used to examine the influence of subject characteristics on the relation between the experimental factors and intake. Regression analysis was used to predict 2-d intakes from food and subject variables. Results were considered significant at P < 0.05.
RESULTS
Reductions in both the portion size and the energy density of all food items that were served over 2 d led to significant and sustained decreases in energy intake. No interaction between the 2 experimental factors was observed, which indicated that their effects on intake were independent and additive.
Independent effect of portion size on intake
Decreasing the portion size of all food items significantly affected the weight of food consumed over 2 d but not the overall energy density of the food consumed (Figure 1). A 25% decrease in the available portions resulted in a mean (±SE) decrease of 10 ± 2.1% in food intake by weight, regardless of the energy density condition. As a consequence, the reduction in portion size also decreased energy intake by the same proportion ( ± SE: 10± 2.4%), which was equivalent to 231 kcal/d.
FIGURE 1.
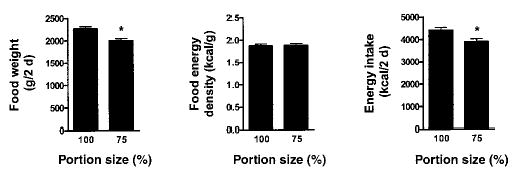
Mean (±SE) effects of food portion size, regardless of energy density condition, on the intake and energy density of the food consumed. The 24 women were served 2-d menus that varied in portion size and energy density. Data were analyzed by using a mixed linear model with repeated measures. *Significantly different from 100% portion size condition, P < 0.0001.
In the standard-portion conditions, the subjects ate a mean (±SE) 56 ± 1.2% of the available weight of food, and in the reduced-portion conditions they ate 65 ± 1.6% (P < 0.0001). Thus, although in the reduced-portion conditions the absolute amount of food eaten was smaller than in the standard-portion conditions, the proportion of the available food eaten was greater. These proportions were also reflected in energy intake; the subjects consumed a mean (±SE) 58 ± 1.3% of the available energy in the standard-portion conditions and 69 ± 1.6% in the reduced-portion conditions. In both portion conditions, however, the subjects ate substantially less food and energy than they were served. Occasionally, a subject consumed all the food provided at a breakfast or lunch meal; this occurred in 16 of 576 meals (3%).
Independent effect of energy density on intake
A decrease in the energy density of all food items had no significant effect on the weight of food consumed over 2 d but had a significant effect on the overall energy density of the food consumed (Figure 2). A 25% decrease in the overall energy density of the available food resulted in a mean (±SE) decrease of 24 ± 0.6% in the energy density of food consumed, regardless of the portion condition (P < 0.0001). As a result, the reduction in energy density also decreased energy intake by 24 ± 1.7%, which was equivalent to 575 kcal/d.
FIGURE 2.
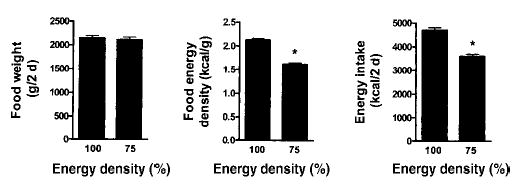
Mean (±SE) effects of food energy density, regardless of portion size condition, on the intake and energy density of the food consumed. The 24 women were served 2-d menus that varied in portion size and energy density. Data were analyzed by using a mixed linear model with repeated measures. *Significantly different from 100% energy density condition, P < 0.0001.
In both the standard- and reduced-energy-density conditions, the overall energy density of the food consumed did not differ significantly from the energy density of the available food ( ± SE: 101 ± 0.7%). Thus, daily energy intake was directly related to the reduction in the energy density of the food that was served. In both energy density conditions, the subjects consumed a mean (±SE) 64 ± 1.1% of the energy that was served to them. Similarly, the overall macronutrient content of the food consumed did not differ significantly from that of the available food (data not shown).
Combined effects of portion size and energy density
Because the effects of portion size and energy density were independent, when both were reduced simultaneously from the standard condition, the combined effects resulted in a mean (±SE) decrease in energy intake of 32.4 ± 2.0%, which was equivalent to 812 kcal/d. Portion size and energy density also had independent effects on energy intake for all the components of the main meals, ie, entrées, desserts, and all side dishes considered together (P < 0.0005 for all; data not shown). Daily energy intakes were less than the estimated requirements in the reduced-energy-density conditions and greater than the requirements in the condition of standard portion size and standard energy density (Table 4). The relation between the experimental variables and energy intake was not affected significantly by any of the measured subject characteristics (age, body mass index, or scores for depression, eating attitudes, and dietary restraint, disinhibition, or hunger). Intake of beverages, which were noncaloric and did not vary in portion size or energy density, showed no significant differences across conditions.
