

Abstract
Dextrocardia associated with atrial situs solitus is commonly referred to as dextroversion. Dextroversion is a result of early interruption of normal embryological development and, therefore, rarely occurs without other associated cardiac and noncardiac anomalies. While percutaneous coronary intervention has been described in many cases of dextrocardia with situs inversus, it has not been previously described in dextroversion. We report the case of an 88-year-old woman with dextroversion who presented with an acute anterior myocardial infarction that was successfully treated with coronary stent implantation.
Dextrocardia in its various forms is a relatively rare congenital anomaly, with an estimated incidence of 1 in 10,000 (1). While variations in terminology and classification systems exist, the condition of dextrocardia with situs solitus is commonly referred to as dextroversion (2, 3). We report the case of a patient with known dextroversion but no other known cardiac or noncardiac anomalies who presented with an anterior myocardial infarction that was successfully treated with primary percutaneous stent implantation.
CASE REPORT
An 88-year-old Caucasian woman with a history of hypertension and type 2 diabetes mellitus presented with a complaint of substernal chest pressure accompanied by dyspnea and nausea. Despite the resolution of chest pressure and dyspnea, the patient continued to experience nausea for the next 10 hours and then sought treatment in the emergency department. She had no history of cardiac problems and no family history of coronary artery disease. The patient's social history revealed no tobacco, alcohol, or illicit drug use.
In the emergency department, her heart rate was 88 beats per minute, and her blood pressure was 149/75 mm Hg. She was breathing 14 times per minute with a pulse oximetric saturation of 92% on room air. Neck examination revealed no jugular venous distension and normal carotid upstrokes without bruits. Auscultation of the lungs revealed bibasilar crackles. The point of maximum impulse was located in the fourth intercostal space just left of the right midclavicular line. Cardiac auscultation demonstrated a regular rate and rhythm with a normal first and second heart sound. No murmurs, rubs, or gallops were heard. No clubbing, cyanosis, or edema was noted.
The admitting electrocardiogram demonstrated an acute injury pattern in leads V1 and V2 (Figure 1). Given the physical findings of a right-sided point of maximum impulse, a right-sided electrocardiogram was also performed and revealed an acute injury pattern throughout the right precordial leads (Figure 2). The initial chest x-ray also confirmed dextrocardia with a left-sided aortic knob (Figure 3). The patient's initial troponin I and creatine kinase–MB levels were 4.2 ng/mL and 8.3 ng/mL, respectively.
Figure 1.
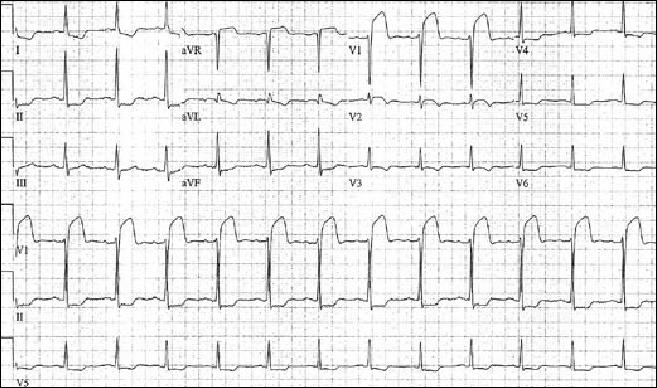
Admitting electrocardiogram.
Figure 2.

Right-sided electrocardiogram.
Figure 3.
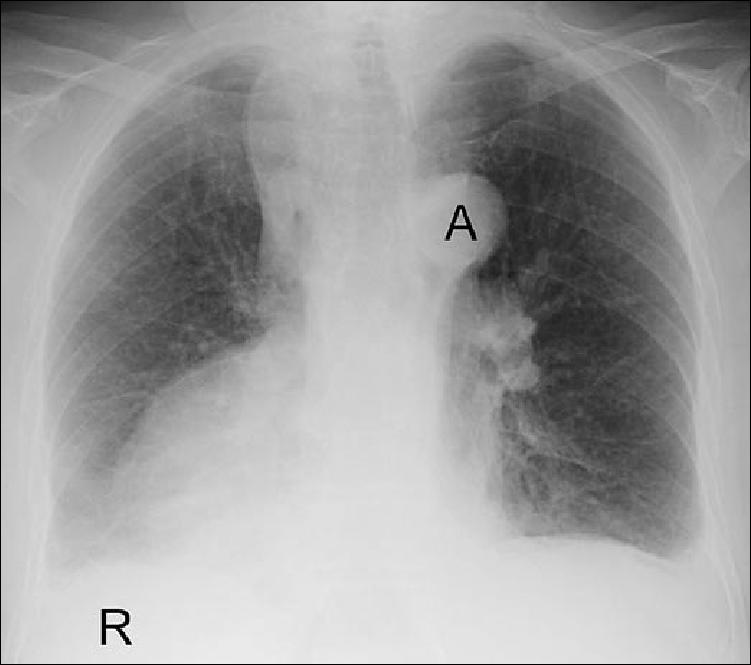
Chest x-ray. A indicates aorta.
