

Abstract
The Institute of Medicine stressed the need for continuous healing relationships, yet the delivery of health care has traditionally been confined to the physician office or hospital. We implemented an eHealth application tightly integrated with our electronic medical record system that provides patients with a convenient, continuously available communication channel to their physician’s office. Patients can view summary data from their medical record, including the results of diagnostic tests, and request medical advice, prescription renewals, appointments, or updates to their demographic information. We have found that patients embrace this new communication channel and are using the service appropriately. Patients especially value electronic messaging with their physicians and timely access to their test results. While initially concerned about an increase in work, physicians have found that use of electronic messaging can be an efficient method for handling non-urgent communication with their patients. Online tools for patients, when integrated with an electronic medical record, can provide patients with better access to health information, improve patient satisfaction, and improve operational efficiency.
INTRODUCTION
The Palo Alto Medical Foundation (PAMF), located in the San Francisco Bay Area, is a 500-physician multi-specialty group practice with over 1.5 million outpatient visits per year. It is an affiliate of Sutter Health system, a large nonprofit health system located primarily in California with 26 hospitals and over 5000 affiliated physicians.
PAMF has been operating with a fully functioning electronic medical record (EMR) at the Palo Alto Division since 2002. In mid-2000, we convened a strategic leadership retreat involving members of the Board of Trustees to explore the demands for and opportunities from providing online services over the Internet. Driven by market demand for Internet-based services, the desire to improve access, and the pressing labor shortage at the time, PAMF decided to establish an eHealth program to provide online access to many of our patient care services. This paper describes the motivation for the program, the functionality implemented to-date, and some early results from our experience.
STRATEGIC PLANNING
Market Analysis: Demand for Online Services
Although physicians spend a considerable amount of time during an office visit providing patient education and instruction,1 patients’ information needs are often not satisfied during the limited time spent with the physician.2 In order to satisfy patients’ information needs and engage them as partners in their care, better methods of providing information to them are needed.3 In September, 2001, a government agency estimated that 54% of the US population were using the Internet and 35% were searching for health information.4 The growing prevalence and use of the Internet by all segments of the population makes it an ideal medium for providing continuous care for patients, as espoused by the Institute of Medicine.5
Major eHealth market-research firms and others have shown a large demand for access to online health services, particularly when operated by health-care provider groups. In one survey by Jupiter Media Metrix in 1999, the top five online services desired by patients included: requesting appointments, requesting prescription renewals, viewing lab test results, viewing drug and disease information, and asking doctors treatment questions. In another survey, conducted by Harris Interactive in 2000, of 1000 consumers who were already searching for health information online, 84 percent of the respondents expressed a desire to receive electronic alerts (e.g., flu vaccine, health maintenance reminders) from their physicians. Eighty-three percent (83%) wanted to have access to lab test results online, 80 percent wanted to have “personalized information after an office visit”, 69 percent wanted to view their charts online, and 43 percent were willing to select physicians based on the availability of Internet services. Patients’ access to their medical record has been shown to improve patient-physician communication 6,7 and to improve patients’ understanding of their medical issues causing them to change their health behavior.8 Other studies have shown how use of Internet technologies can extend care to the home with an improvement of patient outcomes.9,10
In order to further characterize the perceived needs of our local patient population, and to develop an initial market segmentation for our new service, we conducted several focus groups using an external facilitator to explore patient perceptions about online services. We drew several conclusions from our focus groups: 1) young, healthy consumers with little or no regular contact with health-care providers have a relatively low demand for online health-care services; 2) older patients (over 65 years old) with multiple medical problems and less familiarity with Internet applications prefer face-to-face office visits over electronic encounters, but over time, they expect that more communication will be done online; and 3) middle-aged, busy professionals were the most interested in online health-care services because they placed a premium on convenient and efficient use of their time. Based on the results of our literature review and focus groups, we targeted patients 40 to 65 years of age to participate in our initial development and testing phases of the project.