TABLE 4.
Intakes and energy density of the food consumed in the 4 experimental conditions1
| 75% Energy density
|
100% Energy density
|
|||
|---|---|---|---|---|
| 75% Portions | 100% Portions | 75% Portions | 100% Portions | |
| Weight of food consumed (g/2 d)2 | 1981 ± 73 | 2251 ± 76 | 2017 ± 68 | 2279 ± 67 |
| Energy density of food consumed (kcal/g)3 | 1.62 ± 0.2 | 1.62 ± 0.3 | 2.15 ± 0.3 | 2.11 ± 0.3 |
| Fat intake (% of energy intake)3 | 25 ± 0.3 | 25 ± 0.4 | 42 ± 0.3 | 42 ± 0.3 |
| Energy intake (kcal/2 d)4 | 3355 ± 114 | 3873 ± 125 | 4449 ± 145 | 4955 ± 143 |
| Energy intake (% of energy requirement)45 | 76 ± 3.0 | 88 ± 3.0 | 101 ± 3.9 | 112 ± 3.7 |
All values are ± SE. n = 24 women. No significant interaction between energy density and portion size was observed for any outcome (mixed linear model with repeated measures).
Significant main effect of portion size, P < 0.0001; no effect of energy density.
Significant main effect of energy density, P < 0.0001; no effect of portion size.
Significant main effects of portion size and energy density, P < 0.0001 for both.
Energy requirements were estimated from sex, age, height, weight, and activity level (26).
Although in 2 of the experimental conditions the same amount of energy was served, there was a significant difference in the amount of energy that was consumed between these conditions (Table 4). When the subjects were served standard portions of reduced-energy-density foods, they consumed a 12% greater weight of food than when they were served reduced portions of standard-energy-density foods. The energy density of the consumed food, however, was 25% lower. As a result, energy intake was 13% less when the subjects were served large portions of low-energy-density foods than when they were served the same amount of energy as small portions of high-energy-density food. Thus, when the same amount of energy was served, the subjects consumed less energy when the foods were of reduced energy density, even though they ate a greater weight of food.
Effects on energy intake over time
No significant differences in the mean amount of food or energy consumed or in the energy density of the foods that were eaten were observed between the 2 consecutive days of each session. In particular, the mean energy intake on the first day of each session did not differ significantly from the mean intake on the second day. When accumulated energy intake was analyzed, there was a significant difference in cumulative intake across experimental conditions at each successive meal over the 2 d (P < 0.003 for all; Figure 3). Over the course of 2 d, there was no evidence of compensation for the differences in energy intake at previous meals, and total intake continued to diverge across conditions during this time period.
FIGURE 3.
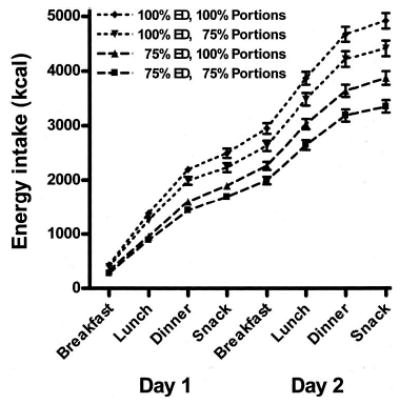
Mean (±SE) cumulative energy intakes by meal for 24 women who were served 2-d menus that varied in portion size and energy density (ED). Data were analyzed by using a mixed linear model with repeated measures. All means at a given time point were significantly different, P ≤ 0.003.
Effects on ratings of hunger, satiety, and food characteristics
The summary measure (area under the curve) of the ratings of fullness, hunger, and prospective consumption over the 2-d session did not differ significantly across conditions (data not shown). Thus, despite substantial differences in the weight and energy of food consumed across experimental conditions, there was no indication of differences in the ratings of hunger and satiety.
