

Abstract
This study tests the efficacy of Structural Ecosystems Therapy (SET), a family–ecological intervention, in improving psychosocial functioning when compared with an attention–comparison person-centered condition and a community control condition. A sample of 209 HIV-seropositive, urban, low-income, African American women was randomized into 1 of the 3 conditions. Results of growth curve analyses over 5 time points revealed that SET was more efficacious than either of the control conditions in reducing psychological distress and family-related hassles. However, contrary to hypotheses, SET was not more efficacious in increasing family support. Latent growth mixture modeling analyses indicated that SET was most efficacious for women who, on average, were at or near the clinical threshold for psychological distress and for women with high levels of family hassles. Implications for further intervention development are discussed.
The emergence of new HIV cases is at an all-time high, with more than 40,000 new cases (14.7 per 100,000 individuals) reported in the United States during the year 2000 (Centers for Disease Control and Prevention [CDC-P], 2002a). African Americans, and especially African American women, are among the leading demographic groups in terms of HIV prevalence (CDC-P, 2002a, 2002b, 2002c). In 2001, African American women accounted for 64% of HIV cases reported among women (CDC-P, 2002d). Among women ages 22–44 years, the rates of HIV infection for African Americans are four times higher than the rates of Latinas and more than 16 times higher than the rates among Whites (CDC-P, 2002d).
The arrival of antiretroviral medications introduced the ability to slow the progression of HIV symptoms. As a result, interventions for HIV-seropositive individuals and their families in the United States have shifted from helping the family prepare and cope with the individual’s impending death (Goodkin, Blaney, Tuttle, & Nelson, 1996) to helping HIV-seropositive individuals and their families adapt and cope effectively with HIV as a chronic illness (Antoni et al., 2000; D. Cruess et al., 2000).
An important goal of psychosocial treatments for HIV-seropositive individuals is to reduce distress. This is important because distress is associated with progression in and worsening of HIV symptoms (S. Cruess et al., 2000). Whereas the relationship between biological and psychosocial processes in HIV is quite rich (e.g., Mulder, de Vroome, van Griensven, Antoni, & Sandfort, 1999; Pereda et al., 2000), the current study focuses only on psychosocial processes. There is evidence that life stressors, particularly everyday stressors characterized as “hassles,” are predictive of increases in psychological distress (De Jong, Van Sonderen, & Emmelkamp, 1999; Delongis, Folkman, & Lazarus, 1988). Such hassles may emanate from within the family, or they may originate from other components of the social environment.
Antoni and colleagues (Antoni et al., 2000; D. Cruess et al., 2000) have demonstrated that individually based psychosocial interventions with HIV-seropositive homosexual men can reduce distress and can inhibit the progression of HIV symptoms. However, a search of the PsycINFO and MedLine databases from 1985 through mid-2003 revealed no published randomized clinical trials of behavioral interventions to modulate psychological distress in HIV-seropositive African American women.
Because of the scarcity of empirically supported psychosocial interventions for HIV-seropositive African American women, we turned to the clinical literature for guidance. It has been suggested that individual modalities may be less efficacious with poor, inner-city African Americans (cf. pilot results reported by Markowitz, Spielman, Sullivan, & Fishman, 2000). However, there is growing sentiment that, because of the presence of multiple environmental stressors related to poverty, persistent residential mobility, racial discrimination, and inadequate access to resources, interventions for HIV-seropositive African American women should attend to the social context in addition to the individual herself (Hill & Herman-Stahl, 2002; Murray, Brown, Brody, Cutrona, & Simons, 2001). This social context includes, among others, family members, friends, neighborhood, and health care providers. The family, in particular, can be a source of support for inner-city African American women (Boyd-Franklin, 1989; Smith et al., 2001).
Clinical sources suggest that some stressors occur within the family and that reducing these family stressors may help to reduce distress (Belsky, Crnic, & Gable, 1995; Compas & Williams, 1990; Seidman et al., 1999; Shaw, Keenan, Vondra, Delliquadri, & Giovannelli, 1997). In addition to reducing family stressors, mobilizing the family as a supportive resource could be another strategy that might reduce distress by buffering the effects of stressors (Gillman & Newman, 1996; Smith & Rapkin, 1996). Adaptive family systemic processes can modulate the deleterious effects of stressors on individual family members’ psychosocial functioning (Feaster & Szapocznik, 2002). Moreover, positive relationships with family members can protect against distress in African American women (Leslie, Stein, & Rotheram-Borus, 2002).
To attend to the family and contextual realities of HIV-seropositive African American women, we developed a family–ecological intervention, Structural Ecosystems Therapy (SET; Mitrani, Szapocznik, & Robinson-Batista, 2000) to decrease family hassles and improve family support (and therefore to reduce psychological distress). This work builds on the pioneering contributions of Nancy Boyd-Franklin (Aléman, Kloser, Kreibick, Steiner, & Boyd-Franklin, 1995; Boyd-Franklin & Boland, 1995) to family systemic therapy with HIV-seropositive African American women, which attends to the woman’s social context. In this application, SET targets a selected population (i.e., individuals with HIV; Institute of Medicine, 1990) of poor, inner-city African American women. Its aim is to reduce psychosocial factors associated with progressions in HIV symptoms (cf. S. Cruess et al., 2000).
This article is the first major publication reporting the results of a randomized clinical trial investigating the efficacy of SET versus two control conditions: an attention–comparison control (person-centered approach; PCA) and a community control (CC). We test three primary hypotheses. First, SET, a family–ecological intervention, should be significantly more efficacious than either attention–comparison control or CC in reducing distress. Second, SET should decrease family hassles for the target woman significantly more than does attention–comparison control or CC. Third, SET should increase family support significantly more than does attention–comparison control or CC. In addition to testing these hypotheses, we planned to examine whether any effect of SET on psychological distress might be at least partially mediated by the effect of SET on family hassles and family support.
Method
Design
This study used a mixed design with three conditions and five assessment points. Participants were assessed at baseline, randomized to condition, and reassessed at 3, 6, 9, and 18 months postbaseline. The study used an intent-to-treat design, which requires that even participants who drop out of the intervention continue to be assessed at the appropriate time points. Participants were assigned to a condition on the basis of an urn randomization procedure (Wei & Lachin, 1988). This frequently used procedure is intended to balance the characteristics of study participants across conditions. The participant characteristics balanced in this study were age, number of psychiatric diagnoses, number of children, and prior history of drug use. At baseline, the three conditions were equivalent on these variables.
Participants
Of the 588 women initially approached about participation, 49 (8.3%) indicated that they were not interested in participating. Another 115 (19.6%) were not screened further because they were not part of the population of interest (i.e., HIV-seropositive African American adult mothers). The 424 mothers who were interested in participating and who belonged to the population of interest were then screened for inclusion and exclusion criteria. Two hundred nine were eligible for participation in the study, whereas the remaining 215 were not. To be eligible for participation, women had to meet seven inclusion and/or exclusion criteria at baseline. First, they must have not reported illicit drug use during the previous 6 months (19.8% of 424 were excluded). Second, they must have endorsed at least two interpersonal problems (including one family-related problem) on our recruitment/screening checklist (4.2% of 424 were excluded).1 Third, to exclude very severe psychiatric disorders, we excluded women who reported any prior psychiatric hospitalization (1.5% of 424 were excluded), with the exception of hospitalizations related to drug abuse. The latter were included because of the pervasiveness of drug abuse among inner-city, HIV-seropositive African American women. However, women with current or past Diagnostic and Statistical Manual of Mental Disorders (3rd ed., rev.; DSM–III–R; American Psychiatric Association, 1987) co-morbid psychiatric diagnoses, as determined by the Structured Clinical Interview for DSM–III–R (SCID; Nonpatient Version for HIV-Seropositive Persons Spitzer, Williams, Gibbon, & First, 1989; see Measures sections), were not excluded. Fourth, women must have had self-reported CD4 cell counts high enough to maximize the likelihood that they would survive through the 18-month follow-up (14.1% of 424 were excluded). At the beginning of the study, only women with self-reported CD4 cell counts above 200 were admitted for participation. However, with the introduction of protease inhibitors and the documented increase in survival rate associated with these medications, the CD4 cell count requirement was reduced from 200 to 50 for women who were using protease inhibitors. This change in inclusion criteria was instituted after approximately 60 participants had been enrolled. Fifth, because our assessments and therapy sessions were home based, we excluded women who were homeless or in a phase of institutionalization where outside contact was prohibited (3.1% of 424 were excluded). Sixth, women whom the recruiter perceived to be cognitively impaired or unable to complete the assessments were excluded from the study (0.5% of 424 were excluded). Finally, 4.2% of the 424 eligible women were excluded because they had participated in the pilot phase of our study or were currently participating in another randomized behavioral trial for HIV-seropositive women.
At baseline, the sample for this study consisted of 209 HIV-seropositive, inner-city, African American women. Table 1 presents the numbers of women by condition and time of assessment. The follow-up rates were quite high through the 9-month assessment point (90.4% at 3 months, 88.5% at 6 months, and 92.3% at 9 months). The follow-up rate at 18 months was only 63.2% because of funding constraints that did not permit us to assess all women at this final time point.
Table 1.
Sample Size by Condition and Time of Assessment
| Condition | Baseline | 3 month | 6 month | 9 month | 18 month | Total assessment |
|---|---|---|---|---|---|---|
| CC | 73 | 67 | 67 | 69 | 37 | 313 |
| PCA | 69 | 61 | 56 | 63 | 44 | 293 |
| SET | 67 | 61 | 62 | 61 | 47 | 298 |
| Total | 209 | 189 | 185 | 193 | 128 | 904 |
Note. CC = community comparison; PCA = person-centered approach; SET = structural ecosystems therapy.
For the randomized sample at baseline, the mean age of the sample was 36 years (SD = 8.0). The median annual personal income for participants was $7,000 (25th percentile $5,316, 75th percentile $10,694), and the median annual income for households was $9,672 (25th percentile $6,366, 75th percentile $14,880). With regard to the women’s marital status, 87 (42%) were never married and not cohabitating, 26 (13%) were married and living with their husbands, 20 (10%) were married but living apart from their husbands, 36 (17%) were unmarried but cohabitating, 6 (3%) were widowed, 33 (16%) were divorced, and 1 participant’s marital status was unknown. Over half of the sample (51%) reported having less than a high school education. Eighty percent (n = 167) of participants were unemployed, and 83% (n = 173) were on public assistance. The mean self-reported T-cell count in the sample at baseline was 461.6 (SD = 303.6). At baseline, the majority of the women (84%) met at least one of the DSM–III–R diagnoses measured in this study (by the SCID, Non-Patient Version for HIV-seropositive persons; see Measures section): Drug abuse or dependence (lifetime but not within the past 6 months, 64%), alcohol abuse or dependence (lifetime but not within the past 6 months, 42%), major depressive episode (lifetime, 38%; within the past month, 12%), and posttraumatic stress disorder (39%). Of the women who met criteria for substance abuse or dependence, 63% met criteria for at least one other diagnosis.
