

Abstract
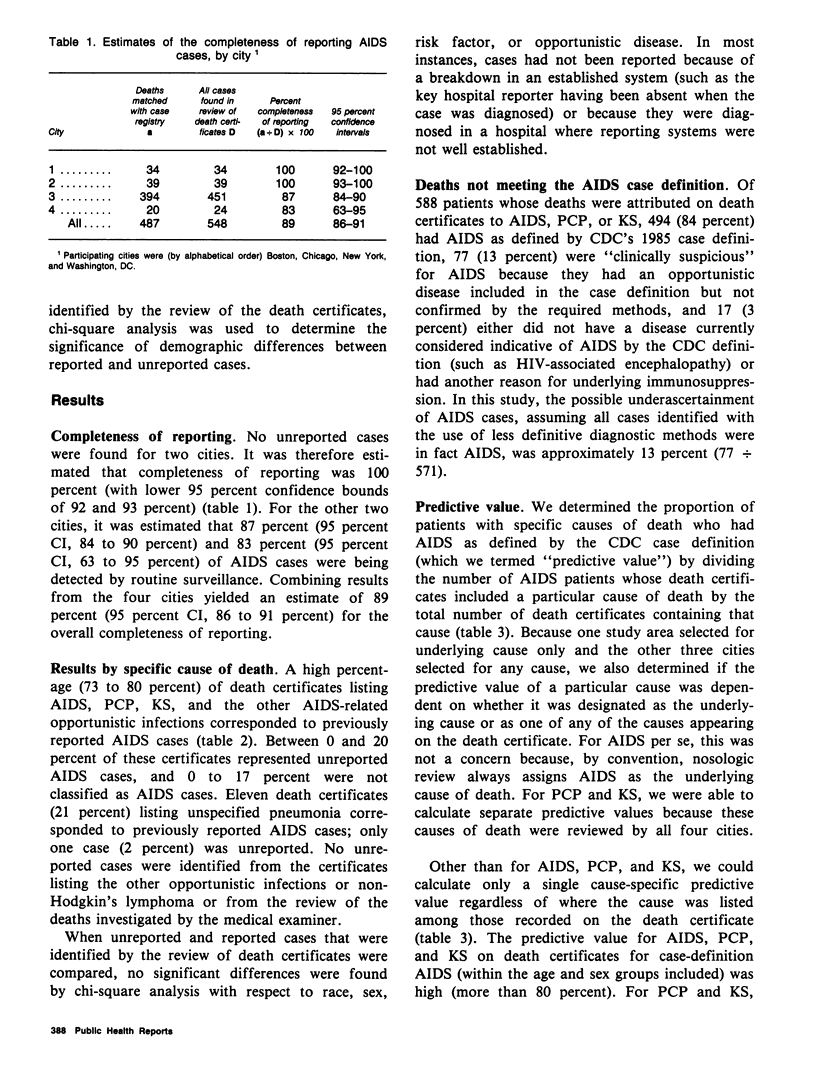
To assess the level of reporting of acquired immunodeficiency syndrome (AIDS) cases, the authors reviewed death certificates for periods of 3 months during July through December 1985 in each of four cities: Washington, DC, New York City, Boston, and Chicago. Since reporting began in 1981, these cities have reported 38 percent of all AIDS cases in the United States. Death certificates were selected and matched to the AIDS surveillance registries in each city, and medical records of those not on the AIDS registry were reviewed to determine if AIDS had been diagnosed. The estimated completeness of AIDS case reporting to AIDS surveillance systems was high in all four cities (ranging from 83 percent to 100 percent). The unreported cases were similar to reported cases with respect to sex, race, risk factor, and specific diagnosis. Of the causes of death examined, AIDS, Pneumocystis carinii pneumonia, and Kaposi's sarcoma were predictive of AIDS as defined by the CDC case definition. However, 77 of 588 deaths (13 percent) attributed to 1 of these 3 causes occurred in cases that were presumptively AIDS but did not meet the diagnostic requirements to be classified as AIDS for reporting purposes. A review of death certificates provides an easy and rapid means of evaluating surveillance efforts and can be a useful adjunct to other methods of surveillance for AIDS.
Full text
PDF



Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Chamberland M. E., Allen J. R., Monroe J. M., Garcia N., Morgan C., Reiss R., Stephens H., Walker J., Friedman S. M. Acquired immunodeficiency syndrome in New York City. Evaluation of an active surveillance system. JAMA. 1985 Jul 19;254(3):383–387. [PubMed] [Google Scholar]
- Kimball A. M., Thacker S. B., Levy M. E. Shigella surveillance in a large metropolitan area: assessment of a passive reporting system. Am J Public Health. 1980 Feb;70(2):164–166. doi: 10.2105/ajph.70.2.164. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Marier R. The reporting of communicable diseases. Am J Epidemiol. 1977 Jun;105(6):587–590. doi: 10.1093/oxfordjournals.aje.a112424. [DOI] [PubMed] [Google Scholar]
- Selik R. M., Haverkos H. W., Curran J. W. Acquired immune deficiency syndrome (AIDS) trends in the United States, 1978-1982. Am J Med. 1984 Mar;76(3):493–500. doi: 10.1016/0002-9343(84)90669-7. [DOI] [PubMed] [Google Scholar]
- Vogt R. L., LaRue D., Klaucke D. N., Jillson D. A. Comparison of an active and passive surveillance system of primary care providers for hepatitis, measles, rubella, and salmonellosis in Vermont. Am J Public Health. 1983 Jul;73(7):795–797. doi: 10.2105/ajph.73.7.795. [DOI] [PMC free article] [PubMed] [Google Scholar]