The patient was taken for emergent cardiac catheterization. Coronary angiography of the right coronary artery was performed with a Judkins right 4 catheter, while the left main coronary artery was engaged with a Judkins left 4 catheter. Angiography demonstrated nonsignificant obstructive disease in the right coronary and left circumflex arteries and a 90% lesion in the proximal left anterior descending artery (Figure 4). This lesion was successfully treated with a Guidant Vision 3.0 × 23-mm stent through a Cordis 3.0 XB guide catheter (Figure 5).
Figure 4.

Left anterior descending artery with a proximal 90% lesion (arrow).
Figure 5.

Left anterior descending artery after stent implantation.
The patient subsequently underwent cardiac magnetic resonance imaging to assess left ventricular function and to determine the extent of myocardial damage. Near transmural hyperenhancement was identified in the anterior, anteroseptal, and anterolateral walls extending from midventricle to the apex. (The specifics of magnetic resonance imaging in this case report have been described elsewhere [4].)
DISCUSSION
Coronary angiography and coronary interventional procedures have been well described in cases of dextrocardia and situs inversus (5–8). Coronary artery bypass grafting has also recently been described in a dextroverted heart (9). This case is the first reported instance of acute myocardial infarction occurring in a patient with dextroversion (congenital dextrocardia with visceral and atrial situs solitus) who was successfully treated with coronary stent implantation.
There have been several reported approaches to classify cardiac malposition (10–12). The simplest method is to describe cardiac position, visceroatrial situs, and ventriculoarterial position. Dextroversion refers to cases of dextrocardia with normally related atria (atrial situs solitus). In this case, the viscera are also in their normal location, i.e., there is no visceral heterotaxy. Lastly, normal D-loop (noninverted) configuration of the ventricles without transposition of the great vessels is also observed. From a developmental standpoint, dextroversion results from rotation of the cardiac apex to the right instead of left hemithorax during embryogenesis, resulting in anterior left-sided and posterior right-sided chambers. Due to interruption of normal rotation, dextroversion, unlike dextrocardia with situs inversus, is associated with cardiac anomalies in >90% of cases (3, 11, 13).
The incidence of dextroversion is unknown. In a Mayo Clinic series between 1960 and 1970, 60 cases of dextrocardia were studied with angiography. Dextroversion was observed in 44 instances (73%), while dextroversion without inverted ventricles and arterial transposition occurred in 8 (13%) of the 60 cases (14). In a recent 10-year retrospective review of 125 echocardiographically confirmed cases of dextrocardia, dextroversion occurred in 43 cases (34%). Only 17 cases of dextroversion occurred with concordant atrioventricular and ventriculoarterial connections, and only two of these cases occurred without any cardiac abnormality (13).
The incidence of coronary artery disease in dextrocardia is no different than in the general population (15). The high percentage of serious cardiac anomalies occurring in patients with dextroversion, however, often precludes adult survival and, therefore, the development of coronary artery disease. In a review of myocardial infarction and dextrocardia, Ptashkin et al came across nine cases in the literature, with only one case occurring with situs solitus (16). However, with further advances in the surgical repair of congenital heart defects, more adult patients with dextroversion will present with acquired heart diseases. No difference is expected in the clinical course or prognosis after an acute myocardial infarction between patients with and without dextrocardia. The presentation may vary only in that the patient may complain of right-sided as opposed to left-sided chest pain (16).
Dextrocardia can provide challenges during coronary angiography and intervention. In the first reported case of percutaneous coronary intervention in dextrocardia with situs inversus, Moreyra et al advocated using multipurpose catheters because their flexible tips allowed for easy manipulation into the coronary ostia (5). Several authors since then have employed standard Judkins catheters during coronary intervention (6–8). Because the aorta is a mirror image in dextrocardia with situs inversus, the Judkins catheters can be used in mirror-image fashion. In other words, a Judkins right catheter can engage the left-sided, morphological right coronary artery, while the Judkins left catheter can be used for the right-sided, morphological left coronary artery. In our patient, the aorta was left-sided, with the coronary artery ostia being located close to their usual positions, allowing for standard Judkins catheter use. In most cases of dextrocardia, whether situs solitus or situs inversus, the choice of diagnostic and interventional guide catheters can be predicted by the position of the aorta (8).
Counterclockwise rotational movements or torquing should be used in cases of dextrocardia with situs inversus in contrast to those used in normal cardiac anatomy (6–8). In addition, interpretation of angiographic images may also be difficult and unfamiliar. Image appearance, therefore, can be improved by horizontally reversing the image and/or inverting the position (i.e., right-left substitution) of the x-ray image intensifier during the procedure (17). In this case, normal rotational movements and image acquisition techniques were successfully employed.