The subjects’ ratings of the serving size of the entrées and desserts (compared with their usual portions) differed significantly by portion size for all 12 of the items that were rated (all P < 0.0001). The mean rating of the standard portions was 63 and that of the reduced portions was 56 [SE of the difference (SED): 0.8]. The ratings of the entrées and desserts also showed some differences according to the energy density manipulation. Across all entrées and desserts, the subjects correctly rated the low-energy-dense items as having less fat than the high-energy-dense items (mean ratings: 57 compared with 61; SED: 1.0; P < 0.0001) but incorrectly rated the 2 versions as having the same energy content (mean ratings: 61 compared with 62; SED: 0.9; P > 0.05). No significant differences in the ratings of the energy or fat content of the entrées and desserts were observed between portion size conditions.
For all 6 entrées and for most desserts (4 of 6), there were no significant differences in the taste ratings between the low- and high-energy-dense versions of the food. For 2 of the desserts (the chocolate chip cookie and the brownie), the low-energy-dense versions were rated as less pleasant in taste than the high-energy-dense versions (mean ratings: 69 compared with 83; SED: 2.1; P < 0.0001).
Factors predicting intake
A regression analysis showed that the main predictors of the daily weight of food consumed were mean entrée taste rating, portion size condition, and overall hunger rating, which together accounted for 30% of the variation in food intake by weight. The only important predictor of the energy density of food that was consumed daily was energy density condition, which accounted for 81% of the variation. For the outcome of daily energy intake, energy density condition (R2 = 0 0.35), mean entrée taste rating (R2 = 0 0.10), portion size condition (R2 = 0 0.08), and overall hunger rating (R2 = 0 0.05) all were important predictors. Together, these variables accounted for 57% of the variation in daily energy intake. The subject characteristics of disinhibition score and body mass index together explained an additional 3% of the variation.
Discharge questionnaire
When asked at discharge about differences between the study sessions, 14 of the 24 women (58%) reported that portion sizes changed across the weeks. Eleven women (46%) reported that they noticed differences in the fat or energy content of some food items (potato chips, brownies, cookies, or the amount of mayonnaise in the sandwiches) across the weeks. Five women (21%) correctly discerned that a purpose of the study was to test the effect of portion size on food intake, and 3 women (13%) correctly discerned that a purpose was to test the effect of energy content on intake. Only one subject correctly discerned both of these purposes. The effect of food portion size and energy density on total energy intake was still significant (P < 0.0001) after excluding the subjects who discerned either of the purposes of the study.
DISCUSSION
The results of the present study showed that reductions in portion size and energy density independently influence energy intake when multiple foods are served and that the effects were additive and sustained over 2 d in young women who were predominantly of normal weight. These findings expand on previous research that showed that changes in both the portion size and energy density of a single food independently affected energy intake during a meal (22). In the present study, reducing the portion size of all foods by 25% resulted in a 10% decrease in both food weight intake and energy intake. Reducing the energy density of all foods by 25% resulted in a 24% decrease in both the energy density of food consumed and energy intake but did not significantly affect the weight of food consumed. When varied together, the reductions in portion size and energy density combined to decrease daily energy intake by 812 kcal (32%). These effects on energy intake were sustained from meal to meal over 2 d.
Although both the portion size and energy density manipulations influenced energy intake, there were differences in their effects. Reductions in portion size affected energy intake by decreasing the weight of food consumed, but the magnitude of the effect was not proportional to the manipulation; the percentage decrease in the weight of food that was consumed was less than one-half the original reduction in portion size. On the other hand, reducing the energy density of the food that was served resulted in the same reduction in the energy density of food consumed, with no influence on the weight of food consumed. Therefore, the magnitude of the reduction in energy intake (24%) was equivalent to the original decrease in energy density (25%).
The findings indicated that the effect of the energy density manipulation was stronger than that of portion size. A regression analysis showed that the energy density condition was the most important predictor of energy intake and accounted for more variation than the combined influence of entrée taste ratings, portion size condition, and overall hunger rating. The subjects’ characteristics explained little of the variation in energy intake across sessions and did not significantly change the effect of the experimental variables on intake; these findings might differ in a population with a greater range of age and body size. The comparison of the 2 conditions in which equal energy was served also showed that the effect of energy density on intake was stronger than that of portion size. When the 2 factors were changed simultaneously in opposite directions, energy intake was lowest when the energy density was reduced, even though the weight of food eaten was greater.