Recruitment
Participants in the study were recruited from the fall of 1996 to the spring of 1999. The women were recruited from community-based agencies that provide HIV care and other social services to HIV-seropositive individuals in South Florida. After recruitment and determining study eligibility, the recruiter arranged to obtain consent from and conduct an assessment with each woman. After explaining the study to each woman, the interviewer read and obtained informed consent. In SET, informed consent was also obtained from all individuals who participated in therapy sessions.
Intervention Conditions
The study used two types of interventions, SET (Jackson-Gilfort, Mitrani, & Szapocznik, 2000; Mitrani et al., 2000; Nelson, Mitrani, & Szapocznik, 2000), an ecosystemic and family-based therapy, and the PCA (Rogers, 1959), a nondirective individual counseling approach that was used as the attention–comparison control.
SET
SET targets social interactions, particularly those that are maladaptive, at the interfaces among the woman, her family, and the social environment (Mitrani et al., 2000). Interactions are exchanges, verbal or nonverbal, between two or more people. Family interaction patterns are repetitive verbal or nonverbal exchanges that take place between or among family members. Maladaptive family interactional patterns are repeated exchanges within the family that are experienced as aversive, that result in symptomatic behavior, or that cause family functions to go unfulfilled.
SET is an ecological extension of Brief Strategic Family Therapy (BSFT; Szapocznik & Kurtines, 1989). BSFT was designed to identify and correct maladaptive interactional patterns within the family. SET extends the principles of BSFT to apply also to relationships between the family and outside systems (e.g., health care providers). The three basic techniques in SET, derived from BSFT, are joining, diagnosing, and restructuring (cf. Minuchin & Fishman, 1981; Szapocznik, Hervis, & Schwartz, 2003; Szapocznik & Kurtines, 1989). Joining refers to the process of establishing a therapeutic system, in which the therapist is both a member and the leader. Joining is intended to create a therapeutic system that includes the woman, her family, and representatives from other relevant systems (e.g., friends, health care providers) who will be involved in the therapeutic process. Diagnosing (Szapocznik et al., 1991) refers to the identification of interactional patterns, both within the family and between the family and outside systems, that fail to meet the woman’s, and possibly her family’s, own objectives. These objectives may include the long-term well-being of the woman and her children. Diagnosis in SET, as in BSFT, looks at five major dimensions of interactional functioning: (a) structure–organization (leadership, subsystems and alliances, and communication flow), (b) developmental stage (the age-appropriateness of family members’ roles and behaviors), (c) resonance (the level of permeability of boundaries among family members and between the family and other systems which can result in enmeshed [too much permeability] or disengaged [too little permeability] interactions), (d) identified patienthood (the extent to which the HIV-seropositive woman is viewed as the cause of the family’s problems), and (e) conflict resolution (the management of problems and disagreements). Restructuring encompasses interventions that the therapist undertakes to change maladaptive interactional patterns. A broad range of techniques is used in restructuring. Some of the more frequently used restructuring strategies are the following:
Working in the present involves attending to the processes of interactions among family members or between family members and members of outside systems as they occur in the session. For example, a discussion of “who takes out the garbage,” or any other issue that emerges in the session, may be used to help a family who diffuses conflict to stay on topic. Diffusion, the act of “changing the subject” when conflict emerges, is one example of a maladaptive family pattern. SET focuses on changing these types of maladaptive family interactions in the “here and now” of therapy.
Reframing represents a strategy of cognitive restructuring that permits new and more positive interactions to emerge. For example, in the case of an HIV-seropositive woman who does not want to call her mother because “my mother only yells at me when I call her,” the cognitive frame may be shifted from “woman rejects mother” to “woman cares for mother” by suggesting that “I can understand that you would not want to call your mother under those circumstances because she is so very important to you, that when she is not accepting, it is far too painful for you to tolerate.”
Working with HIV-seropositive women typically involves two kinds of boundary shifting interventions: those intended to enlarge positive informal social support networks and linkages with formal service delivery, on the one hand, and those intended to disconnect the woman from damaging relationships (e.g., affiliations with drug-using men) on the other.
PCA (attention–comparison control)
PCA was incorporated in the study to control for common factors (Strupp & Hadley, 1979) in therapy such as attention, supportiveness, and empathy. The aim of this condition was to implement an intervention that was distinct from the central techniques and active ingredients of SET. PCA is nondirective, whereas SET is directive; PCA targets the individual, whereas SET targets the family and the ecosystems; PCA targets self, whereas SET targets family interactions; and PCA sets no goals for the client, whereas SET is strategic and directive. The focus in PCA is on the quality of the relationship between the therapist and the client, in which the therapist demonstrates empathy, unconditional positive regard, and congruence (Rogers, 1959). Empathy refers to the ability of the therapist to accurately recognize and reflect to the client his or her thoughts, feelings and meanings. Unconditional positive regard refers to the therapist’s acceptance of the client as he or she is “in the moment” and conveyance of that acceptance not by direct statements of positive regard but rather by an attitude of valuing the client and by an absence of evaluative (negative or positive) feedback to the client. Congruence, also known as genuineness, is the matching of the therapist’s internal experience and overt behavior in such a way that the client perceives the therapist as genuine and sincere. By definition, PCA does not incorporate any specific therapeutic techniques; rather, it is the therapeutic relationship that is the active ingredient. Although PCA was initially selected as an intervention to control for attention and other common factors in therapy, it was conducted as a true therapy condition. Therefore, PCA represented both an attention control and a comparison condition, thereby ultimately rendering the test of SET more rigorous.
CC
The CC condition was intended to reflect (and control for) the baseline of services that HIV-seropositive African American women receive in the local community. Women in this condition received no services from the study. However, like women in all conditions, they received referrals to outside services if these were needed.
Therapists
Requirements
Because the active intervention conditions were theoretically distinct, therapists were nested within conditions (Kazdin, 1994a, 1994b). Therapists working in the SET condition were required to have a master’s degree in counseling, social work, or marriage and family therapy and to have had at least 1 year of clinical experience, with some experience in working with families. Therapists working in the PCA condition were required to have a master’s degree in psychology, counseling, or social work, and to have had at least 1 year of clinical experience, including some individual counseling. All therapists were African American women with experience in African American culture and in counseling African Americans.
Training
Training for SET therapists was conducted using the SET treatment manual, with supplementary readings from other structural family therapy models (e.g., Minuchin & Fishman, 1981). Carleen Robinson-Batista, the most senior therapist on the SET team, initially conducted SET cases to assist in the calibration of the modality. The senior author, José Szapocznik, the SET trainer/supervisor, Victoria B. Mitrani, and Robinson-Batista met for 4 half-day workshops to discuss and review the manual. As new therapists joined the SET team, they received approximately 3 months of training. During the training, trainees also conducted cotherapy cases with Robinson-Batista and attended individual and group supervision meetings for 3 to 4 hr per week.
To prevent the bias that might occur because SET was developed at the site where the study was conducted, we made PCA training slightly more rigorous than SET training. There were three components involved in the training of the PCA therapists. First, therapists were asked to read the PCA manual designed for this study. Second, training was conducted by South Florida’s most senior and best known PCA therapist and trainer, Ted Aidman, who met with the PCA team (three therapists plus the day-to-day modality supervisor, Magaly H. Mauer) once per week during the pilot year. These weekly meetings between the PCA therapists and the trainer were held to help the therapists and modality supervisor to grow into and experience the PCA modality. Third, Barbara Brodley, a central figure in the development and refinement of PCA (e.g., Bozarth & Brodley, 1991), conducted two intensive, 3-day training workshops.
Supervision
In SET, ongoing supervision consisted of reviewing videotapes and case notes. Therapists met with the SET supervisor (Victoria B. Mitrani) weekly as a group for 2 hr. Videotapes were reviewed in the context of the supervision, according to clinical needs. If the supervisor believed that a therapist was not adhering properly to the SET model, she met weekly with that therapist for videotape and case review until she was satisfied that the therapist was again adhering to the model. Once every 2 months, the senior author served as an oversight supervisor, reviewing random tapes and providing guidance on adherence to the therapists and supervisor.
In PCA, weekly (Year 1) and biweekly (Year 2) supervision meetings were held between therapists and the PCA supervisor, Magaly H. Mauer. For quality control, on a weekly basis, the supervisor randomly selected case notes from each therapist, and on a monthly basis, she randomly selected session videotapes from each therapist for review. The supervisor identified problems with therapist adherence by watching session tapes and consulting with therapists during the supervision meetings. Adherence problems generally involved directiveness, which is proscribed in PCA. Problems were corrected in monitoring sessions using the same communication style used in PCA (i.e., empathy, unconditional positive regard, and congruence) to help the therapist to see and correct the problem herself. If that did not work, the supervisor used the training manual to point out the therapist’s mistakes. Barbara Brodley served as oversight supervisor for the PCA condition, reviewing one randomly selected videotape per month and providing phone supervision. The external supervision for PCA was twice as frequent as for SET. This was done to counteract the bias that might occur because SET was developed at the site where the study was conducted.
Adherence to treatment protocol
Therapy sessions for each of the conditions were rated for adherence or integrity to therapy protocol by independent raters who were blind to treatment condition. Therapist adherence was monitored continuously throughout the study. A total of 175 therapy sessions (95 from SET and 80 from PCA) were randomly chosen from study records. Ratings were conducted directly from videotapes of therapy sessions. Each session was divided into 20-min segments, and each 20-min segment was rated. A total of 398 20-min segments were rated (234, SET; 164, PCA). Raters identified in-session therapist interventions directly from these videotapes. Therapist interventions were operationalized using each condition’s treatment manual. Raters were initially trained to an interrater reliability coefficient of .80 with the rating supervisor (Michael S. Robbins), and were retrained every 6 months to prevent drift. The rating supervisor reviewed adherence ratings. If a rater failed to maintain an interrater reliability coefficient of .70 with the rating supervisor, the rater was suspended, additional training was implemented, and the rater was allowed to continue rating only after achieving an interrater reliability coefficient of .80 with the rating supervisor. Therapy segments were rated on (a) technique, (b) focus of therapy, and (c) directiveness of the therapist. Of the 14 techniques rated, 12 are central to SET and 2 are central to PCA. SET segments were rated significantly higher on all ratings central to SET (all ps < .01), whereas PCA segments were rated significantly higher on both ratings central to PCA (both ps < .001). The level of directiveness, the technique that is most fundamentally different between the SET and PCA conditions, was significantly different between the two conditions, F(1, 396) = 1,391.7, p < .0001. In SET, the mean level of directiveness was 3.71, corresponding to considerably directive. In PCA, the mean level of directiveness was 0.09, corresponding to not at all directive.