Organizational Need for Process Improvements
In addition to consumer demand for online services, PAMF had a desire to replace some of the traditionally cumbersome, paper-based operational procedures with technology-enabled processes that require fewer steps, fewer resources, and produce faster turnaround time for patients. The prescription renewal procedure is a clear example of a cumbersome process – something that could take as long as two days to complete in the paper world – that could be improved upon. Before the project, the patient’s pharmacy faxed a renewal request to the clinic pharmacy where it was transcribed into the clinic pharmacy’s software program, printed out and sent to the physician’s medical assistant (MA) via inter-departmental mail. The MA requested the patient chart and placed the prescription renewal request and patient chart on the physician’s desk for approval. After approval, the MA called the pharmacy, who then filled the prescription and notified the patient. Due to the slow turnaround time, patients often called in a second time to check the status of their renewal requests, contributing to long telephone queues. Patient dissatisfaction with telephone access, the turnaround times for prescription renewal requests, and a limited labor pool to service the demand acted as drivers for automating the process. Thus, offering eHealth services provided an opportunity to address some operational issues in addition to providing new services.
FUNCTIONALITY
Defining the Functional Requirements for an eHealth Application
We used the information from available surveys about consumer demand for online health services as well as results from our own focus group to develop a list of strategic objectives for our eHealth initiative. We decided to focus our initial efforts on the following functions:
- Access health summary from the medical record
- View test results
- Ask medical advice from physicians and advice nurses
- View and request prescription renewals
- View and request new appointments
- Update demographic information
- Access physician-endorsed health information resources
Early on, we identified a clear critical success factor: in order for physicians to adopt online communication with patients, the workflow associated with the additional communication channel must be fully integrated with existing communications workflows. In our case, since we were already using an EMR for office-based and telephone-based communications, it was mandatory for the online communication channel to dovetail with our EMR workflows. Somewhat fortuitously, the vendor of our EMR, Epic Systems (Madison, WI) was developing an eHealth application, MyChart, which integrates with their EMR application. We chose to work with the vendor to specify and enhance their evolving application as a co-development effort. The result of our efforts was an integrated eHealth application that fits the workflow requirements described above, and which we named PAMFOnline (www.pamfonline.org). In the first release of PAMFOnline, we were able to implement all of the initial strategic functional requirements we set for the project. Figure 1 displays the health summary for a test patient, containing the diagnoses, medications, allergies, health maintenance schedule, and immunizations.
Figure 1.

Health Summary (partial view) in PAMFOnline
From a security perspective, all communications with the Internet-based secure web server are encrypted using 128-bit SSL encryption, and all accesses are logged in the audit log. Caching on the browser is programmatically disabled and there is an automatic timeout for the login.
EARLY EXPERIENCE WITH PAMFONLINE
We announced the general release of PAMFOnline to our patients in January, 2002, and have had a steady enrollment stream since, with over 12,000 patients now using the system. The mean age is 52 years old, which is approximately the midpoint of our anticipated 40–65 year-old target population. We were encouraged that although we expected older patient to adopt the technology later, currently 26% of PAMFOnline enrollees are over 60 years of age and 10% are over 70 years old.
All of the functions, except for clinical messaging with physicians and advice nurses, are provided without charge. The number of messages sent to a clinician (either an advice nurse or physician) constitutes approximately one-half of the messages received (see Figure 2). From the start of our strategic planning process, we had set a policy that professional services rendered by clinicians would be compensated by some form of revenue to offset the professional costs of delivering the services. We decided to adopt a subscription model to recover part of the costs for delivering the service and set a nominal fee that we believed would not impede access to service.
Figure 2.
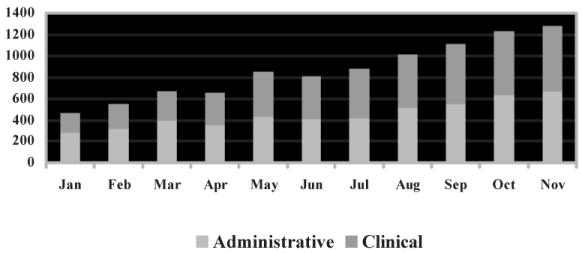
Distribution of Patient Messages
We conducted a patient satisfaction survey nine months after general release. The online survey was sent to 5233 users, of which 914 responded (18%). The gender was approximately equally split (51% male and 49% female). Thirty-three percent (33%) of the survey respondents were over the age of 60, consistent with their significant representation among PAMFOnline users.
Overall, 73% were satisfied with the existing functionality. The majority of users ranked viewing lab test results from their electronic medical record as the most important benefit of PAMFOnline, consistent with the experience of others.11 Figure 3 shows the distribution of patient rankings of other existing features. Note that the highest rated service, online messaging with clinicians, was only accessible to those who subscribed to the messaging service.
