

Abstract
Objective
We hypothesized that increasing brain serotonin in healthy individuals with high scores on 2 self-report measures of trait quarrelsomeness would reduce quarrelsome behaviours and enhance agreeable behaviours when measured ecologically using an event-contingent recording method.
Methods
We conducted a double-blind crossover study, in which participants took tryptophan (3 g/d) and placebo for 15 days each and recorded how they behaved, felt and perceived others during everyday social interactions.
Results
Tryptophan significantly decreased quarrelsome behaviours and increased agreeable behaviours and perceptions of agreeableness. Men also behaved less dominantly, whereas both men and women perceived others as more dominant.
Conclusion
Tryptophan's effects on behaviours and perceptions, while more marked in the men, were generally positive and accompanied by improved affect. Increasing serotonin in quarrelsome people may not only reduce behaviours associated with a predisposition to various mental and physical disorders but also enhance socially constructive behaviours and improve social perceptions.
Medical subject headings: affect, aggression, serotonin, social behaviour, social perception, tryptophan
Abstract
Objectif
Nous avons posé en hypothèse que l'élévation de la concentration de sérotonine cérébrale chez des sujets en bonne santé qui ont des résultats élevés à deux mesures autodéclarées du caractère belliqueux réduirait les comportements belliqueux et améliorerait les comportements affables lorsqu'on les mesure écologiquement au moyen d'une méthode de consignation contingente des événements.
Méthodes
Nous avons réalisé un essai croisé à double insu pour lequel les participants ont pris du tryptophane (3 g/j) et un placebo pendant 15 jours chacun et ont consigné leur comportement, leurs sentiments et leur perception à l'égard d'autrui pendant les interactions sociales quotidiennes.
Résultats
Le tryptophane réduit considérablement les comportements belliqueux et accroît les comportements affables et les perceptions d'un caractère affable. Les hommes se sont aussi comportés de façon moins dominante tandis que les hommes et les femmes percevaient les autres comme plus dominants.
Conclusion
Même s'ils sont plus marqués chez les hommes, les effets du tryptophane sur les comportements et les perceptions ont en général été positifs et ont entraîné une amélioration de l'affect. L'élévation de sérotonine chez les personnes belliqueuses peut non seulement atténuer les comportements associés à une prédisposition à divers troubles mentaux et physiques, mais aussi améliorer les comportements socialement constructifs et les perceptions sociales.
Introduction
In monkeys and in humans, levels of various markers of brain serotonin function are negatively associated with impulsive aggression.1–5 For example, in monkeys low levels of 5-hydroxyindoleacetic acid in cerebrospinal fluid predict impulsive–aggressive behaviour and early mortality.6,7 In humans, this serotonergic marker is associated with aggression, as well as with suicide.1 Moreover, impulsive–aggressive behaviour can be elicited by decreasing serotonin experimentally.8–11 Conversely, serotonin-enhancing drugs can decrease inappropriate aggression.9,12,13
Serotonin seems to play a different role in regulating aggression that is used to increase dominance. This is particularly evident in evolutionarily older species such as ants, crayfish and lobsters, in which serotonin-enhancing drugs have been shown to increase aggression during agonistic encounters.14–16 A similar positive relation between serotonin function and dominance-related aggression has been observed in at least 1 species of monkey.17 However, in other monkey species, subordinate group members treated with serotonin-enhancing drugs often achieve dominance by first increasing affiliative behaviours toward group members, thereby creating social support, and only then engaging in aggressive encounters with competitors.18 High serotonin function has been linked to both social status and levels of affiliation.3,19–21 Affiliative behaviour in primates may be a more cost-effective means to establish dominance relationships.
These and other data suggest that the human serotonin system may not only inhibit maladaptive behaviours but also promote socially constructive behaviours. Given the importance of good social functioning for mental well-being and physical health, it is surprising how little information is available concerning the role of serotonin in human social interactions. Only the serotonin–aggression relation has been studied in both patients12 and healthy individuals.8,11 A few volunteer studies have looked at the role of serotonin in other social behaviours. The findings are generally in agreement with data from studies of monkeys and show that serotonin may indeed enhance human affiliation and promote social dominance.22,23 However, measurements were generally limited to standardized social interactions, laboratory settings and single observations. In contrast, Moskowitz et al24 used an event-contingent recording method to study the effects of a serotonergic manipulation on people's social behaviours during social interactions in their everyday lives. Twelve days of tryptophan supplementation resulted in a decrease in quarrelsome behaviours and an increase in dominant behaviours. There were no changes in agreeable behaviours, submissive behaviours and experienced affect.