CONCLUSION
Myocardial infarction in the setting of isolated dextroversion is rare. While myocardial infarction and percutaneous coronary intervention have been extensively described in cases of dextrocardia with situs inversus, no cases have been reported with dextroversion. Our experience in this case demonstrates that coronary angiography and intervention can be performed in cases of dextroversion with ease using standard catheterization techniques.
References
- 1.Rosenberg HN, Rosenberg I. Simultaneous association of situs inversus, coronary heart disease, and hiatus hernia. Ann Intern Med. 1949;(30):851–859. doi: 10.7326/0003-4819-30-4-851. [DOI] [PubMed] [Google Scholar]
- 2.Welsh RA, Felson B. Uncomplicated dextroversion of the heart. Radiology. 1956;66(1):24–32. doi: 10.1148/66.1.24. [DOI] [PubMed] [Google Scholar]
- 3.Grant RP. The syndrome of dextroversion of the heart. Circulation. 1958;18(1):25–36. doi: 10.1161/01.cir.18.1.25. [DOI] [PubMed] [Google Scholar]
- 4.Salanitri J, Welker M, Pereles FS. Magnetic resonance imaging of acute myocardial infarction in dextrocardia with situs solitus (dextroversion) Australas Radiol. 2005;49(5):422–426. doi: 10.1111/j.1440-1673.2005.01476.x. [DOI] [PubMed] [Google Scholar]
- 5.Moreyra AE, Saviano GJ, Kostis JB. Percutaneous transluminal coronary angioplasty in situs inversus. Cathet Cardiovasc Diagn. 1987;13(2):114–116. doi: 10.1002/ccd.1810130208. [DOI] [PubMed] [Google Scholar]
- 6.Gaglani R, Gabos DK, Sangani BH. Coronary angioplasty in a patient with dextrocardia. Cathet Cardiovasc Diagn. 1989;17(1):45–47. doi: 10.1002/ccd.1810170111. [DOI] [PubMed] [Google Scholar]
- 7.Blankenship JC, Ramires JA. Coronary arteriography in patients with dextrocardia. Cathet Cardiovasc Diagn. 1991;23(2):103–106. doi: 10.1002/ccd.1810230207. [DOI] [PubMed] [Google Scholar]
- 8.Robinson N, Golledge P, Timmis A. Coronary stent deployment in situs inversus. Heart. 2001;86(5):E15. doi: 10.1136/heart.86.5.e15. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Totaro P, Coletti G, Lettieri C, Pepi P, Minzioni G. Coronary artery bypass grafts in a patient with isolated cardiac dextroversion. Ital Heart J. 2001;2(5):394–396. [PubMed] [Google Scholar]
- 10.Daves ML, Pryor R. Cardiac positions: a primer. Am Heart J. 1970;79(3):408–421. doi: 10.1016/0002-8703(70)90429-1. [DOI] [PubMed] [Google Scholar]
- 11.Rao PS. Dextrocardia: systematic approach to differential diagnosis. Am Heart J. 1981;102(3 Pt 1):389–403. doi: 10.1016/0002-8703(81)90315-x. [DOI] [PubMed] [Google Scholar]
- 12.Van Praagh R, Van Praagh S, Vlad P, Keith JD. Anatomic types of congenital dextrocardia: diagnostic and embryologic implications. Am J Cardiol. 1964;(13):510–531. doi: 10.1016/0002-9149(64)90159-6. [DOI] [PubMed] [Google Scholar]
- 13.Garg N, Agarwal BL, Modi N, Radhakrishnan S, Sinha N. Dextrocardia: an analysis of cardiac structures in 125 patients. Int J Cardiol. 2003;88(2–3):143–155. doi: 10.1016/s0167-5273(02)00539-9. [DOI] [PubMed] [Google Scholar]
- 14.Squarcia U, Ritter DG, Kincaid OW. Dextrocardia: angiocardiographic study and classification. Am J Cardiol. 1973;32(7):965–977. doi: 10.1016/s0002-9149(73)80166-3. [DOI] [PubMed] [Google Scholar]
- 15.Hynes KM, Gau GT, Titus JL. Coronary heart disease in situs inversus totalis. Am J Cardiol. 1973;31(5):666–669. doi: 10.1016/0002-9149(73)90341-x. [DOI] [PubMed] [Google Scholar]
- 16.Ptashkin D, Stein E, Warbasse JR. Congenital dextrocardia with anterior wall myocardial infarction. Am Heart J. 1967;74(2):263–267. doi: 10.1016/0002-8703(67)90287-6. [DOI] [PubMed] [Google Scholar]
- 17.Goel PK. Double-inversion technique for coronary angiography viewing in dextrocardia. Catheter Cardiovasc Interv. 2005;66(2):281–285. doi: 10.1002/ccd.20473. [DOI] [PubMed] [Google Scholar]