Procedure
All assessments and therapy sessions were conducted at the woman’s home or at another location convenient to the woman. Participants were not compensated for participation in the therapy services. However, participants were compensated for aiding in the research by providing data at each of the assessment time points. Participants were compensated $50 at baseline, 3-, 6-, and 9-month postbaseline assessments and $100 for their participation in the 18-month postbaseline assessment. Assessors and therapists contacted each woman to set and confirm appointments for each assessment or therapy session, respectively. For women in the SET condition, therapists also contacted family members to remind them to be available for therapy sessions.
For each woman, at baseline, we obtained the names, addresses, and phone numbers of three contact persons who would be likely to know the woman’s whereabouts if the assessment team was unable to locate her. In addition, women were sent birthday and holiday cards and on occasion received gifts for the holidays. Through these procedures, we were able to limit attrition to below 10% from baseline through the 9-month assessment time point.
Measures
The measures reported in this article were part of a larger assessment battery administered to participants. The average completion time for the larger battery ranged from 120 to 150 min. Because of the lengthy nature of the assessment battery, each assessment was completed in two parts. The measures of psychological distress, family hassles, and family support were all administered during the first assessment session. The measure used to characterize the populations was administered during the second assessment session, which usually occurred within 3 days of the first.
Measure to Characterize the Population
The SCID was administered at baseline and used to characterize the population. The measure was used to assess lifetime and current alcohol and drug abuse or dependence as well as lifetime or current major depression, anxiety disorder, and posttraumatic stress disorder. The SCID was administered and rated by raters trained by a SCID-qualified psychiatrist. Interrater reliability for this measure was adequate (κ = .78).
Psychological distress
The Global Severity Index from the Brief Symptom Inventory (Derogatis, 1993) was used to measure psychological distress. The Brief Symptom Inventory consists of 53 self-report items that assess the respondent’s psychological symptoms within the past 7 days. The Global Severity Index includes the following nine dimensions: (a) depression, (b) anxiety, (c) paranoid ideation, (d) psychoticism, (e) somatization, (f) interpersonal sensitivity, (g) hostility, (h) phobic anxiety, and (i) obsessive–compulsive behavior. Each item is rated on a 5-point Likert scale ranging from 1 (not at all) to 5 (extremely). The Global Severity Index is calculated by deriving an item mean response (i.e., 0–4) across the 53 items. In this study, Cronbach’s alpha for scores on the Global Severity Index was .96.
Family hassles
The Hassles Scale (DeLongis et al., 1988), revised for African American women, was used to assess daily hassles in a number of areas. In the version of the scale used in this study, we omitted items that would not be relevant to poor, urban African American women (e.g., financial investments) and added items not in the original scale that would apply to the current sample (e.g., your ex-spouse; see Smith et al., 2001). The family hassles score was obtained by counting the number of family-related hassles items that the woman had endorsed (maximum 12). Cronbach’s alpha for scores on the family hassles subscale in this sample was .68.
Family support
Family support was measured using the Social Support Questionnaire (SSQ) Short Form (Sarason, Sarason, Shearin, & Pierce, 1987). The SSQ asks the respondent to list the initials and the relationships of the individuals on whom they can depend for six different aspects of support. For each of the six different aspects of support, the respondent can list up to nine individuals. The count of the number of family members listed (across the six aspects of support) was used. The Cronbach’s alpha estimate for scores on the family support scale in the present sample is .76.
Results
Data Analytic Strategy
For each dependent variable (psychological distress, family hassles, and family support), the analytic approach comprised three planned stages.
Stage 1 analyses: Primary hypothesis test
The primary test of the hypotheses was accomplished using a mixed-model (i.e., a repeated measures between-groups design) analysis of variance (ANOVA), focusing on the Condition × Time interaction. Mixed-model methods (Littell, Milliken, Stroup, & Wolfinger, 1996) contain both a fixed effect portion (i.e., the observed predictor(s), condition, here represented as a between-subjects factor) as well as a specification of random components, which can account for the nonindependence of nested (i.e., repeated) observations. In the current study, the random effects portion of the model contains at least one person-specific error component (in general, growth curve specifications contain a person-specific component for each of the polynomial time terms—linear, quadratic, cubic, etc.), which accounts for the nesting of repeated measures within participants over time. This mixed model can also be considered as a hierarchical linear model (cf. Bryk & Raudenbush, 1992) with a random intercept (a random component that allows the intercept of the growth curve to vary across persons). The repeated measures ANOVA parameterization was chosen to avoid assigning a specific form to the time trend, thereby providing an omnibus test of difference over time. All analyses were conducted on an intent-to-treat basis. All participants were included in the analyses regardless of the number of sessions or assessments they completed. For dependent measures where baseline scores differed by condition at a conservative alpha level of .20 (Feaster et al., 2000), baseline scores were covaried and the model was estimated using data from the remaining time points. These analyses tested the hypothesis that SET was efficacious, compared with PCA and CC, for the sample as a whole and for each outcome variable.
Stage 2 analyses: Polynomial trends and dose–response relationships
For each psychosocial outcome variable, we performed Stage 2 analyses only if Stage 1 analyses revealed a significant effect of the intervention on that outcome. Stage 2 analyses included two independent components: the polynomial (i.e., linear, quadratic) decomposition of any significant time path of the intervention and the analysis of the relationship of the outcome to the amount of therapy exposure (i.e., dose). The polynomial decomposition was designed to characterize the time path of differences by condition. In this step, a growth curve specification was fit to the data. These specifications have person-specific random components associated with both the intercept and each of the (potentially multiple) slope terms. Choice of linear, quadratic or cubic growth components was determined by using the Bayesian Information Criterion (BIC; Schwartz, 1978), a measure of goodness of fit used to determine the best-fitting model to the data. For the Stage 2 analyses of the relationship of outcome to dosage, after establishing the significant polynomial components of the time path of change, we entered intervention dosage into the model to ascertain whether an endogenous (i.e., naturally occurring rather than experimentally manipulated) dose–response relationship contributed significantly to the model. These analyses (a) explored whether the differences over time could be characterized by linear, quadratic, and/or cubic trends and (b) tested whether the number of therapy contact hours (in SET and PCA) was related to the extent of change observed in each outcome within each active therapy condition.
Stage 3 analyses: Latent growth mixture modeling
The third and final stage of analysis for each psychosocial outcome was an exploratory examination of latent growth mixture models (Muthén et al., 2002; Muthén & Muthén, 1998–2003). These analyses were performed regardless of whether the primary hypothesis tests were statistically significant. This procedure examines whether there are unobserved latent classes of participants within the sample, for which the intervention was more or less successful. This analysis, then, was planned to explore whether there were any clinically important subgroups of participants that may have demonstrated different patterns of growth and, therefore, differential responses to the interventions, over time. This technique groups participants into classes based both on baseline levels of the dependent variable and on the trajectories of the growth curve over time. The estimated trajectory of growth for each of the conditions is allowed to vary within these classes, thus allowing the effectiveness of the interventions to vary by class. In these analyses, intervention condition was coded as two dummy variables. The dummy variable for PCA was assigned a score of 1 if the participant was in the PCA condition and a score of 0 (for CC) otherwise; similarly, the dummy variable for SET was assigned a score of 1 if the participant was in the SET condition and 0 (for CC) otherwise. Therefore, within each class of participants, the coefficients obtained for the SET and PCA conditions indicate the direction and degree to which each intervention differs from CC. To estimate the extent to which PCA differed from SET, we estimated another specification of this model with dummy variables for the CC and SET conditions. In this specification, the coefficients for SET and CC indicate the direction and degree to which each of these conditions differed from PCA. The BIC, in conjunction with the clinical usefulness of the classes (B. Muthén, personal communication, April 24, 2002), can be used to determine the number of classes to include within each solution. Lower values of the BIC indicate a better fitting model. A separate solution was estimated for each dependent variable.
The latent growth mixture modeling method does not deterministically assign a participant to a class; rather, it estimates the probability that a particular participant belongs to each of the classes. Thus, for these analyses individuals are assigned class membership based on the class with the largest probability. A matrix comparing the assigned class membership to the average probability of membership in each of the other classes is presented to aid in assessing the fit of the latent class model. This matrix is similar to the matrix of observed versus predicted category membership used to describe fit in ordered logistic regression. These analyses tested whether SET was differentially efficacious for empirically distinguishable groups of participants.
Mediational analyses
Mediational analyses were planned that examined whether any significant changes in family hassles or family support might have mediated the effect of the intervention on psychological distress. For each potential mediator that may be significantly affected by SET (family hassles and family support), simple growth curves from the tests of the effects of SET on the potential mediator and on psychological distress were estimated as latent growth curve analyses, and paths from the growth curve of the hypothesized mediator to the growth curve of distress were estimated. Mediation was assumed if the significance of the intervention on the parameters of the growth curve of distress was decreased to nonsignificance when the path was added from the growth curve of the potential mediator to the growth curve of distress. Note that these mediational models were estimating simple latent growth curves, not latent growth mixture models.
Comparability of Conditions
There were no significant differences by condition on demographic characteristics. Of the 209 women enrolled in the study, 136 were randomized to one of the two active treatment conditions (SET or PCA). Of the 136 women who were assigned to SET or PCA, 68% (n = 92) were successfully engaged into treatment, 75% in SET and 61% in PCA (Prado et al., 2002), with engagement defined as attendance at two or more therapy sessions. Engagement rates were not significantly different between SET and PCA, χ2(1, N = 136) = 2.59, p < .11.