The present research, using the same event-contingent recording method and tryptophan treatment, aimed to confirm that tryptophan can decrease quarrelsome behaviour and to extend these findings in a group of people with high trait levels of quarrelsomeness. Individuals who are quarrelsome during everyday social interactions are not only prone to impulsive–aggressive behaviour in more extreme situations but also are at risk of depression, suicide, hypertension and heart disease.25–28 Given that in laboratory settings the effects of changed availability of tryptophan on aggression are more pronounced in people with higher self-reported quarrelsomeness,29–31 we expected that the effects of tryptophan in quarrelsome individuals in everyday life would not only include a decrease in quarrelsomeness and an increase in dominance, but also an increase in agreeableness.
Another goal of this study was to further examine the range of effects of tryptophan. Given the reciprocal nature of social interactions, a behavioural change in one person is likely to elicit a behavioural change in others. In our previous study, tryptophan decreased quarrelsome behaviours in individuals who received tryptophan second, but not in those who received tryptophan first.24 We then suggested that a decrease in quarrelsomeness in individuals who received tryptophan in the first treatment phase might have carried over into future social interactions in the subsequent placebo phase, if there was also a change in the behaviour of participants' interaction partners. Two steps were taken to provide a more rigorous test of whether the order effect was the result of a pharmacological carryover or of a change in behaviour in response to changed perceptions of others. The washout between the study phases was increased from 2 to 6 days. In addition, participants in the present study also rated the behaviour of their interaction partners to examine whether there was a perceived change in the behaviour of others. Specifically, it was expected that tryptophan would increase perceptions of agreeableness.
Methods
Participants
The study was approved by the Research Ethics Board of the McGill University Health Centre, Montréal. All participants signed a consent form after the nature of the study had been explained to them. They received monetary compensation for time spent. The study was carried out in accordance with the Canadian Tri-Council Policy Statement: Ethical Conduct for Research Involving Humans (http://www.pre.ethics.gc.ca/english/policystatement/policystatement.cfm).
Participants were recruited via advertisements in local newspapers. Requirements for study participation were the following: working at least 30 hours per week, a high score on 2 questionnaires related to trait quarrelsomeness (see below), absence of current depression and alcoholism, absence of current major medical illness, and no contraindication for the use of tryptophan as mentioned in the product monograph. In Canada, tryptophan is a prescription drug.
Advertisements used to recruit participants included the following statements: Do you have problems with irritability?; Do you repeatedly lose control of your temper?; and Do you get easily agitated? People who telephoned in response to the advertisements were given a brief explanation of the study. Those who were interested in participating were asked about their eligibility. Those who qualified were invited for screening.
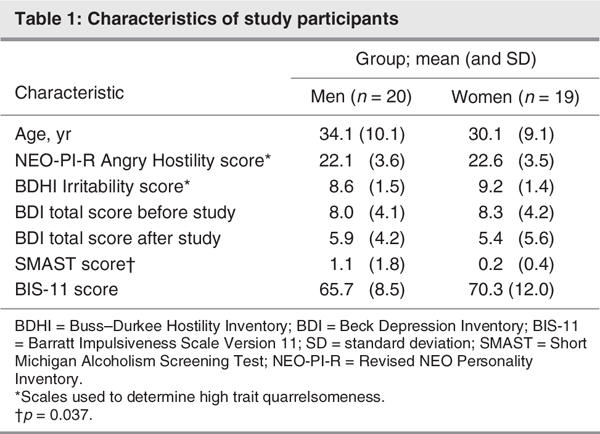
In the laboratory, the study was explained in detail. Informed consent was then obtained, and participants completed the Beck Depression Inventory (BDI),32 the Short Michigan Alcoholism Screening Test (SMAST),33 the Buss–Durkee Hostility Inventory (BDHI)34 and an adapted version of the NEO Five-Factor Inventory that included the entire Angry Hostility subscale of the Revised NEO Personality Inventory (NEO-PI-R).35 Trait quarrelsomeness was based on a person's score on (1) the NEO-PI-R Angry Hostility subscale, which reflects the “tendency to experience anger and related states such as frustration and bitterness,”35 and (2) the BDHI Irritability subscale, which reflects the “readiness to explode with negative affect at the slightest provocation.”34 Only those whose score was at least 1 standard deviation above the population mean on 1 scale and at least half a standard deviation above the population mean on the other were included.34,35
Individuals who met the criteria for high trait quarrelsomeness were interviewed by the collaborating psychiatrist (G.P.). Individuals with current depressed mood as indicated by a BDI score higher than 10 and as determined by the psychiatrist were excluded. Those with probable alcoholism as indicated by a SMAST score higher than 2 and as determined by the psychiatrist were also excluded. Finally, eligibility for taking tryptophan was confirmed. Given ties between irritability, aggression and impulsivity,36 people who entered the study after meeting all criteria also completed the Barratt Impulsiveness Scale Version 11 (BIS-11).37
Screening appointments were made by telephone with 151 people. A total of 46 participants did not show up. Two individuals were no longer interested in participating after reading the consent form. The number of excluded individuals was 57 (2 did not have a job, 8 showed signs of depression, 47 scored below the cutoff on trait quarrelsomeness measures). A total of 46 participants started the study. One man and 1 woman dropped out before the beginning of the second treatment phase; both had been on placebo in the first phase. Three men and 2 women were withdrawn from the sample when they stopped fitting the inclusion criteria during the study (e.g., lost job, became ill). The results are described for the 39 participants (20 men, 19 women) who completed the study. There were no gender differences on the baseline measures of Angry Hostility, Irritability and Impulsiveness, or on the baseline BDI scores, but men scored significantly higher on the SMAST (Table 1). There were no significant treatment order or gender × treatment order effects on the baseline measures.