In the present study, although the subjects could eat as much as they liked and had more food available than was necessary to meet their energy requirements, the subjects spontaneously consumed 1625 kcal less over 2 d when both portion size and energy density were decreased. Despite this substantial reduction in energy intake, the subjects’ reported hunger and fullness did not differ significantly across conditions. In previous studies of manipulations of food energy density, few significant differences in reported hunger and satiety were seen despite differences in energy intake (19, 20, 28). In studies of portion size, changes in hunger and fullness were occasionally associated with the change in portions (9, 10). In one study of multiple meals, although the subjects reported an increase in fullness after eating larger portions they did not reduce their energy intake at subsequent meals (14). It appears that even if consumers report some differences in hunger and satiety as a result of food manipulations, these differences do not necessarily lead to adjustments in intake.
The manipulations of portion size and energy density of the available foods influenced the amount of energy the subjects consumed in relation to their estimated daily energy requirements. The subjects consumed more energy than their estimated requirements when the foods served were of standard energy density and standard portion size. This is of concern, because the foods offered in this condition consisted of many commonly consumed, commercially available foods. This overconsumption occurred even though no caloric beverages were consumed. Because beverages are associated with imprecise energy compensation (29), it is possible that variations in the energy density and portion size of beverages would have been associated with even greater increases in daily energy intake. In addition, few opportunities for snacking existed in the present study, and snack foods were not a major part of the manipulation. Because the consumption of energy-dense snacks has been associated with the rise in obesity rates (30), it is possible that the inclusion of more snacking opportunities would have influenced the results.
The calculations of estimated energy intakes also indicated that the subjects consumed less energy than was required in both of the reduced-energy-density conditions. Because most of the subjects in the present study were of normal weight, this could be a problem if it continued. However, the limitations of the intake of snacks and caloric beverages may have been a factor in the subjects’ underconsumption of energy. Also, although we carefully questioned the subjects before meals about their compliance with the study protocol, there was no way to be certain that they did not consume food or beverages other than those we provided.
One goal of the present study was to determine whether moderate reductions in the portion size and energy density of commonly consumed foods would be noticed and whether they would affect the acceptability of the foods. Both the subject ratings and the responses on the discharge questionnaire showed that the subjects were more aware of the portion size changes than of the energy density changes, even though the energy density manipulation had a greater effect on energy intake. The subjects noticed a change in both the portion size and the fat content of several foods, but this did not translate into a differential rating in energy content for either characteristic. For the 6 entrées, which provided most of the energy that was consumed, the manipulation of energy density did not have a significant effect on taste ratings. The energy density manipulation did, however, lead to decreased ratings of palatability for 2 of the 6 desserts. The 25% reduction in the energy density of the available foods apparently did not lead to a decrease in acceptability, because the subjects ate the same amount (ie, weight) of food in both energy density conditions.
For most of the foods, the reduction in energy density was achieved largely by reducing the fat content. Previous work has shown that the influence of fat manipulation on energy intake can be attributed primarily to its effect on energy density and that energy density affects intake even when fat content is held constant (4, 20, 28). The incorporation of water into foods, eg, through the addition of vegetables to mixed dishes, has also been associated with a reduction in energy density that leads to decreased energy intake (20, 28).
The practical implications of the present findings require additional exploration. Because reductions in portion size and energy density added together, small changes in both could be made in commonly consumed foods. The findings of the present study suggest that although consumers may have some awareness of a 25% reduction in portion size, a 25% decrease in energy density may not be noticed for many foods and may have little effect on palatability. Because reductions in the energy density of foods are both more effective in reducing energy intake and less noticeable than are reductions in portion size, decreasing energy density while maintaining portion sizes may provide an acceptable approach to help moderate energy intake. Indeed, recent research showed that encouraging overweight consumers to eat satisfying portions of low-energy-density foods was a successful dietary strategy for weight management (31, 32). In order to combat obesity, it is critical to investigate properties of foods that affect energy intake and modifications that help consumers reduce their overconsumption of energy.
Acknowledgments
We thank all the study participants and acknowledge the contributions of the staff of the Laboratory for the Study of Human Ingestive Behavior.
BJR, LSR, and JSM contributed to the conception and design of the study. JSM supervised the experiment and the data collection. LSR performed the statistical analysis. BJR and LSR interpreted the data and wrote the manuscript. None of the authors had any conflicts of interest.
Footnotes
From the Nutrition Department, The Pennsylvania State University, University Park, PA.
