

SUMMARY
This study examined the feasibility of a CD-ROM intervention to prevent alcohol abuse among high-risk youths. Youths from 41 community-based agencies in greater New York City participated in a randomized trial of a skills-based interactive CD-ROM. Outcome data were collected on 489 early adolescents in these agencies before and after a randomized subset of youths interacted with a 10-session alcohol abuse prevention program on CD-ROM. Compared to control participants, youths in the intervention arm had a positive increase in perceived harm of alcohol use and increased assertiveness skills. At posttest, drinking rates for control and intervention participants were equal and unchanged from pretest. These findings suggest that CD-ROM technology offers a new and promising medium for engaging high-risk youth in an alcohol abuse prevention program. Study implications and future applications of the present approach are discussed.
Keywords: Alcohol abuse, CD-ROM, prevention, youth, computer, skill- building
Nearly one half of all U.S. youths have tried alcohol before ninth grade, and by tenth grade 50% have been drunk at least once (Centers for Disease Control and Prevention, 2000; Johnston, O’Malley, & Bachman, 2002). Expectedly, youthful drinking often antecedes adult drinking. More than 40% of individuals who start drinking before age 13 years will abuse alcohol or develop alcohol dependence as adults (Grant & Dawson, 1997). In a survey of 18- to 24-year-old current drinkers who failed to complete high school, nearly 60% had drunk alcohol before age 16 years (National Institute on Alcohol Abuse and Alcoholism, 1998). Clearly, the time to prevent alcohol abuse is before young people enter the teen years.
Prevention programs aimed at alcohol and other substance use have proven their worth (Botvin & Kantor, 2000; Scheier, Botvin, & Griffin, 2001; Schinke, Gordon, & Weston, 1990). Before they are widely disseminated and accessible, however, prevention programs must address a number of challenges. Chief among these challenges is finding a way to attract and sustain youths’ attention. These engaging prevention programs must be replicable and easily disseminated, and they must lend themselves to high protocol fidelity to move from science to practice. In fact, well-implemented programs are associated with commensurately positive results (Botvin, Baker, Dusenbury, Botvin, & Diaz, 1995). Cost-containment is vital before prevention will be embraced by budget-minded education and non-profit sectors. Fortunately, many, if not all, of these obstacles to effective prevention programming may be addressed through new technologies.
Prevention and New Technologies
The marriage of prevention science and new technologies offers considerable promise. Prevention aims to deter problem behavior before it starts and, failing that, to delay the age of onset of behavior problems. With respect to youths and alcohol consumption, if drinking is delayed until age 21 years, the risk of serious alcohol problems decreases by 70% (Grant & Dawson, 1997). For prevention programs to work, they must establish and sustain connections with youth recipients. The appropriate use of new technologies is essential to making that connection.
Reviews of prevention programs for youths increasingly recognize interactive computer technology as a potential avenue for health education and intervention. Children and teenagers use computers and the Internet more than any other age group. Of those aged 5 to 17 years, 90% use computers; 75% of teenagers surf the Internet (U.S. Department of Commerce, 2002). These trends notwithstanding, investigators have only begun to experiment with technological delivery modes for prevention programming. Nearly all science-based adolescent drug abuse and other prevention programs are delivered via small group format, despite the myriad advantages to computer-based interventions (Rotheram-Borus, 2000).
CD-ROM and the Internet are the two prevailing modes for computer-based interventions. Both technologies have their advantages. The Internet can be accessed from the home, school, or such community agencies as libraries and youth service organizations. But dial-up modems, which are used by 80% of Internet users, are slow. Highly innovative interactive programs need broadband service to run optimally. Though the Internet holds greater potential, the current standard for delivering fast-paced, interactive prevention programming is CD-ROM.
CD-ROM
Youths who receive prevention programs via CD-ROM can access and navigate through topic modules at their own pace. Interactively presented content is stimulating and varied and permits skills demonstrations and guided rehearsal. Young people enjoy unique character designs and animations, complex graphics, and judiciously placed text. The branching technology available to CD-ROM programming allows for the development of multiple story lines that play according to the choices youths make. Youths benefit by interacting with tailored sessions based on their current skill level. Further, researchers cognizant of their target population can incorporate developmentally and culturally tailored audio, animation, graphics, and video into the CD-ROM.
Protocol fidelity, portability, ease of use, and data storage associated with CD-ROM technology can benefit research design and dissemination capabilities. CD-ROM allows investigators to distribute prevention programs, knowing that youths will receive the evaluated intervention. More than 10 hours of interactive content can be stored on one portable disk and delivered to anyone with access to a computer and CD-ROM drive.