On average, the women randomized to the SET condition had significantly more hours of therapy contact (M = 12.45, SD = 12.85) than did the women randomized to the PCA condition (M = 5.74, SD = 5.23), F(1, 129) = 15.24, p < .0001. This implies that SET was more successful than PCA in retaining participants in treatment. On average, SET sessions were 61.71 min (SD = 17.55) in length, whereas PCA sessions were 50.77 min (SD = 17.94), consistent with differences in practice between family therapy and individual psychotherapy. Baseline levels of psychological distress differed weakly by condition, F(2, 204) = 2.41, p < .10, and baseline levels of family hassles were significantly different by condition, F(2, 204) = 3.24, p < .05. The SET condition was associated with the highest baseline level of psychological distress and family hassles, and the CC condition was associated with the lowest baseline levels. Therefore, Stage 1 analyses, the primary hypothesis tests, for psychological distress and family hassles used the analysis of covariance (ANCOVA) specification, controlling for baseline levels of each dependent measure and analyzing the remaining time points. Family support did not differ significantly by condition at baseline, F(2, 204) = 0.94, p < .39. Therefore, the primary hypothesis test for family support used all time points.
Tests of Hypotheses
Results are presented separately for each of the three hypotheses. Within the presentation of each hypothesis, the three stages of analysis are presented in turn—Stage 1, or primary test of the hypothesis, first; Stage 2, or examination of polynomial trends and dose–response relationships, second; and Stage 3, or latent growth mixture modeling, third. Note that Stage 2 (polynomial trends and dose–response) is presented only in cases where the results of the Stage 1 analysis were statistically significant.
Hypothesis 1: Psychological Distress
Stage 1: Primary hypothesis test
In the primary mixed-model hypothesis test for psychological distress, baseline levels of distress were covaried. Because of several distinct outliers, a rank transformation was performed prior to analysis (Conover & Iman, 1981, 1982). To ensure that the rank transformation did not alter the patterns of relationships across time points, the data were ranked across all available time points rather than within time points.
The primary analysis for psychological distress revealed a significant Condition × Time interaction, F(6, 472) = 2.19, p < .05, indicating that the three conditions (SET, PCA, and CC) differed in trajectories of distress over time.2 The main effect of condition was not significant, F(2, 472) = 1.28, p < .28, although there was a significant main effect of time, F(3, 472) = 4.09, p < .007, indicating that all three conditions evidenced significant declines in distress over time. Figure 1 displays the estimated means of psychological distress from the ANCOVA specification for the rank-ordered data. Examination of the error bars in Figure 1 demonstrates that, at the 3-month assessment, the mean psychological distress score was significantly lower in the SET condition than in the CC condition. Scores in both conditions declined over subsequent assessment times, and at the 9-month assessment, the mean rank for SET remained significantly lower than the mean rank for CC and significantly lower than the mean rank for PCA. The psychological distress scores in the PCA condition were relatively stable over time. In terms of mean psychological distress score, the PCA condition ranked between SET and CC (and not significantly different from either) at 18 months. The mean rank for SET remained significantly lower than did the mean rank for CC at 18 months.
Figure 1.
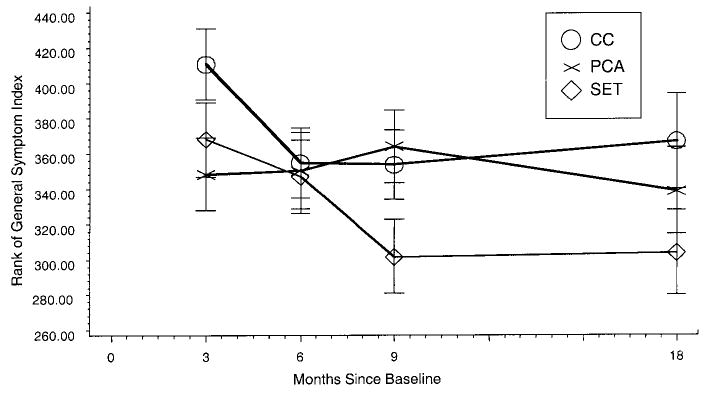
Predicted time path of ranked Brief Symptom Inventory scores, controlling for baseline. CC = community comparison condition; PCA = person-centered approach; SET = Structural Ecosystems Therapy.
Stage 2: Polynomial trends and dose–response relationships
For the psychological distress score, over time and across conditions, the BIC suggested that a quadratic model (BIC = 8,716.1) provided the best fit to the data. An examination of the polynomial components (linear and quadratic) with a Condition × Time interaction revealed a significant interaction with the linear growth component, F(2, 98) = 3.88, p < .024, but not with the quadratic growth component, F(2, 98) = 3.01, p < .054. Thus, whereas both linear and quadratic changes were evident in the data overall, there was a statistically significant difference between conditions in the linear component but not in the quadratic component.
We examined the possibility of a dose–response relationship in the effect of SET on psychological distress by adding the interaction of number of clinical contact hours and intervention condition to the linear growth component. There was a significant effect of the dose–response interaction term on the linear component, F(2, 282) = 3.68, p < .03. The linear slope term for women in the SET condition was significantly negative, indicating that, in the SET condition, the degree of decrease in distress was associated with amount of therapeutic contact. In the PCA condition, the effect of the interaction term on the over-time slope for distress was not significant, indicating that there was not a dose-response association with psychological distress outcomes in PCA.
Stage 3: Latent growth mixture modeling
In the latent growth mixture modeling exploratory analysis, the best-fitting solution, based on baseline levels and trajectories of psychological distress, comprised three classes of quadratic trajectories (BIC = 1,304.2). These classes appeared to be quite distinct from each other, as can be seen from examining the relationship between assigned class membership and the average probability of membership in the other classes (see the last set of rows in Table 2). The probability matrix indicates that most participants assigned to each class have only small probabilities of membership in other classes. The three-class solution for the latent growth mixture model is presented visually in Figures 2 and 3. The estimated effects within each class of each intervention on the intercepts and slopes of the psychological distress score are presented in Table 2.
Table 2.
Latent Growth Mixture Model for Psychological Distress
| Class 1 (n = 14)
|
Class 2 (n = 13)
|
Class 3 (n = 182)
|
||||
|---|---|---|---|---|---|---|
| Growth component | Estimate | |Est./SE| | Estimate | |Est./SE| | Estimate | |Est./SE| |
| Baseline intercept | 2.27 | 5.74 | 1.08 | 6.29 | 0.79 | 16.07 |
| Baseline PCA | 0.41 | 0.46 | 0.20 | 0.74 | 0.01 | 0.12 |
| Baseline SET | 0.37 | 0.88 | 0.45 | 1.93 | 0.16 | 1.63 |
| Linear intercept | −0.24 | 1.30 | 0.62 | 3.28 | −0.11 | 3.69 |
| Linear PCA | −0.68 | 2.48 | −0.21 | 0.97 | 0.03 | 0.55 |
| Linear SET | −0.10 | 0.43 | −0.18 | 0.83 | −0.11 | 2.23 |
| Quadratic intercept | −0.01 | 0.43 | −0.06 | 2.51 | 0.02 | 3.26 |
| Quadratic PCA | 0.11 | 4.32 | −0.01 | 0.34 | −0.01 | 0.66 |
| Quadratic SET | 0.04 | 1.13 | 0.01 | 0.32 | 0.01 | 1.29 |
| Average class probability | ||||||
| Class 1 | .96 | .04 | .01 | |||
| Class 2 | .00 | .95 | .01 | |||
| Class 3 | .04 | .01 | .98 | |||
Note. |Est./SE| is the absolute value of the estimate divided by its standard error. The reference group in each of the levels of the growth curve is the community comparison (CC) condition. Thus, the intercept refers to the predicted mean at baseline of the CC. The coefficients for person-centered approach (PCA) and structural ecosystems therapy (SET) represent their respective deviation from the CC intercept.
Figure 2.
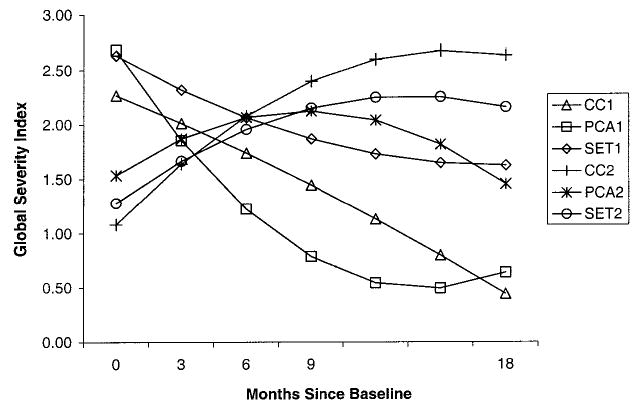
Latent growth mixture model for psychological distress, Classes 1 and 2. CC = community comparison condition; PCA = person-centered approach; SET = Structural Ecosystems Therapy; 1 = Class 1; 2 = Class 2.
Figure 3.
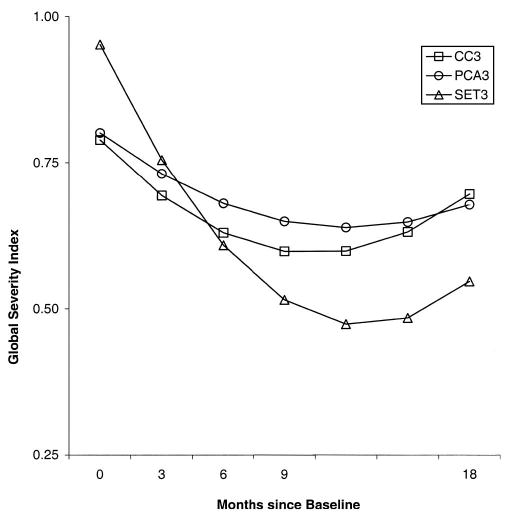
Latent growth mixture model for psychological distress, Class 3. CC = community comparison condition; PCA = person-centered approach; SET = Structural Ecosystems Therapy; 3 = Class 3.
The first class (see Figure 2) represents a relatively small group (n = 14, or 6.7% of the sample) of participants who had extremely high scores on psychological distress at baseline. Across conditions, the intercepts (predicted baseline scores) for psychological distress for each of the three conditions in this class were all at least 3.9 SDs above the clinical threshold using female nonpatient norms (Derogatis, 1993). Moreover, all participants in this class evidenced significant declines in distress across the duration of the study. The PCA condition was associated with a significantly more negative linear component and a significantly more positive linear-quadratic component than was the control condition, linear: t(170) = 2.48, p < .02; quadratic: t(170) = 4.32, p < .0001. The net effect is that the predicted means at the 18-month assessment were not significantly different between PCA and CC. SET was associated with the highest 3-month level of psychological distress and with the least amount of decline over time. SET was not significantly different from CC or from PCA on the linear and quadratic trends. For Class 1, SET was associated with the highest mean distress score at 18 months.
