

Abstract
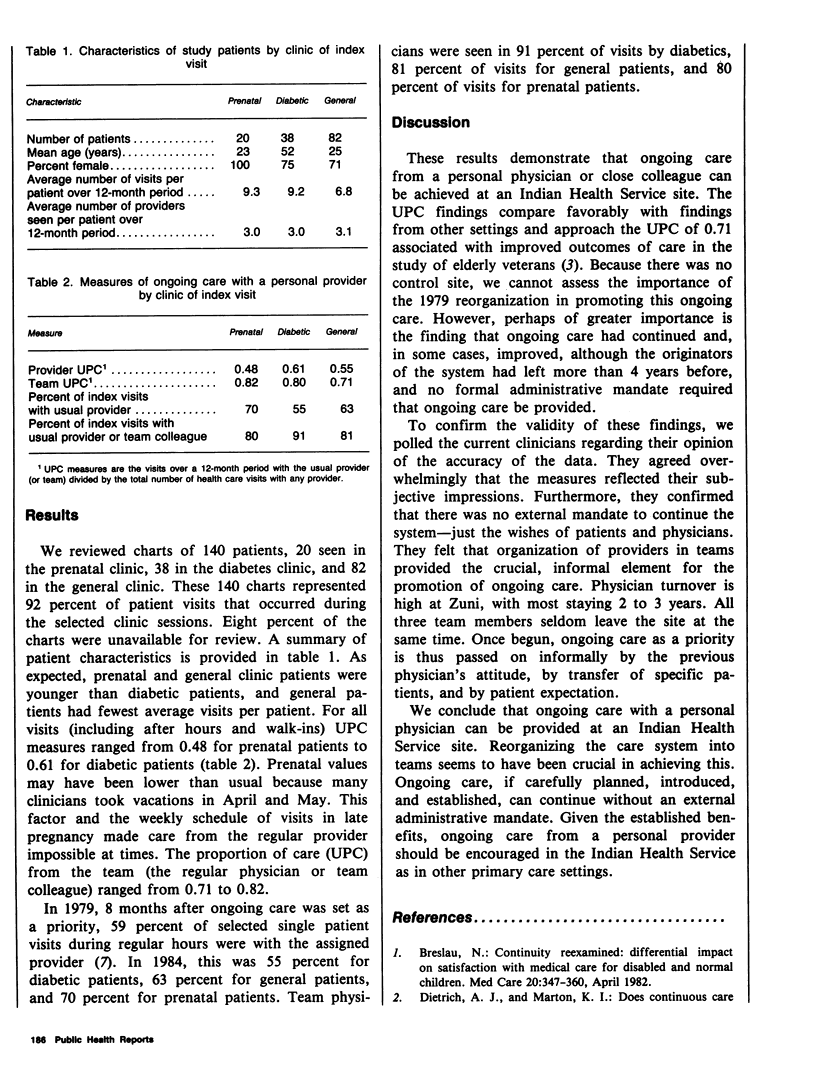
In 1979, continuing care from a personal physician was identified as a priority at the Indian Health Service site in Zuni, NM, a rural hospital and ambulatory care center serving 7,000 Zuni people. To encourage such care, a system was established that assigned each patient to a regular physician and organized physicians into teams. Three teams, each consisting of three clinicians and other support personnel, served specific geographic regions of the village. Five years later, the ongoing care provided for active randomly selected prenatal, diabetic, and general clinic patients was evaluated. The physician staff of the site had gone through a complete turnover during the previous five years. Based on a chart review for the year prior to patient identification, patients saw their regular physician from 48 to 61 percent of the time in all their visits, and their regular physician or his or her team colleague from 71 to 82 percent of the time in all their visits. Ongoing care from a personal physician or close colleague can be achieved in the Indian Health Service. Organization of physicians into teams appeared to be the critical element in promoting ongoing care at this site where physician turnover is high. Team physicians seldom all leave at once, and ongoing care as a priority is passed on by the attitude of other team physicians, by transfer of specific patients, and by patient expectation. Given the established benefits, ongoing care from a personal provider should be encouraged in the Indian Health Service as in other primary care settings.
Full text
PDF
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Breslau N. Continuity reexamined: differential impact on satisfaction with medical care for disabled and normal children. Med Care. 1982 Apr;20(4):347–360. [PubMed] [Google Scholar]
- Breslau N., Haug M. R. Service delivery structure and continuity of care: a case study of a pediatric practice in process of reorganization. J Health Soc Behav. 1976 Dec;17(4):339–352. [PubMed] [Google Scholar]
- Breslau N., Reeb K. G. Continuity of care in a university-based practice. J Med Educ. 1975 Oct;50(10):965–969. doi: 10.1097/00001888-197510000-00006. [DOI] [PubMed] [Google Scholar]
- Dietrich A. J., Marton K. I. Does continuous care from a physician make a difference? J Fam Pract. 1982 Nov;15(5):929–937. [PubMed] [Google Scholar]
- Dietrich A. J., Olson A. L. Political and cultural factors in achieving continuity with a primary health care provider at an Indian Health Service hospital. Public Health Rep. 1981 Sep-Oct;96(5):398–403. [PMC free article] [PubMed] [Google Scholar]
- Hill M., McAuley R. G., Spaulding W. B., Wilson M. Validity of the term "family doctor": a limited study in Hamilton, Ontario. Can Med Assoc J. 1968 Apr 13;98(15):734–738. [PMC free article] [PubMed] [Google Scholar]
- Patten R. C., Friberg R. Measuring continuity of care in a family practice residency program. J Fam Pract. 1980 Jul;11(1):67–71. [PubMed] [Google Scholar]
- Wasson J. H., Sauvigne A. E., Mogielnicki R. P., Frey W. G., Sox C. H., Gaudette C., Rockwell A. Continuity of outpatient medical care in elderly men. A randomized trial. JAMA. 1984 Nov 2;252(17):2413–2417. [PubMed] [Google Scholar]