Figure 3.
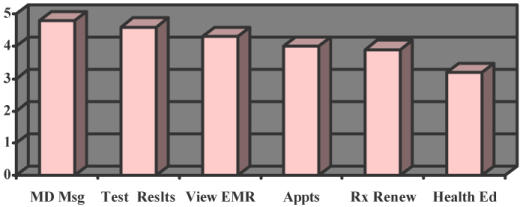
Patient Rankings of Existing Features (1–5, 5 = extremely important)
In the comment section of the survey, one of the most common requests was to increase the amount of information exposed from the EMR, especially more lab test results. At the time of the survey, sharing past lab test results (results posted before PAMFOnline was implemented) with patients required an action by the physician. In response to the survey results, we have programmatically released historical lab test results. In addition, we have implemented automated ways to release the test results after the physician has had time to review the results. This has been greeted with enthusiastic support from our users.
Resource Utilization
We saw great potential for shifting some telephone-based, and later office-based, encounters to electronic encounters through PAMFOnline – improving access and making it more convenient for our patients.
Although we noted some initial hesitancy among our busy physicians about the possibility of creating additional demand for their time by opening up another communication channel for patients, no excess demand has materialized. In fact, we have observed a decrease in telephone encounters and office visits based on preliminary analysis of utilization by patients enrolled in PAMFOnline compared with their pre-enrollment utilization history. We will continue to evaluate the impact on resource utilization over time.
Physician Acceptance
We conducted a survey of our initial 19 physicians participating in the beta testing phase of PAMFOnline and found that 92% of the 13 respondents were satisfied with the use of PAMFOnline, 100% felt that using PAMFOnline to respond to patients was the same or faster than using the phone, and 92% felt that patients’ use of PAMFOnline was what they expected, or less. Physicians also reported that PAMFOnline reduced the time required to respond to patients who used to call them frequently.
Improving Operational Efficiency
One of the advantages of requesting services online is that the requests can be automatically directed to personnel who can best handle them. Appointment requests are routed to a scheduling pool. All clinical requests (e.g., prescription renewal, lab test questions, medical advice) are directed to a pool of advice nurses. Most requests or questions can be handled by an advice nurse or can be managed using a protocol. If needed, advice nurses forward messages on to the appropriate physician.
Compared to the cumbersome paper methods of processing prescription renewal requests, use of the electronic medical record and PAMFOnline combined simplified the time-consuming tasks described earlier to one where the patient’s online request for a prescription renewal is sent directly to an advice nurse and, in many cases, on to the pharmacy via the EMR after approval, shortening a 1–2 day turnaround time to a matter of hours. The patient is notified automatically via PAMFOnline once the renewal request has been approved.
Enhanced Patient Education
One of the concerns that arises when releasing more detailed information from the EMR to the patient is that it may lead to more questions and, potentially, more concern or anxiety.6 This is particularly true of unfamiliar terms and phrases contained in test results. In order to address this proactively, we worked with Sentius (Palo Alto, CA), to apply their dynamic hyperlink technology, RichLink, to content presented within PAMFOnline. RichLink works by dynamically processing HTML documents to create a hyperlink for each word or phrase it recognizes from its Meta-Dictionary. In the Meta-Dictionary, we have created mappings between words, phrases, and synonyms to physician-endorsed content. It is well known that, although patients and consumers are searching the Internet for health information, they prefer to receive information from their physicians, especially if it is tailored to their particular situation.12
SOME CHALLENGES
One of our biggest initial challenges was to efficiently process the enrollment requests. Because our application gives patients access to information from their medical record, we considered each application to enroll in PAMFOnline as a request for release of medical information. Accordingly, we required authentication of the signature on each user agreement, either in person or by comparing the submitted signature with the registration signature on file. After the signature was authenticated, a 25-character access code was mailed to the patient at the address on file. Because of the delay between applying for an access code and its receipt, not all patients who received their codes logged in immediately to establish their private ID and password. For security reasons, access codes expire after 30 days. Consequently, for patients who tried to log in after their access codes expired, we had to re-issue another access code. As we improved our turnaround time and provided email reminders to log in, we decreased the problem of expired codes.