The second class (see Figure 2) also represented a relatively small group (n = 13, or 6.2% of the sample), who entered the study with clinically elevated psychological distress scores (although lower than those evidenced by Class 1). Estimated intercepts (at baseline) for psychological distress within this class, computed separately by condition, ranged from 1.08 to 1.54 (still exceeding the clinical threshold). In Class 2, in contrast to Class 1, the trajectories were all characterized by upward slopes, indicating increases in distress over time. In this class, none of the pairwise comparisons (i.e., SET vs. PCA; SET vs. CC; and PCA vs. CC) revealed significant differences over time.
The third class (see Figure 3) was the largest (n = 182, or 87% of the sample). The estimated intercepts (baseline) for psychological distress, computed separately by condition, ranged from .79 to .95. In contrast to Classes 1 and 2, this class was very near the clinical cutoff of psychological distress (although well above the nonpatient mean at 3 months, indicating elevated levels of psychological distress relative to community norms). In this class, SET evidenced a significantly greater (linear) rate of decline in psychological distress than did CC, t(170) = 2.23, p < .03, and a significantly greater (linear) rate of decline than did PCA, t(170) = 2.37, p < .02. SET participants evidenced a 0.75 SD decline in psychological distress score relative to the 0.18 SD decline observed in the CC group and the 0.22 SD decline observed in PCA. PCA was not significantly different from CC on the linear and quadratic trends.
Hypothesis 2: Family Hassles
Stage 1: Primary hypothesis test
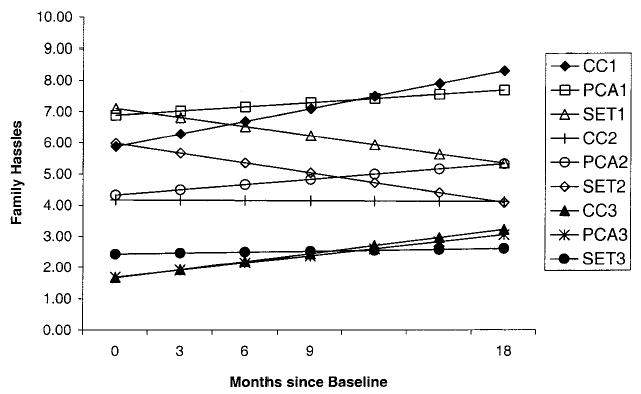
The primary mixed-model analysis of family hassles produced a significant Condition × Time interaction, F(6, 472) = 2.53, p < .03, indicating that the trajectory of family hassles over time differed significantly by condition, controlling for baseline level of family hassles.3 The main effects for condition, F(2, 472) = 1.84, p < .16, and time, F(3, 472) = 1.92, p < .13, were not significant. Figure 4 displays the predicted mean family hassles scores by condition and time (adjusted for baseline scores). The SET condition was associated with the highest mean level of family hassles at 3 months, after which the mean family hassles score in SET declined significantly between 3 and 9 months before increasing slightly at 18 months. As can be observed by examining the nonoverlapping error bars in Figure 4, SET was associated with significantly lower levels of family hassles than either CC or PCA at both 9 and 18 months. In contrast, both CC and PCA evidenced increases in family hassles over time. PCA was associated with a significantly greater increase in family hassles than either SET or CC through 9 months, and levels of family hassles were significantly higher in PCA than in SET or CC at 9 and 18 months.
Figure 4.
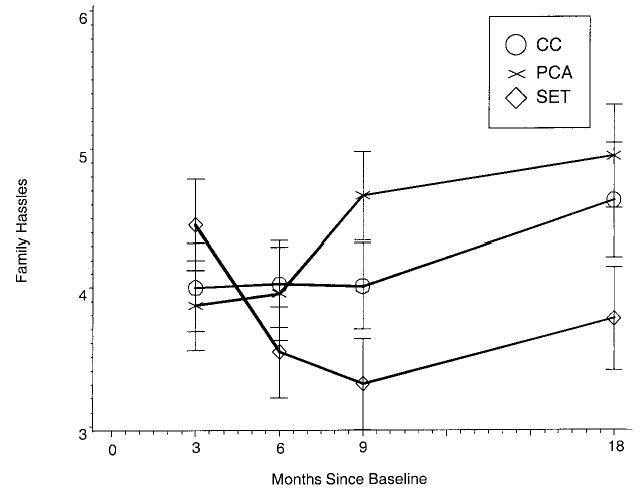
Predicted time path of family hassles, controlling for baseline. CC = community comparison condition; PCA = person-centered approach; SET = Structural Ecosystems Therapy.
Stage 2: Polynomial trends and dose–response relationships
For family hassles, the BIC suggested that a quadratic model provided the best fit to the data. An examination of the interaction of condition with each of the polynomial components revealed a significant interaction with the linear growth component, F(2, 97) = 5.17, p < .008, and a nonsignificant interaction with the quadratic growth component, F(2, 98) = 2.95, p < .058.
There was no evidence of a dose–response relationship in the effects of SET or PCA on family hassles. When number of clinical contact hours was added to the linear and quadratic portion of the trajectory, there was no significant effect.
Stage 3: Latent growth mixture modeling
The exploratory examination of classes based on baseline levels of and over-time trajectories in family hassles revealed a three-class linear solution (BIC = 4,278.7). As with psychological distress, the classes were relatively distinct from each other, with the weight of the probability of class membership falling on the diagonal (see last set of rows in Table 3). These three classes are presented visually in Figure 5, and the estimated effects of each intervention condition on these intercepts and slopes of family hassles by class are presented in Table 3.
Table 3.
Latent Growth Mixture Model for Family Hassles
| Class 1 (n = 30)
|
Class 2 (n = 91)
|
Class 3 (n = 88)
|
||||
|---|---|---|---|---|---|---|
| Growth component | Estimate | |Est./SE| | Estimate | |Est./SE| | Estimate | |Est./SE| |
| Intercept baseline | 5.88 | 7.41 | 4.17 | 14.40 | 1.66 | 3.28 |
| Baseline PCA | 1.01 | 1.28 | 0.16 | 0.41 | 0.02 | 0.04 |
| Baseline SET | 1.23 | 1.34 | 1.82 | 3.86 | 0.77 | 1.34 |
| Linear intercept | 0.40 | 2.39 | −0.01 | 0.07 | 0.26 | 1.25 |
| Linear PCA | −0.27 | 1.38 | 0.17 | 0.90 | −0.03 | 0.13 |
| Linear SET | −0.70 | 3.07 | −0.31 | 1.75 | −0.23 | 1.03 |
| Average class probability | ||||||
| Class 1 | .86 | .06 | .00 | |||
| Class 2 | .14 | .88 | .06 | |||
| Class 3 | .00 | .06 | .94 | |||
Note. |Est./SE| is the absolute value of the estimate divided by its standard error. The reference group in each of the levels of the growth curve is the community comparison (CC) condition. Thus, the intercept refers to the predicted mean at baseline of the CC. The coefficients for person-centered approach (PCA) and structural ecosystems therapy (SET) represent their respective deviation from the CC intercept.
Figure 5.
Latent growth mixture modeling for family hassles, all three classes. CC = community comparison condition; PCA = person-centered approach; SET = Structural Ecosystems Therapy; 1 = Class 1; 2 = Class 2; 3 = Class 3.
The first class for family hassles was the smallest (n = 30, 14.4% of the sample). This class was associated with the highest baseline levels of family hassles (with no significant differences by condition at baseline). In this class, women in the SET condition evidenced a significantly greater linear decline in family hassles than did women in CC, t(181) = 3.07, p < .003, or women in PCA, t(181) = 2.12, p < .05. In this class, PCA and CC were not significantly different from one another.
The second class for family hassles was the largest (n = 91, 43.5% of the sample). Participants in this class entered the study with slightly lower baseline levels of family hassles than did those in Class 1. Women in the SET condition showed a steeper (linear) decline in family hassles than did women in PCA, t(181) = −2.75; p < .05. There was only a weak effect, t(181) = 1.75, p < .10, for women in the SET condition to display a steeper decline in family hassles than those in CC. As in Class 1, women in PCA did not show significant differences in trajectories compared with women in CC.
Approximately 42% of the sample (n = 88) was placed into the third family hassles class. As a whole, this class reported considerably fewer mean family hassles at baseline than did the other classes. Class 3 also was not associated with any significant change in the amount of family hassles over time, for any of the conditions.
Hypothesis 3: Family Support
Stage 1: Primary hypothesis test
The primary mixed-model analysis for family support produced a significant main effect of time, F(4, 679) = 23.68, p < .0001, indicating significant changes across all three conditions. However, the Time × Condition interaction was not statistically significant, F(8, 679) = 1.02, p < .43, nor was there a main effect for condition, F(2, 679) = 0.91, p < .41.4 The trajectories indicate that all three conditions were associated with declines in family support and with leveling off between 9 and 18 months. Because there was no intervention effect on the trajectories over time, the Stage 2 analyses examining polynomial trends and dose–response relationship were not conducted.
Stage 3: Latent growth mixture modeling
The exploratory latent growth mixture modeling analysis on family support again produced a three-class solution, this time based on quadratic growth components (BIC = 6,303.4). As with psychological distress and family hassles, the classes were quite distinct from each other, with the weight of the probability of class membership falling on the diagonal. In the case of family support, however, there were no significant effects of intervention condition within any of the three classes.5
Mediating Effects of Family Hassles in the Impact of Intervention Condition on Psychological Distress
Because SET did not significantly affect family support, mediational analyses of family support on psychological distress could not be conducted. We used a latent growth curve framework to examine the potential role of family hassles in mediating the effect of intervention condition on psychological distress. First, paths from the growth curve of family hassles to the growth curve of psychological distress were significant, χ2(3) = 10.9, p < .02. Second, once these paths were included in the model, the effect of SET on the growth curve of psychological distress was no longer significant, χ2(3) = 1.7, p < .64. Prior to the addition of the path from the growth curve of hassles to the growth curve of psychological distress, SET had a significant linear effect on the growth curve of distress, t(175) = 2.03, p < .05, whereas after the paths were added, the linear effect of SET on the psychological distress slope was not significant, t(169) = .84, p < .40. According to Baron and Kenny’s (1986) definition of mediation, it can thus be assumed that the effects of SET on family hassles mediated the effects of SET on psychological distress. However, because the change patterns observed for family hassles and psychological distress were observed during the same time interval (i.e., between 3 and 18 months), no causal inferences can be drawn (cf. Kraemer, Stice, Kazdin, Offord, & Kupfer, 2001). To attempt to rule out reciprocal causation, we estimated a mediation model in which the effect of SET on family hassles would be mediated by psychological distress. Drawing the paths from psychological distress to family hassles showed a significant effect, χ2(3) = 9.6, p < .03. In this model, however, the effect of SET on the linear change in family hassles (initially significant: t[175] = 2.66, p < .01) maintained a weak effect on the linear change component, t(169) = 1.94, p < .055, when a pathway from the growth curve for psychological distress to the growth of family hassles was included. Therefore, psychological distress did not fully mediate the effect of SET on family hassles. Whereas reverse causation could not be ruled out entirely, there was greater support for the mediation of family hassles on the effects of SET on psychological distress than for the mediation of psychological distress on the effects of SET on family hassles.