Cost also favors CD-ROM. At present, a science-based, adult-led prevention program, including the necessary training and materials, costs between $500 and $900 for a classroom of 30 students. CD-ROMs greatly reduce the need for program materials and staff training; they can reach each child in a class of 30 students for a total cost of less than $60.00.
The Digital Divide
No discussion of Internet usage and computer accessibility can neglect the “digital divide.” This refers to the gap between people and communities who can make effective use of new information technology and those who cannot (Digital Divide Network, 2002). Debate as to whether the “divide” is shrinking or expanding continues. In 1998, 37% of homes in the United States were equipped with computers. By 2001, that number had increased to 57%. Over those same 4 years, Internet use increased from 19% to 51% (U.S. Department of Commerce, 2002). Demographic statistics, however, reveal ethnic-racial gaps in computer ownership and Internet use.
By the end of 2001, Asian and White Americans’ computer use was roughly 70%, whereas African-Americans’ and Latinos’ use was 56% and 49%, respectively (U.S. Department of Commerce, 2002). The digital divide is also apparent in Internet use. About 30% fewer African-Americans and Latinos are online compared to Asian and White Americans.
Minority youths with the least access to computers and the Internet are at greatest risk for substance abuse. Compared to Whites, Blacks have higher substance-related mortality and morbidity (National Cancer Institute, 1991). A higher percentage of Latino youths, compared to Whites and Blacks, have tried alcohol before they are 13 years old (Centers for Disease Control and Prevention, 2001). Despite the logic of directing prevention efforts at minority children, gaps remain in the science of preventing alcohol and other substance abuse among African-American, Latino, economically disadvantaged, and other high-risk youths. The study described in this article aimed to bridge some of those gaps. In so doing, the study examined the feasibility and preliminary effectiveness of an interactive CD-ROM designed to prevent alcohol abuse among high-risk youths.
METHODS
Setting and Participants
Study participants were 489 youths from greater New York City, and parts of New Jersey and Delaware. Youths were recruited from 43 afterschool agencies that serve economically disadvantaged children and adolescents. These sites were primarily afterschool drop-in centers, clubs, neighborhood centers, and other youth organizations. Based on Census data from 2000 and the zip codes in which the agencies are located, family household incomes were at or below the Federal poverty line of $17,050 for a family of five (U.S. Department of Health and Human Services, 2000).
Study participants assented to research involvement and their parents or legal guardians provided informed consent. Though all participants were English speaking, consent forms were made available in Spanish for parents who were not comfortable with English. The Institutional Review Board at Columbia University approved consent procedures.
At baseline 51.4% of the sample was female and the median age was 10.84 years. Most of the participants were from ethnic-racial minority groups: 54% were African-American, 30% were Hispanic, 11% were White, and 5% were from other ethnic-racial groups.
Design
Prior to pretesting, participants were randomly assigned to one of three arms: control, CD-ROM intervention, and parent-enhanced CD-ROM intervention. Eleven sites (youth n = 160) were assigned to the control arm and 26 sites (youth n = 329) were assigned to the intervention arms. Participants in the control arm completed pretest and posttest measurements only. Participants in both intervention arms completed pretest measurements, received the CD-ROM intervention, and were posttested.
Measures
On forms kept separate from other measures, informed and consenting youths reported various demographic and tracking information. Assertion skills were measured by asking youths to define the word assertiveness and answer questions about their ability to intercede if their friends were about to get into trouble and their ability to stop socializing with friends who could get them into trouble. This skill was measured by adapting the short form of the Children’s Action Tendency Scale (Deluty, 1979, 1984). Youths’ ability to perceive harm was measured on a 5-point Likert scale by asking “How often do people hurt themselves when they drink alcohol?”
Included in the schedule were questions related to self-efficacy, problem solving, educational attainment, peer interactions, and family rules related to alcohol and substance use. Peer substance use associations were measured by asking participants how many of their five closest friends drink alcohol; have ever been drunk; smoke marijuana; smoke cigarettes; sniff inhalants; or use crank, heroin, ecstasy, or any other drug. Alcohol and other substance use were self-reported.