Supported by NIH grants DK39177 and DK59853.
Reprints not available. Address correspondence to BJ Rolls, Nutrition Department, 226 Henderson Building, The Pennsylvania State University, University Park, PA 16802-6501. E-mail: bjr4@psu.edu.
References
- 1.Ledikwe JH, Ello-Martin JA, Rolls BJ. Portion sizes and the obesity epidemic. J Nutr. 2005;135:905–9. doi: 10.1093/jn/135.4.905. [DOI] [PubMed] [Google Scholar]
- 2.Prentice AM, Jebb SA. Fast foods, energy density and obesity: a possible mechanistic link. Obes Rev. 2003;4:187–94. doi: 10.1046/j.1467-789x.2003.00117.x. [DOI] [PubMed] [Google Scholar]
- 3.Drewnowski A, Specter SE. Poverty and obesity: the role of energy density and energy costs. Am J Clin Nutr. 2004;79:6–16. doi: 10.1093/ajcn/79.1.6. [DOI] [PubMed] [Google Scholar]
- 4.Kral TV, Rolls BJ. Energy density and portion size: their independent and combined effects on energy intake. Physiol Behav. 2004;82:131–8. doi: 10.1016/j.physbeh.2004.04.063. [DOI] [PubMed] [Google Scholar]
- 5.Ello-Martin JA, Ledikwe JH, Rolls BJ. The influence of food portion size and energy density on energy intake: implications for weight management. Am J Clin Nutr. 2005;82(suppl):236S–41S. doi: 10.1093/ajcn/82.1.236S. [DOI] [PubMed] [Google Scholar]
- 6.World Health Organization. Diet, nutrition and the prevention of chronic diseases. Geneva, Switzerland: World Health Organ, 2003. [PubMed]
- 7.Dietary Guidelines Advisory Committee. Report of the Dietary Guidelines Advisory Committee on the Dietary Guidelines for Americans, 2005. http://www.health.gov/dietaryguidelines/dga2005/report/(accessed 30 June, 2005).
- 8.Rolls BJ, Morris EL, Roe LS. Portion size of food affects energy intake in normal-weight and overweight men and women. Am J Clin Nutr. 2002;76:1207–13. doi: 10.1093/ajcn/76.6.1207. [DOI] [PubMed] [Google Scholar]
- 9.Rolls BJ, Roe LS, Meengs JS, Wall DE. Increasing the portion size of a sandwich increases energy intake. J Am Diet Assoc. 2004;104:367–72. doi: 10.1016/j.jada.2003.12.013. [DOI] [PubMed] [Google Scholar]
- 10.Rolls BJ, Roe LS, Kral TVE, Meengs JS, Wall DE. Increasing the portion size of a packaged snack increases energy intake in men and women. Appetite. 2004;42:63–9. doi: 10.1016/S0195-6663(03)00117-X. [DOI] [PubMed] [Google Scholar]
- 11.Levitsky DA, Youn T. The more food young adults are served, the more they overeat. J Nutr. 2004;134:2546–9. doi: 10.1093/jn/134.10.2546. [DOI] [PubMed] [Google Scholar]
- 12.Diliberti N, Bordi P, Conklin MT, Roe LS, Rolls BJ. Increased portion size leads to increased energy intake in a restaurant meal. Obes Res. 2004;12:562–8. doi: 10.1038/oby.2004.64. [DOI] [PubMed] [Google Scholar]
- 13.Wansink B, Park SB. At the movies: how external cues and perceived taste impact consumption volume. Food Qual Prefer. 2001;12:69–74. [Google Scholar]
- 14.Rolls BJ, Roe LS, Meengs JS. Larger portion sizes lead to a sustained increase in energy intake over two days. J Am Diet Assoc (in press). [DOI] [PubMed]
- 15.Poppitt SD, Prentice AM. Energy density and its role in the control of food intake: evidence from metabolic and community studies. Appetite. 1996;26:153–74. doi: 10.1006/appe.1996.0013. [DOI] [PubMed] [Google Scholar]
- 16.Yao M, Roberts SB. Dietary energy density and weight regulation. Nutr Rev. 2001;59:247–58. doi: 10.1111/j.1753-4887.2001.tb05509.x. [DOI] [PubMed] [Google Scholar]