Discussion
The present study was conducted to investigate the efficacy of SET, a family-ecological intervention, in reducing distress, reducing family hassles, and increasing family support in HIV-seropositive African American women. The efficacy of SET was evaluated by comparing its outcomes against those of the attention/comparison control (PCA) condition and the CC condition.
Primary Outcomes
Psychological distress
Our findings indicate that HIV-seropositive African American women assigned to the SET condition decreased significantly more in psychological distress during and after treatment than did those women in the PCA or CC conditions. Specifically, SET was significantly more efficacious than either PCA or CC during therapy (i.e., between baseline and 9 months), and SET was the only condition that maintained its gains at the 18-month assessment. In contrast, although there was some variability in distress in PCA and CC, there were no significant changes over time in these conditions.
Exploratory analyses examining the women by latent class indicated that SET was more efficacious than either PCA or CC in reducing distress for the class at the clinical threshold of psychological distress, Class 3. In our sample, this represented the majority of the women. During the course of the study, the women in Class 3 assigned to the SET condition evidenced a clinically meaningful mean decline of more than two times the female nonpatient adult normative standard deviation for the Brief Symptom Inventory Global Severity Index. In contrast, all women in the most severely distressed class, Class 1, who were initially over four normative standard deviations above the clinical threshold, reported significant declines across conditions, with the PCA condition associated with significantly greater decline. For Class 2, representing intermediate levels of psychological distress (i.e., above the clinical threshold but not as severely distressed as Class 1), all treatment conditions were associated with increased levels of psychological distress across time but no significant differences by condition. Thus, SET was efficacious for women at the threshold of clinical levels of distress at baseline, but it was not efficacious for the small group of women who were extremely distressed at baseline. Thus, along with receiving SET, these highly distressed women may be in need of an additional intervention component to reduce their distress levels. Psychological distress, as operationalized in this study, consists of a number of symptomatic dimensions, including features of depression and anxiety. Efficacious treatments to be used along with SET for highly distressed women might consist of both behavioral and pharmacological components that specifically target depression and anxiety. In a subsequent study currently underway (Grant DA15004; Daniel Feaster, Principal Investigator), in the SET condition, we screen for distress levels and actively work with highly distressed women to obtain psychiatric consultation for them and, when appropriate, pharmacological treatment.
Family hassles
SET was more efficacious than either the PCA or CC conditions in reducing the number of family hassles. Specifically, among the three treatment conditions, only SET was associated with consistent declines in family hassles at the 3-, 6-, and 9-month assessments and maintenance of this difference at 18 months. PCA, on the other hand, demonstrated an increase over time in family hassles. This finding may be of particular interest because it is similar to our findings on a prior study, albeit with a different individual condition, a different population, and a different measure of family functioning. As in the current study, in that study (Szapocznik et al., 1989) with 6–11-year-old Cuban boys with behavior and emotional problems, the family condition, also based on BSFT, was found to improve family functioning, whereas the individual condition, individual child psychodynamic therapy, was found to bring about a deterioration in family functioning after the completion of treatment. At that time, we speculated that one possible explanation for deteriorating family functioning in the individual condition may have been that when the individual who is the target of therapy improves, he or she is extricated from family maladaptive patterns of interaction, causing an unbalancing of the family’s homeostasis. Although unbalancing can be a means to improving family interactions, and is used as a strategy in family therapy, families typically require the guidance of a therapist to replace the unraveling maladaptive interactions with more adaptive patterns. In the current study, although that may be one explanation, other explanations are possible. One is that PCA gave women a stronger sense of self, which permitted them to acknowledge the annoying behavior of their family members and, thus, to report more family hassles. Another explanation is that women in PCA may have developed a more “self” or individualistic orientation, which clashed with their African American family’s more collectivist orientation (Boyd-Franklin, 1989).
The exploratory latent growth mixture modeling suggested that SET was most efficacious with women with high levels of family hassles at baseline, somewhat efficacious with women entering the study with moderate levels of family hassles, and not efficacious with those women entering the study with low levels of family hassles. This supports the ability of SET to reduce the woman’s experience of hassles within the family. On the other hand, in families with low levels of hassles at baseline, there may not have been many within-family hassles to correct in therapy. This may represent a true lack of family hassles or a floor effect of the measure.
Family social support
The finding that SET failed to increase family support was unexpected given that fostering family support is a primary target of SET and is considered an active ingredient of the intervention. A possible explanation for this finding lies in the fact that family support at baseline was a strong predictor of engagement of adult family members in the SET condition (Mitrani, Prado, Feaster, Robinson-Batista, & Szapocznik, 2003). As a result, those women for whom an increase in family support was most needed were those whose adult family members were least likely to participate in the treatment. Conversely, those families in which adult family members participated in SET were those who already were supportive of the target woman. Because SET was not efficacious in increasing family support for those participants who most needed it, changes in the intervention are needed that will bring about the engagement of family members when family support is low.
SET is based on BSFT (Szapocznik et al., 2003; Szapocznik & Williams, 2000), an intervention that is very hierarchical, with the therapist taking a strong leadership role. BSFT, however, was developed for families of troubled children and adolescents. In making the transition to SET for application with adults, we discussed whether we ought to give an adult target client a more central role in determining whom she involves in therapy. Because we discussed extensively during model development how assertive we should be to involve families if the women were reluctant to involve them, we were aware that we decided to allow the woman to dictate the involvement of her family. Although we did not expect this decision to cause a failure in improving family support, we were watching for the efficacy or lack of efficacy of allowing women to determine inclusion of their families in therapy. As we note above, this decision resulted in women who had strong family support engaging their family members, whereas women with poor family support often did not have family members involved in SET. The strategy of using the woman as the central gatekeeper to family involvement in treatment yielded few opportunities to work with the families of the women who most needed help to increase their family support. Building on this experience, in a subsequent trial (Grant DA15004; Daniel Feaster, Principal Investigator), we have changed the model to require the therapist to be much more assertive in engaging family members in families in which the woman reports low levels of family support.
Sometimes the woman’s concerns about engaging her family may be highly justifiable, such as concerns about family members who are drug involved or abusive. However, in other cases, a woman’s wish to not involve her family may be based on past noxious support that at one time existed but caused the woman to move away from her family. Some of these may be highly treatable with SET, such as cases in which there is high family conflict, high negativity toward the woman, or the woman is stigmatized and blamed by the family. Typically, these problems reflect familial overinvolvement (i.e., enmeshment) that paradoxically has led to disengagement. Second, family members may indeed be disinterested in the woman. This also is a treatable problem, although more difficult for SET to treat than conflict, negativity, stigmatizing, and blaming.
Dose–Response Effects
Because participants were not randomized to receive different treatment dosages, we were not able to test for a true dose–response effect. Therefore, we are only able to report endogenous dose–response effects; that is, those that reflect a naturally occurring process of decision making on the part of the client and therapist (i.e., how often to participate in treatment, or when to end treatment). This relationship may be informative about the natural properties of SET (Feaster, Newman, & Rice, 2003). Of the two outcomes for which SET had a significant effect, there was a significant dose–effect relationship only for psychological distress. Amount of therapeutic contact in the SET condition was predictive of the degree of decline in distress over time. It appears that those women who evidenced more need for the intervention (or greater motivation to participate), possibly in the form of heightened discomfort with their own levels of distress, received higher doses of treatment.
The lack of a dose–response relationship for family hassles may be a function of the majority of participants reporting low baseline levels of family hassles. The small subsample (n = 30) of women with elevated family hassles at baseline did not provide adequate power to uncover a dose–response effect. Future studies might consider including only participants with moderate to high level of hassles. It is possible that in a sample with higher levels of hassles, there would have been sufficient variance to demonstrate a dose–response relationship.
Mediation Effects
In the present study, SET had a significant impact on both psychological distress and family hassles. Within a growth curve framework, our results suggest that the effect of SET on psychological distress may have been mediated by the decline in family hassles. However, given that the effects of SET on distress and on family hassles occurred simultaneously (i.e., between the same set of time points), it may not be safe to assume that the effects of SET on psychological distress operated through changes in family hassles. Whereas Baron and Kenny’s (1986) classic definition of mediation does not require that the mediator temporally precede the outcome, such temporal ordering is important to the establishment of causality (Kraemer et al., 2001). In accordance with assumptions that full mediation implies a causal relationship, some have argued that assumptions of full mediation require a complete absence of temporal overlap between the mediating and outcome processes (Kraemer et al., 2001). Thus, it can be safely asserted that the effects of SET on psychological distress and on family hassles were related and that the effects of SET on family hassles may have mediated (i.e., without temporal independence between the mediator and the outcome) the effects of SET on psychological distress. There is always a possibility of reverse causality; for example, that as women became less distressed they tended to view their families as less troublesome or that as women became less distressed their family members’ behavior toward the women (i.e., family hassles) changed. Indeed, there is some evidence for this: A reverse-causality test of the pathways from the growth curve in psychological distress to the growth curve of family hassles was significant. It is not possible to test this reciprocal causality jointly, so it is difficult to say which direction yields the stronger effect. It is true, however, that in the model of change in family hassles predicting change in psychological distress, the effect of SET was reduced to nonsignificance, whereas in the reverse-causality specification, the effect of SET on family hassles maintained a weak effect (p < .055) when distress was added to the model. This suggests that the effect of the intervention on psychological distress is more completely explained by the change in family hassles than is the effect of the intervention on family hassles explained by the change in psychological distress.