Intervention Content
Youths in the intervention arm received the interactive CD-ROM prevention program Thinking Not Drinking: A SODAS City Adventure. Thinking Not Drinking is a skills-based program that consists of ten, 45-minute sessions. Grounded in the frameworks of social cognitive theory, problem-behavior theory, peer-cluster theory, and family-networks theory, the sessions cover goal setting, coping, media literacy, peer pressure, and assertiveness training, as well as such preventive strategies as norm correcting, decision making, and effective communication. The CD-ROM emphasizes prevention strategies thematically through a specific problem-solving sequence.
The problem-solving approach, which provides a context for learning and applying alcohol abuse prevention content, is central to other substance abuse prevention programs (Botvin, Baker, Dusenbury, Tortu, & Botvin, 1990; Botvin, Epstein, Baker, Diaz, & Ifill-Williams, 1997; Hawkins, Catalano, Kosterman, Abbott, & Hill, 1999; Schinke, Botvin, & Orlandi, 1991). The problem-solving approach also lends itself to relatively straightforward programming, provides engaging interactive material, and equips youths with a practical skill set to understand, integrate, and apply all other elements of the alcohol abuse prevention program.
Each session in the CD-ROM begins with skill-specific objectives youths must meet to advance to the next session. Navigating through an edgy urban landscape, youths encounter simulated yet realistic obstacles and distractions depicted by animated characters mimicking the age, gender, and demographic background of the target adolescents. To successfully maneuver through each session, youths must employ specific problem-solving skills. A principal character, acting as the youths’ conscience, guides youths through the core problem-solving sequence of Stop, Options, Decide, Act, and Self-praise.
In the Stop step, youths learn to pause and define problems and to identify their responsibility in solving problems related to alcohol abuse use and other personal issues. In the second step, Options, youths interact with a process for learning how to generate, consider, and evaluate alternative solutions to problems. For the Decide step, youths choose what they consider the best solution from the generated list of alternatives by assessing each option on its costs and benefits.
In Act, the fourth step, youths are provided the opportunity to witness the consequences of their decision, whether or not the choice is correct. If youths pick the appropriate choice, they see the positive results of their decision making. If they select an incorrect option, they are rerouted to the original list of options, but only after they have witnessed the negative consequences of the poor decision. Youths are then asked to Decide and Act again, until the correct option is chosen and the positive consequence experienced.
In the Self-praise step, youths see how to reward themselves for engaging in the problem-solving sequence, regardless of the outcome of the options they selected. Since youths cannot control the way others react to their problem-solving responses in everyday situations, the self-praise step provides a predictable reward that youths can give to themselves when they correctly use problem-solving techniques–regardless of the consequences.
Procedure
Most youths completed the 10-session intervention at the collaborating afterschool agency from which they were recruited. During the course of delivery intervention, some study participants moved away from or stopped attending their afterschool program. In these instances, youths completed the intervention in the research offices or on laptop computers in their homes. Youths with adequate home computers were provided copies of the game. Each intervention session took approximately 45 minutes to complete and was intended to be completed weekly.
Columbia University research assistants collected pretest data on all 489 participants at collaborating sites. At posttest, the majority of data were collected via telephone because many youths had stopped attending their sites and others had moved beyond the study area. To protect participants’ privacy, the survey delivery plan precluded family members’ interpreting youths’ responses. Participants received a mailer containing a survey answer booklet in advance of the telephone survey. During the posttest telephone survey, data collectors read each survey item and participants responded with the letter that represented their answer.
Data Analysis and Results
Quantitative
Outcome data were coded, cleaned, entered and analyzed according to measurement protocol for each schedule. Data analyses proceeded with SPSS for Windows.TM Table 1 shows no differences between intervention and control arms on participants’ age, gender, or school grades. Family composition and race differed between the two groups. Divorced or separated households accounted for 46.3% of intervention families; only 35% of participants in the control arm were in divorced or separated families. Ethnic-racial background also was not evenly distributed between the two groups.
TABLE 1.