- 17.Rolls BJ, Drewnowski A, Ledikwe JH. Changing the energy density of the diet as a strategy for weight management. J Am Diet Assoc. 2005;105:98–103. doi: 10.1016/j.jada.2005.02.033. [DOI] [PubMed] [Google Scholar]
- 18.Drewnowski A, Almiron-Roig E, Marmonier C, Lluch A. Dietary energy density and body weight: is there a relationship? Nutr Rev. 2004;62:403–13. doi: 10.1111/j.1753-4887.2004.tb00012.x. [DOI] [PubMed] [Google Scholar]
- 19.Bell EA, Castellanos VH, Pelkman CL, Thorwart ML, Rolls BJ. Energy density of foods affects energy intake in normal-weight women. Am J Clin Nutr. 1998;67:412–20. doi: 10.1093/ajcn/67.3.412. [DOI] [PubMed] [Google Scholar]
- 20.Rolls BJ, Bell EA, Castellanos VH, Chow M, Pelkman CL, Thorwart ML. Energy density but not fat content of foods affected energy intake in lean and obese women. Am J Clin Nutr. 1999;69:863–71. doi: 10.1093/ajcn/69.5.863. [DOI] [PubMed] [Google Scholar]
- 21.Stubbs RJ, Johnstone AM, Harbron CG, Reid C. Covert manipulation of energy density of high carbohydrate diets in ‘pseudo free-living’ humans. Int J Obes. 1998;22:885–92. doi: 10.1038/sj.ijo.0800676. [DOI] [PubMed] [Google Scholar]
- 22.Kral TVE, Roe LS, Rolls BJ. Combined effects of energy density and portion size on energy intake in women. Am J Clin Nutr. 2004;79:962–8. doi: 10.1093/ajcn/79.6.962. [DOI] [PubMed] [Google Scholar]
- 23.Garner DM, Garfinkel PE. The Eating Attitudes Test: an index of the symptoms of anorexia nervosa. Psychol Med. 1979;9:273–80. doi: 10.1017/s0033291700030762. [DOI] [PubMed] [Google Scholar]
- 24.Zung WWK. Zung self-rating depression scale and depression status inventory. In: Sartorius N, Ban TA, eds. Assessment of depression. Berlin, Germany: Springer, 1986:221–31.
- 25.Stunkard AJ, Messick S. The three-factor eating questionnaire to measure dietary restraint, disinhibition, and hunger. J Psychosom Res. 1985;29:71–83. doi: 10.1016/0022-3999(85)90010-8. [DOI] [PubMed] [Google Scholar]
- 26.Food and Nutrition Board, Institute of Medicine. Dietary reference intakes for energy, carbohydrate, fiber, fat, fatty acids, cholesterol, protein, and amino acids. Washington, DC: The National Academies Press, 2002. [DOI] [PubMed]
- 27.US Department of Agriculture, Agricultural Research Service. USDA National Nutrient Database for Standard Reference, Release 17. 2004. Internet: http://www.nal.usda.gov/fnic/foodcomp (accessed July 6, 2005).
- 28.Bell EA, Rolls BJ. Energy density of foods affects energy intake across multiple levels of fat content in lean and obese women. Am J Clin Nutr. 2001;73:1010–8. doi: 10.1093/ajcn/73.6.1010. [DOI] [PubMed] [Google Scholar]
- 29.DellaValle DM, Roe LS, Rolls BJ. Does the consumption of caloric and non-caloric beverages with a meal affect energy intake? Appetite. 2005;44:187–93. doi: 10.1016/j.appet.2004.11.003. [DOI] [PubMed] [Google Scholar]
- 30.Zizza C, Siega-Riz AM, Popkin BM. Significant increase in young adults’ snacking between 1977–1978 and 1994–1996 represents a cause for concern! Prev Med. 2001;32:303–10. doi: 10.1006/pmed.2000.0817. [DOI] [PubMed] [Google Scholar]
- 31.Rolls BJ, Roe LS, Beach AM, Kris-Etherton PM. Provision of foods differing in energy density affects long-term weight loss. Obes Res. 2005;13:1052–60. doi: 10.1038/oby.2005.123. [DOI] [PubMed] [Google Scholar]
- 32.Ello-Martin JA, Roe LS, Rolls BJ. A diet reduced in energy density results in greater weight loss than a diet reduced in fat. Obes Res. 2004;12:A23 (abstr). [Google Scholar]