Although the integration of the eHealth application with our EMR provides a common infrastructure for electronic communication with patients, the clinical staff must still be trained to use the new functionality efficiently, which requires implementation staff time.
Supporting patient users (e.g., technical problems, password resets, browser incompatibilities) requires ongoing resources. For exmaple, to notify patients of new messages on PAMFOnline, we depend on an up-to-date email adddress. With the recent churning of jobs and ISPs, the number of undeliverable emails increased, requiring us to call patients to update their email addresses.
SUMMARY
Motivated by a desire to provide patients with convenient, online access to their medical record and secure communication with physicians and their staff, we implemented an eHealth application that is integrated with our electronic medical record system. The tight integration between the eHealth application and the EMR system allowed us to integrate the workflow from online messaging with that of telephone encounters and other messages (e.g., staff messages, lab test results), which is critical to clinician acceptance and efficient processing. The system has been available in general release for 18 months and feedback from patients has been very positive. We are developing new functionality to promote more interaction with patients and to create “continuous healing relationships” as part of health care delivery in the 21st century.
Acknowledgments
We thank the many people who contributed to the development and implementation of PAMFOnline, including Jill Antonidies, and Rick Gable. The PAMF EMR team, Epic developers, Sutter Health IT team, and PAMF IT department were integral to the success of this program. Importantly, the physicians and patients who help us continually enhance the system are key to evolving the system into a useful adjunct to shared care between patients and providers.
REFERENCES
- 1.Tang PC, Jaworski MA, Fellencer CA, Kreider N, LaRosa MP, Marquardt WC. Clinician information activities in diverse ambulatory care practices. Proc AMIA Annu Fall Symp. 1996:12–16. [PMC free article] [PubMed] [Google Scholar]
- 2.Tang PC, Newcomb C, Gorden S, Kreider N. Meeting the information needs of patients: results from a patient focus group. Proc AMIA Annu Fall Symp. 1997:672–676. [PMC free article] [PubMed] [Google Scholar]
- 3.Tang PC, Newcomb C. Informing patients: a guide for providing patient health information. J Am Med Inform Assoc. 1998;5(6):563–570. doi: 10.1136/jamia.1998.0050563. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.National Telecommunications and Information Administration, U.S. Dept of Commerce. A nation online: how Americans are expanding their use of the Internet. 2002. U.S. Dept of Commerce.
- 5.Committee on Quality of Health Care in America. Crossing the quality chasm: a new health system of rht 21st century. Washington, DC: National Academy Press, 2001.
- 6.Ross SE, Lin CT. The effects of promoting patient access to medical records: a review. J Am Med Inform Assoc. 2003;10(2):129–138. doi: 10.1197/jamia.M1147. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Bronson DL, Costanza MC, Tufo HM. Using medical records for older patient education in ambulatory practice. Med Care. 1986;24(4):332–339. doi: 10.1097/00005650-198604000-00004. [DOI] [PubMed] [Google Scholar]
- 8.Bronson DL, O’Meara K. The impact of shared medical records on smoking awareness and behavior in ambulatory care. J Gen Intern Med. 1986;1(1):34–37. doi: 10.1007/BF02596322. [DOI] [PubMed] [Google Scholar]
- 9.Brennan PF, Moore SM, Bjornsdottir G, Jones J, Visovsky C, Rogers M. HeartCare: an Internet-based information and support system for patient home recovery after coronary artery bypass graft (CABG) surgery. J Adv Nurs. 2001;35(5):699–708. doi: 10.1046/j.1365-2648.2001.01902.x. [DOI] [PubMed] [Google Scholar]
- 10.Goldsmith DM, Safran C. Using the Web to reduce postoperative pain following ambulatory surgery. Proc Amia Symp. 1999:780–4. 780–784. [PMC free article] [PubMed] [Google Scholar]
- 11.Cimino JJ, Patel VL, Kushniruk AW. What do patients do with access to their medical records? Medinfo. 2001;10(Pt 2):1440–1444. [PubMed] [Google Scholar]
- 12.Jones R, Pearson J, McGregor S, Cawsey AJ, Barrett A, Craig N, et al. Randomised trial of personalised computer based information for cancer patients. BMJ. 1999;319(7219):1241–1247. doi: 10.1136/bmj.319.7219.1241. [DOI] [PMC free article] [PubMed] [Google Scholar]