Demographic Characteristics of Study Population
| CD and Parent Group (n = 329) % | Control (n = 160) % | df | χ2 | p | |
|---|---|---|---|---|---|
| Age (in years) | 5 | 1.916 | ns | ||
| 9 | 7.6 | 6.9 | |||
| 10 | 32.5 | 28.9 | |||
| 11 | 35.9 | 35.8 | |||
| 12 | 19.8 | 23.9 | |||
| 13 and older | 4.3 | 4.4 | |||
| Gender | 1 | .002 | ns | ||
| Female | 51.4 | 51.6 | |||
| Male | 48.6 | 48.4 | |||
| Parents Divorced | 2 | 9.580 | .008 | ||
| Yes | 46.3 | 35.0 | |||
| No | 43.3 | 58.1 | |||
| Don’t Know | 10.4 | 6.9 | |||
| Race | 3 | 22.791 | .001 | ||
| Hispanic | 35.8 | 21.8 | |||
| Black | 37.7 | 58.9 | |||
| White | 14.5 | 7.4 | |||
| Other | 11.9 | 11.9 | |||
| School Grades | 4 | 2.976 | ns | ||
| Excellent | 31.3 | 25.6 | |||
| Very Good | 8.2 | 18.8 | |||
| Good | 40.7 | 41.9 | |||
| Not Good | 8.5 | 12.5 | |||
| Poor | 1.3 | 1.2 |
Gain score analyses were employed for outcome tests. These scores were derived arithmetically by subtracting participants’ pretest scores from their posttest scores on the same items. By analyzing gain scores with two-sample, independent t tests, the significance of between-arm differences in participants’ outcome scores from the pretest measurement occasion to the posttest measurement occasion was determined.
Figure 1 shows that youths assigned to the intervention arm scored more positively on assertion skills and perceived harm of alcohol than participants assigned to the control arm. At pretest, intervention and control participants scored 1.15 on a 2-point scale for assertion skills, where 1 = wrong definition of assertion and 2 = correct definition. At posttest, control participants were unchanged, and intervention participants increased to 1.36, t(472) = 4.01, p < .0005 (two-tailed).
FIGURE 1.
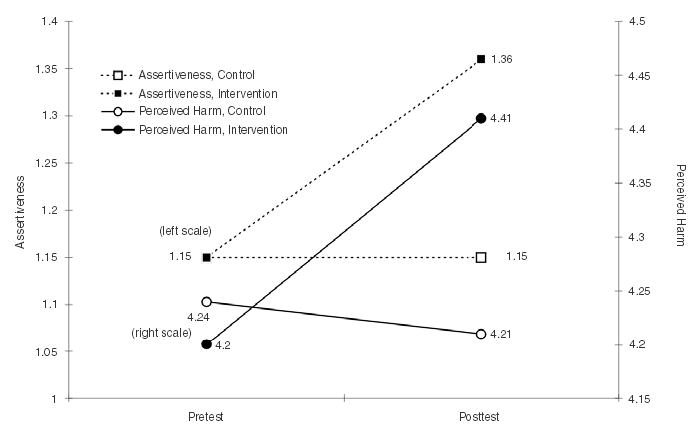
Pretest to Posttest Gain Series: Intervention and Control Arms
As seen in Figure 1, participant scores at pretest did not differ significantly (Intervention = 4.20, Control = 4.24) when asked to rate their perceived harm of alcohol on a 5-point scale, with 1 = never harmful and 5 = always harmful. At posttest, intervention participants scored higher with a mean of 4.41, whereas control participants scored 4.21, t(485) = 1.94, p < .053 (two-tailed).
Not surprisingly, no differences were found for substance use association or participant alcohol and drug use. At pretest, youths’ mean age was 10.83 years; at posttest, approximately 9 months later, their mean age was 11.59 years. Though these young ages are desirable for targeting alcohol and substance use prevention programs, detecting behavior change among early adolescents is difficult. The frequency of substance abuse behavior is low. Behavioral outcomes on the effectiveness of the CD-ROM intervention are not expected until subsequent follow-up measures.
Qualitative
As a result of random assignment, some collaborating sites had higher functioning computers than others. No site was expelled from the study based on computer quality. Complications arose at less than one-third of the 26 intervention sites. In these instances, the existing RAM (Random Access Memory) on the computers was insufficient for adequate interaction with the CD-ROM. The necessary upgrades in RAM were arranged, and this gift fostered a positive relationship with agency staff.
Once the appropriate platform was achieved, SODAS City met with enthusiasm from collaborating sites, parents, and youths. Site staff appeared to value the ease with which they could implement the intervention and often asked if they could provide the game to youths who were not in the study (which was possible because of the randomized block design that assigned sites to arms). After the 10 sessions were delivered, several site directors asked to enroll incoming youths into the program (which was not possible because of the absence of consent and baseline data). As a result of their positive experiences with the software, site staff have requested other types of CD-ROM interventions when they become available.
Uniformly positive feedback has come from youth participants in the intervention arm. Of the 329 participants, only three youths attrited. At sites, youths were enthusiastic about interacting with the CD-ROM; often staff had to ensure that no more than one episode was played per session. Over the intervention delivery period, the investigators received a number of telephone calls from youths wondering when they were to receive additional program content. Several requested that SODAS City be sent home to sisters, brothers, and friends.