Limitations
We acknowledge a number of limitations to this study. First, engagement rates among the target women were lower than expected (75% in SET and 61% in PCA; Prado et al., 2002). In our intent-to-treat design, nonparticipation in the intervention undoubtedly contributed to the findings. Moreover, although SET was designed as a family–ecological treatment, in 9.8% of cases in which the woman had at least one therapy session no members of the family or ecosystem were involved. Second, participants in the SET condition received significantly more hours of treatment than did participants in the PCA condition. This may be evidence that SET, possibly due in part to its specialized engagement and retention strategies, was more efficacious in facilitating motivation and availability for therapy than was PCA. However, the inability of PCA to retain participants may have weakened its ability to serve as an appropriate attention control–comparison condition. A third limitation of the current study is its reliance on the target woman’s self-report for family hassles and family support. Thus, we have assessed only one person’s viewpoint regarding family level interactional processes. The use of self-reports may have introduced bias that could have been overcome using observational measures of family interactions. A fourth limitation was the lack of balance across conditions on the dependent measures. Including the baseline values of the dependent measures in the urn randomization would have prevented our need to covary for distress and family hassles in the Stage 1 analyses. A fifth limitation was the lack of measures that might have assessed outcomes specific to PCA.
Conclusions
Despite these limitations, this study provides important evidence for the efficacy of SET in reducing distress and family-related hassles in HIV-seropositive African American women. In turn, because distress is associated with HIV progression (S. Cruess et al., 2000), SET may have helped these women to maintain their health and to slow the worsening of HIV symptoms. It appears that, for the majority of women in the study, SET was significantly more efficacious in reducing psychological distress than either the PCA attention control comparison or CC. Further, for women entering the study with the highest levels of self-reported family hassles, SET was significantly more efficacious in reducing family hassles than either the PCA attention control comparison or CC. Our results, although tentative, suggest that the mechanisms through which SET reduced distress may have involved reducing family-related hassles.
The results of this study also point to family engagement as an important area in which the SET intervention may need to be further developed and refined. Additional strategies may need to be developed to engage disengaged families and to work with the women’s internal barriers to involve in therapy her adult family members who provide her with low levels of support. Such specialized engagement strategies have been shown to be efficacious in BSFT with adolescents (Coatsworth, Santisteban, McBride, & Szapocznik, 2001; Santisteban et al., 1996; Szapocznik et al., 1988).
Implications
This research may have implications for HIV progression, given that stressors (e.g., family hassles) and distress have been linked to impaired immune function. This research should be generalizable to the population of HIV-seropositive African American women in treatment today who, like the sample in this study, are likely to be more concerned about living with HIV than dying of AIDS. Further research should explore the potential of SET in improving immune outcomes in HIV-seropositive African American women. Research on family interventions with HIV-seropositive African American women and their families may also have implications for African American families in which a member is experiencing other types of chronic medical conditions. Distress is common in patients with chronic medical illnesses (e.g., for chronic pain of rheumatoid arthritis, Brown, Glass, & Park, 2002; for coronary heart disease, Burg & Abrams, 2001). Moreover, distress may have implications for recovery (e.g., for recovery after coronary bypass, Mahler & Kulik, 2002). Further research should explore the impact of a family–ecological intervention such as SET in African American women with other chronic medical conditions. Future research might explore whether reducing family hassles and distress in African American women leads to better medical recovery.
Acknowledgments
This work was supported by National Institute of Mental Health (NIMH) Grant R37 MH55796 (José Szapocznik, Principal Investigator). We thank Bengt Muthén, Hendricks Brown, and the members of the Prevention Science Methodology Group (National Institute on Drug Abuse and NIMH Grant 5R01-MH40859) for helpful comments; person-centered approach and Structural Ecosystems Therapy therapists Ernestine Davis, Susan Edwards, April Jackson-Gilfort, Doris Green, and Rhonda Nelson; and the assessment and recruitment staff. Finally, we thank the families who participated in this study.
Footnotes
Family problems listed on the checklist included fear of disclosing HIV status to family members, conflicts with family, communication problems with family, drug and/or alcohol problems in the family, child custody problems, child-related problems (e.g., school, behavior, health), and problems with one’s romantic partner. Nonfamily problems listed on the checklist included anxiety, depression, loneliness, transportation problems, and fear that others (outside the family) will discover one’s HIV status.
Because of higher attrition at Time 5, we re-examined the data using the first four time points only (i.e., not using Time 5 data). The analysis yielded similar results.
Because of higher attrition at Time 5, we re-examined the data using the first four time points only (i.e., not using Time 5 data). The analysis yielded similar results.
Because of higher attrition at Time 5, we re-examined the data using the first four time points only (i.e., not using Time 5 data). The analysis yielded similar results.
Table not shown, but available from José Szapocznik upon request.
References
- Aléman, J., Kloser, P., Kreibick, T., Steiner, G. L., & Boyd-Franklin, N. (1995). Women and HIV/AIDS. In N. Boyd-Franklin, G. L. Steiner, & M. G. Boland (Eds.), Children, families, and HIV/AIDS: Psychosocial and therapeutic issues (pp. 90–111). New York: Guilford Press.
- American Psychiatric Association. (1987). Diagnostic and statistical manual of mental disorders (3rd ed., rev.). Washington, DC: Author.
- Antoni MH, Cruess DG, Cruess S, Lutgendorf S, Kumar M, Ironson G, et al. Cognitive–behavioral stress management intervention effects on anxiety, 24-hr urinary norepinephrine output, and t-cytotoxic/suppressor cells over time among symptomatic HIV-infected gay men. Journal of Consulting and Clinical Psychology. 2000;68:31–45. doi: 10.1037//0022-006x.68.1.31. [DOI] [PubMed] [Google Scholar]
- Baron RM, Kenny DA. The moderator–mediator variable distinction in social psychological research: Conceptual, strategic, and statistical considerations. Journal of Personality and Social Psychology. 1986;51:1173–1182. doi: 10.1037//0022-3514.51.6.1173. [DOI] [PubMed] [Google Scholar]
- Belsky J, Crnic K, Gable S. The determinants of coparenting in families with toddler boys: Spousal differences and daily hassles. Child Development. 1995;66:629–642. [PubMed] [Google Scholar]
- Boyd-Franklin, N. (1989). Black families in therapy. New York: Guilford Press.
- Boyd-Franklin, N., & Boland, M. G. (1995). A multisystemic approach to service delivery for HIV/AIDS families. In N. Boyd-Franklin, G. L. Steiner, & M. G. Boland (Eds.), Children, families, and HIV/AIDS: Psychosocial and therapeutic issues (pp. 216–232). New York: Guilford Press.
- Bozarth JD, Brodley BT. Actualization: A functional concept in client-centered therapy. Journal of Social Behavior and Personality. 1991;6:45–59. [Google Scholar]
- Brown SC, Glass JC, Park DC. The relationship of pain and depression to cognitive function in rheumatoid arthritis patients. Pain. 2002;96:279–284. doi: 10.1016/S0304-3959(01)00457-2. [DOI] [PubMed] [Google Scholar]
- Bryk, A. S., & Raudenbush, S. W. (1992). Hierarchical linear models: Applications and data analysis methods. Newbury Park, CA: Sage.
- Burg MM, Abrams D. Depression in chronic medical illness: The case of coronary heart disease. Journal of Clinical Psychology. 2001;57:1323–1337. doi: 10.1002/jclp.1100. [DOI] [PubMed] [Google Scholar]
- Centers for Disease Control and Prevention. (2002a). Division of HIV/AIDS prevention: Basic statistics. Retrieved October 1, 2002, from http://www.cdc.gov/hiv/stats.htm#cumaids
- Centers for Disease Control and Prevention. (2002b). Estimated male adult/adolescent AIDS incidence, by exposure category and race/ethnicity, diagnosed in 2000, and cumulative totals through 2000. Retrieved October 1, 2002, from http://www.cdc.gov/hiv/stats/hasr1301/table19.htm
- Centers for Disease Control and Prevention. (2002c). Estimated female adult/adolescent AIDS incidence, by exposure category and race/ethnicity, diagnosed in 2000, and cumulative totals through 2000. Retrieved October 1, 2002, from http://www.cdc.gov/hiv/stats/hasr1301/table20.htm
- Centers for Disease Control and Prevention. (2002d). HIV/AIDS among U.S. women: Minority and young women at continuing risk. Retrieved October 1, 2002, from http://www.cdc.gov/hiv/pubs/facts/women.pdf
- Coatsworth JD, Santisteban DA, McBride CK, Szapocznik J. Brief strategic family therapy versus community: Engagement, retention and an exploration of the moderating role of adolescent symptom severity. Family Process. 2001;40:313–332. doi: 10.1111/j.1545-5300.2001.4030100313.x. [DOI] [PubMed] [Google Scholar]
- Compas BE, Williams RA. Stress, coping, and adjustment in mothers and young adolescents in single and two parent families. American Journal of Community Psychology. 1990;18:525–545. doi: 10.1007/BF00938058. [DOI] [PubMed] [Google Scholar]
- Conover WJ, Iman RL. Rank transformations as a bridge between parametric and nonparametric statistics. American Statistician. 1981;35:124–133. [Google Scholar]
- Conover WJ, Iman RL. Analysis of covariance using the rank transformation. Biometrics. 1982;38:715–724. [PubMed] [Google Scholar]
- Cruess D, Antoni MH, Schneiderman N, Ironson G, McCabe P, Fernandez JB, et al. Cognitive–behavioral stress management increases free testosterone and decreases psychological distress in HIV-seropositive men. Journal of Health Psychology. 2000;19:12–20. doi: 10.1037//0278-6133.19.1.12. [DOI] [PubMed] [Google Scholar]
- Cruess S, Antoni M, Kilbourn K, Ironson G, Klimas N, Fletcher MA, et al. Optimism, distress, and immunologic status in HIV infected gay men following Hurricane Andrew. International Journal of Behavioral Medicine. 2000;7:160–182. [Google Scholar]
- De Jong GM, Van Sonderen E, Emmelkamp PMG. A comprehensive model of stress and neuroticism in explaining the stress–distress relationship. Psychotherapy and Psychosomatics. 1999;68:290–298. doi: 10.1159/000012346. [DOI] [PubMed] [Google Scholar]
- DeLongis A, Folkman S, Lazarus RS. The impact of daily stress on health and mood: Psychosocial and social resources as mediators. Journal of Personality and Social Psychology. 1988;54:486–495. doi: 10.1037//0022-3514.54.3.486. [DOI] [PubMed] [Google Scholar]
- Derogatis, L. R. (1993). Brief Symptom Inventory: Administration, scoring, and procedures manual. Minneapolis, MN: National Computer Systems.