DISCUSSION AND CONCLUSIONS
Modest findings from this feasibility study suggest that new technologies, specifically CD-ROM technology, hold promise for transmitting alcohol abuse prevention program content to high-risk youths. Through interactive skills-based sessions, participants in the intervention arm showed an increased understanding of assertiveness. Youths practiced being assertive and witnessed the benefits of assertion through simulated real-life scenarios.
The data suggest that youths who interacted with the 10-session CD-ROM were more cognizant of the harmful effects of alcohol. Again, this message was gained through interactive play rather than passive listening. Given multiple opportunities to see the negative consequences of using alcohol, intervention participants moved in the desired outcome direction; control participants’ measured perceived harm of alcohol remained unchanged.
The positive trends in intervention participants’ assertion skills and perceived harm of alcohol are protective factors to help children and adolescents avoid problems with alcohol and other substance use. Assertion skills help youths to distinguish among assertive, aggressive, and passive behaviors while increasing their social proficiency and resiliency. With respect to decisions regarding alcohol and substance use, youths with an increased perception of the harm of alcohol and increased assertiveness are more likely to make decisions away from alcohol and drug use.
The lack of change in alcohol and substance use between intervention and control arms was somewhat disappointing. But the absence of behavior change is understandable and arguably appropriate, considering the low base rates of drinking and substance use among members of the young sample at pretest and in light of the close proximity of posttesting to intervention. Because study participants were from urban areas, generalization of any findings to all American youths is unwarranted.
Despite these limitations, the study has strengths. During 10 interactive sessions, youths rehearsed real-life situations, experienced the consequences of poor decision making, and compared those results with the outcomes of better decision making. High-quality graphics, attention to cultural nuances and challenging yet age-appropriate objectives ensured successful engagement with the participants. The use of CD-ROM technology was feasible for delivering alcohol abuse prevention material. Study sites implemented the program quickly and easily, without burdensome materials and labor intensive training.
For schools and social service agencies, time and money are precious commodities. Effective prevention programs that can be implemented without depleting resources will likely be preferred to programs that are costly and time-consuming. The portability of our CD-ROM was helpful when participants moved or stopped attending their afterschool program. When these displaced youths gained access to a computer, they could participate fully in the research, receiving intervention identical to other participants. Although initial development and creative costs were high, the final program was duplicated and packaged for less than $1.00 per child.
Additional work with CD-ROM technology in the field of alcohol abuse and other prevention science is warranted. Investigators must and will continue to use the latest tools available to reach target youths with effective programs. Doubtless, we will observe the development of interactive prevention programs online in the future. Until Internet accessibility is pervasive and content is not limited by bandwidth, prevention should continue to explore the exciting and aforementioned advantages of CD-ROM technology. Perhaps the present research will aid in that exploration.
Acknowledgments
The authors extend their sincere thanks to United Neighborhood Houses, Police Athletic League, and the numerous other organizations throughout greater New York City, New Jersey, and Delaware without whose handsome support this research would not have been possible.
Footnotes
[Haworth co-indexing entry note]: “Alcohol Abuse Prevention Among High-Risk Youth: Computer- Based Intervention.” Schinke, Steven P., Traci M, Schwinn, and Alfred J. Ozanian. Co-published simultaneously in Journal of Prevention & Intervention in the Community (The Haworth Press, Inc.) Vol. 29, No. 1/2, 2005, pp. 117-130; and: Technology Applications in Prevention (ed: Steven Godin) The Haworth Press, Inc., 2005, pp. 117–130. Single or multiple copies of this article are available for a fee from The Haworth Document Delivery Service [1-800-HAWORTH, 9:00 a.m. - 5:00 p.m. (EST). E-mail address: docdelivery@haworthpress.com].
This research was supported in full by a generous grant from the National Institute on Alcoholism and Alcohol Abuse, AA11924.
References
- Botvin GJ, Baker E, Dusenbury LD, Botvin EM, Diaz T. Long-term follow-up results of a randomized drug abuse prevention trial in a White middle-class population. Journal of the American Medical Association. 1995;273:1106–1112. [PubMed] [Google Scholar]
- Botvin GJ, Baker E, Dusenbury L, Tortu S, Botvin EM. Preventing adolescent drug abuse through a multimodal cognitive-behavioral approach: Results of a 3-year study. Journal of Consulting & Clinical Psychology. 1990;58:437–446. doi: 10.1037//0022-006x.58.4.437. [DOI] [PubMed] [Google Scholar]
- Botvin GJ, Epstein JA, Baker E, Diaz T, Ifill-Williams M. School-based drug abuse prevention with inner-city minority youths. Journal of Child & Adolescent Substance Abuse. 1997;6:5–19. [Google Scholar]
- Botvin GJ, Kantor LW. Preventing alcohol and tobacco use through life skills training. Alcohol Health & Research World. 2000;24:250–257. [PMC free article] [PubMed] [Google Scholar]
- Centers for Disease Control and Prevention. (2001). Youth 2001 Online: Alcohol/Other Drug Use. In Youth Risk Behavior Surveillance System Retrieved July 30, 2002, from http://apps.nccd.cdc.gov/YRBSS/GraphV.asp
- Centers for Disease Control and Prevention. Youth Risk Behavior Surveillance–United States, 1999. Morbidity and Mortality Weekly Report: CDC Surveillance Summaries. 2000;49(No SS5):1–94. [PubMed] [Google Scholar]
- Deluty RH. Behavioral validation of the Children’s Action Tendency Scale. Journal of Behavioral Assessment. 1984;6:115–130. [Google Scholar]
- Deluty RH. Children’s Action Tendency Scale: A self-reported measure of aggressiveness, assertiveness, and submissiveness in children. Journal of Consulting and Clinical Psychology. 1979;47:1061–1071. doi: 10.1037//0022-006x.47.6.1061. [DOI] [PubMed] [Google Scholar]
- Digital Divide Network. (2002). Digital Divide Basics Retrieved July 31, 2002, from http://www.digitaldividenetwork.org/content/sections/index.cfm?key=2
- Grant BF, Dawson DA. Age at onset of alcohol use and association with DSM-IV alcohol abuse and dependence: Results from the National Longitudinal Alcohol Epidemiologic Survey. Journal of Substance Abuse. 1997;9:103–110. doi: 10.1016/s0899-3289(97)90009-2. [DOI] [PubMed] [Google Scholar]
- Hawkins JD, Catalano RF, Kosterman R, Abbott R, Hill KG. Preventing adolescent health-risk behaviors by strengthening protection during childhood. Archives of Pediatric & Adolescent Medicine. 1999;153:226–234. doi: 10.1001/archpedi.153.3.226. [DOI] [PubMed] [Google Scholar]
- Johnston, L. D., O’Malley, P. M., & Bachman, J. G. (2002). Monitoring the Future national results on adolescent drug use: Overview of key findings, 2001 Rockville, MD: National Institute on Drug Abuse.
- National Cancer Institute. (1991). Cancer among blacks and other minorities: Statistical profiles. Bethesda, MD: U.S. Department of Health and Human Services.
- National Institute on Alcohol Abuse and Alcoholism. (1998). Drinking in the United States: Main Findings from the 1992 National Longitudinal Alcohol Epidemiologic Survey (NLAES). In US Alcohol Epidemiologic Data Reference Manual (Vol. 6). Bethesda, MD: Author.
- Rotheram-Borus MJ. Expanding the range of interventions to reduce HIV among adolescents. AIDS. 2000;14(Suppl 1):S33–S40. doi: 10.1097/00002030-200006001-00005. [DOI] [PubMed] [Google Scholar]
- Scheier L, Botvin GJ, Griffin KW. Preventive intervention effects on developmental progression in drug use: Structural equation modeling analyses using longitudinal data. Prevention Science. 2001;2(2):91–112. doi: 10.1023/a:1011543730566. [DOI] [PubMed] [Google Scholar]
- Schinke, S. P., Botvin, G. J., & Orlandi, M. A. (1991). Substance abuse in children and adolescents Newbury Park, CA: Sage Publications.
- Schinke SP, Gordon AN, Weston RE. Self-instruction to prevent HIV infection among African-American and Hispanic-American Adolescents. Journal of Consulting and Clinical Psychology. 1990;58:432–436. doi: 10.1037//0022-006x.58.4.432. [DOI] [PMC free article] [PubMed] [Google Scholar]
- U.S. Department of Commerce, Economics and Statistics Administration National Telecommunications and Information Administration. (2002, February). A Nation Online: How Americans Are Expanding Their Use of the Internet Retrieved July 27, 2002, from http://www.ntia.doc.gov/ntiahome/dn/
- U.S. Department of Health and Human Services. (2000). The 2000HHS Poverty Guidelines Retrieved July 28, 2002, from http://aspe.hhs.gov/poverty/00poverty.htm