- Feaster, D. J., Goodkin, K., Blaney, N. T., Baldewicz, T., Tuttle, R. S., Woodward, C., et al. (2000). Longitudinal psychoneuroimmunological relationships in the natural history of HIV-1 infection: The stressor-support-coping model. In K. Goodkin & A. Visser (Eds.), Psychoneuroimmunology: Stress, mental disorders, and health (pp. 179–229). Washington, DC: American Psychiatric Press.
- Feaster DJ, Newman FL, Rice C. Longitudinal analysis when the experimenter does not determine when treatment ends: What is dose–response? Clinical Psychology and Psychotherapy. 2003;10:352–360. doi: 10.1003/cpp.382. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Feaster DJ, Szapocznik J. Interdependence of stress processes among African American family members: Influence of HIV serostatus and a new infant. Psychology and Health. 2002;17:339–363. doi: 10.1080/08870440290029584. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gillman RR, Newman BS. Psychosocial concerns and strengths of women with HIV infection: An empirical study. Families in Society. 1996;77:131–141. [Google Scholar]
- Goodkin K, Blaney NT, Tuttle RS, Nelson RH. Bereavement and HIV infection. International Review of Psychiatry. 1996;8:201–216. [Google Scholar]
- Hill EN, Herman-Stahl MA. Neighborhood safety and social involvement: Associations with parenting behaviors and depressive symptoms among African American and Euro-American mothers. Journal of Family Psychology. 2002;16:209–219. doi: 10.1037//0893-3200.16.2.209. [DOI] [PubMed] [Google Scholar]
- Institute of Medicine. (1990). Treating drug problems: A study of the evolution, effectiveness, and financing of public and private drug treatment systems (Report by the Institute of Medicine Committee for the Substance Abuse Coverage Study, Division of Health Care Services). Washington, DC: National Academy Press.
- Jackson-Gilfort A, Mitrani VB, Szapocznik J. Conjoint couple’s therapy in low income, African American couples: A case report. Journal of Family Psychotherapy. 2000;11:37–60. [Google Scholar]
- Kazdin, A. E. (1994a). Methodology, design, and evaluation in psychotherapy research. In A. E. Bergin & S. L. Garfield (Eds.), Handbook of psychotherapy and behavior change (pp. 19–71). New York: Wiley.
- Kazdin, A. E. (1994b). Psychotherapy for children and adolescents. In A. E. Bergin & S. L. Garfield (Eds.), Handbook of psychotherapy and behavior change (pp. 543–594). New York: Wiley.
- Kraemer HC, Stice E, Kazdin A, Offord D, Kupfer D. How do risk factors work together? Mediators, moderators, and independent, overlapping and proxy risk factors. American Journal of Psychiatry. 2001;158:848–856. doi: 10.1176/appi.ajp.158.6.848. [DOI] [PubMed] [Google Scholar]
- Leslie MB, Stein JA, Rotheram-Borus M. The impact of coping strategies, personal relationships, and emotional distress on health-related outcomes of parents living with HIV or AIDS. Journal of Social and Personal Relationships. 2002;19:45–66. [Google Scholar]
- Littell, R. C., Milliken, G. A., Stroup, W. W., & Wolfinger, R. D. (1996). SAS systems for mixed models. Cary, NC: SAS.
- Mahler HIM, Kulik JA. Effects of a videotape information intervention for spouses on spouse distress an patient recovery from surgery. Health Psychology. 2002;21:427–437. [PubMed] [Google Scholar]
- Markowitz JC, Spielman LA, Sullivan M, Fishman B. An exploratory study of ethnicity and psychotherapy outcome among HIV-positive patients with depressive symptoms. Journal of Psychotherapy Practice and Research. 2000;9:226–231. [PMC free article] [PubMed] [Google Scholar]
- Minuchin, S., & Fishman, H. C. (1981). Family therapy techniques. Cambridge, MA: Harvard University Press.
- Mitrani VB, Prado G, Feaster DJ, Robinson-Batista C, Szapocznik J. Relational factors and family treatment engagement among low-income, HIV+ African American mothers. Family Process. 2003;42:31–46. doi: 10.1111/j.1545-5300.2003.00031.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mitrani, V. B., Szapocznik, J., & Robinson-Batista, C. (2000). Structural ecosystems therapy with seropositive African American mothers. In W. Pequegnat & J. Szapocznik (Eds.), The role of families in preventing and adapting to HIV/AIDS (pp. 243–279). Thousand Oaks, CA: Sage.
- Mulder CL, de Vroome EMM, van Griensven GJP, Antoni MH, Sandfort TGM. Avoidance as a predictor of the biological course of HIV infection over a 7-year period in gay men. Health Psychology. 1999;18:107–113. doi: 10.1037//0278-6133.18.2.107. [DOI] [PubMed] [Google Scholar]
- Murray VM, Brown PA, Brody GH, Cutrona CE, Simons RL. Racial discrimination as a moderator of the links among stress, maternal psychological functioning, and family relationships. Journal of Marriage and Family. 2001;63:915–926. [Google Scholar]
- Muthén B, Brown CH, Masyn K, Jo B, Khoo ST, Yang CC, et al. General growth mixture modeling for randomized preventive interventions. Biostatistics. 2002;3:459–475. doi: 10.1093/biostatistics/3.4.459. [DOI] [PubMed] [Google Scholar]
- Muthén, L. K. & Muthén, B. O. (1998–2003). Mplus user’s guide. Los Angeles, CA: Author.
- Nelson RH, Mitrani VB, Szapocznik J. Applying a family-ecosystemic model to reunite a family separated due to child abuse: A case study. Contemporary Family Therapy. 2000;22:125–146. [Google Scholar]
- Pereda M, Ayuso-Mateos JL, Gomez Del Barrio A, Echevarria S, Farinas MC, Garcia Palomo D, et al. Factors associated with neuropsychological performance in HIV-seropositive subjects without AIDS. Psychological Medicine. 2000;30:205–217. doi: 10.1017/s0033291799001348. [DOI] [PubMed] [Google Scholar]
- Prado G, Szapocznik J, Mitrani VB, Mauer M, Smith L, Feaster DJ. Factors influencing engagement into interventions for adaptation to HIV in African American women. AIDS and Behavior. 2002;6:141–151. doi: 10.1023/a:1015497115009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rogers C. The essence of psychotherapy: A client-centered view. Annals of Psychotherapy. 1959;1:51–57. [Google Scholar]
- Santisteban DA, Szapocznik J, Perez-Vidal A, Kurtines WM, Murray EJ, LaPerriere A. Efficacy of intervention for engaging youth and families into treatment and some variables that may contribute to differential effectiveness. Journal of Family Psychology. 1996;10:35–44. [Google Scholar]
- Sarason IG, Sarason BR, Shearin EN, Pierce GR. A brief measure of social support: Practical and theoretical implications. Journal of Social and Personal Relationships. 1987;4:497–510. [Google Scholar]
- Schwartz G. Estimating the dimension of a model. The Annals of Statistics. 1978;6:461–464. [Google Scholar]
- Seidman E, Chesir TD, Friedman JL, Yoshikawa H, Allen L, Roberts A. The risk and protective functions of perceived family and peer microsystems among urban adolescents in poverty. American Journal of Community Psychology. 1999;27:211–237. doi: 10.1023/A:1022835717964. [DOI] [PubMed] [Google Scholar]
- Shaw DS, Keenan K, Vondra JI, Delliquadri E, Giovannelli J. Antecedents of preschool children’s internalizing problems: A longitudinal study of low-income families. Journal of The American Academy of Child and Adolescent Psychiatry. 1997;36:1760–1767. [PubMed] [Google Scholar]
- Smith L, Feaster DJ, Prado G, Kamin M, Blaney N, Szapocznik J. The psychosocial functioning of HIV+ and HIV− African American mothers. AIDS and Behavior. 2001;5:219–231. [Google Scholar]
- Smith MY, Rapkin BD. Social support barriers to family involvement in care giving for persons with AIDS: Implications for patient education. Patient Education and Counseling. 1996;27:85–94. doi: 10.1016/0738-3991(95)00792-x. [DOI] [PubMed] [Google Scholar]
- Spitzer, R., Williams, J., Gibbon, M., & First, M. (1989). Structured Clinical Interview for DSM–III–R Disorders. New York: New York State Psychiatric Institute, Biometrics Research Department.
- Strupp HH, Hadley SW. Specific versus nonspecific factors in psychotherapy: A controlled study of outcome. Archives of General Psychiatry. 1979;36:1125–1136. doi: 10.1001/archpsyc.1979.01780100095009. [DOI] [PubMed] [Google Scholar]
- Szapocznik, J., Hervis, O. E., & Schwartz, S. J. (2003). Brief Strategic Family Therapy for adolescent drug abuse. Rockville, MD: National Institute on Drug Abuse.
- Szapocznik, J., & Kurtines, W. M. (1989). Breakthroughs in family therapy with drug abusing problem youth. New York: Springer.
- Szapocznik J, Perez-Vidal A, Brickman A, Foote FH, Santisteban D, Hervis OE, et al. Engaging adolescent drug abusers and their families into treatment: A strategic structural systems approach. Journal of Consulting and Clinical Psychology. 1988;56:552–557. doi: 10.1037//0022-006x.56.4.552. [DOI] [PubMed] [Google Scholar]
- Szapocznik J, Rio AT, Hervis OE, Mitrani VB, Kurtines WM, Faraci AM. Assessing change in family functioning as a result of treatment: The Structural Family Systems Rating Scale (SFSR) Journal of Marital and Family Therapy. 1991;17:295–310. [Google Scholar]
- Szapocznik J, Rio A, Murray E, Cohen R, Scopetta MA, Rivas-Vasquez A, et al. Structural family versus psychodynamic child therapy for problematic Hispanic boys. Journal of Consulting and Clinical Psychology. 1989;57:571–578. doi: 10.1037//0022-006x.57.5.571. [DOI] [PubMed] [Google Scholar]
- Szapocznik J, Williams RA. Brief strategic family therapy: Twenty-five years of interplay among theory, research and practice in adolescent behavior problems and drug abuse. Clinical Child and Family Psychology Review. 2000;3:117–134. doi: 10.1023/a:1009512719808. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wei LJ, Lachin JM. Properties of the urn randomization in clinical trials. Controlled Clinical Trials. 1988;9:345–364. doi: 10.1016/0197-2456(88)90048-7. [DOI] [PubMed] [Google Scholar]