Table 1
Treatment
We carried out a double-blind crossover study, in which participants took 1 g of L-tryptophan (Tryptan, ICN Canada, Montréal) or an identical placebo 3 times a day with meals for 15 days each. Treatment order was counterbalanced. A 6-day inter-treatment interval was included to ensure washout and to start each treatment phase on the same day of the week. For all participants, both phases started and finished on a Tuesday.
The daily dose of tryptophan given is considered sufficient to maximize serotonin synthesis.38 Tryptophan was chosen over other serotonin-enhancing drugs, because it has a relatively specific effect on brain serotonin,39 it is a dietary component with few side effects and negligible toxic effects when given as a drug,40 and in healthy people it has little if any effect on mood.41
Event-contingent recording
During both treatment phases, participants reported their social interactions. Data were collected using the event-contingent recording method used by Moskowitz et al.24 Treatment length was 15 days, because (1) reliability across days asymptotes after 12 days and does not increase with greater aggregation of the number of days,42 and (2) Moskowitz et al24 showed that data from the first 3 days might need to be excluded, because these days may be affected by participants' tendency to provide socially desirable self-ratings upon entry into the study.
Information was recorded using standardized forms. As before, participants provided information about the context in which each interaction occurred, and they indicated how they felt and behaved. The present study also included a rating of the perceived behaviour of interaction partners. Finally, participants were asked to report whether they had ingested alcohol within 1 hour of a social interaction and not to report an interaction when illicit drugs had been consumed in the 3 hours before an interaction. A brief description of the measures taken from the event-contingent method used is provided below. Readers are referred to Moskowitz et al24 for more details.
Measurement of affect
Each form included 2 methods for measuring affect experienced during a social interaction. First, participants rated the following positive and negative affect adjectives on a scale from 0 to 6:43 worried/anxious, happy, frustrated, pleased, angry/hostile, enjoyment/fun, unhappy, joyful, depressed/blue. Second, participants marked the valence and arousal of their experienced affect on a 9 × 9 affect grid.44 By placing a single mark, they indicated the extent to which they were feeling unpleasant versus pleasant on the horizontal dimension of the grid and the extent of alertness versus sleepiness on the vertical dimension of the grid.
Event-level positive and negative affect scores were constructed by (1) adding up the individual adjective scores corresponding to positive and negative affect and (2) dividing each sum score by the number of adjectives to provide a mean. The difference between mean positive affect and mean negative affect provided a composite measure of affect. In addition, event-level affect valence and affect arousal scores were coded from the affect grid using a number between 1 and 9. Higher scores on the horizontal dimension indicated more pleasant affect. Higher scores on the vertical dimension indicated greater arousal.
Measurement of social behaviour
Each form listed 12 social behaviours that could be classified according to the interpersonal circumplex model: affiliation on one axis is defined by agreeable and quarrelsome behaviours, and power or status on the other axis is defined by dominant and submissive behaviours.45–48 Each form included 3 items of each dimension of behaviour, such as “I exchanged pleasantries” and “I gave information” for agreeableness, “I showed impatience” and “I criticized the other(s)” for quarrelsomeness, “I expressed an opinion” and “I assigned someone to a task” for dominance, and “I gave in” and “I spoke softly” for submissiveness. Participants were asked to check off all behaviours they engaged in during a social interaction. To prevent them from marking the same behaviours for every interaction, the list of behaviours on each form varied in a daily rotation of 4 forms. All behaviours were taken from a list of 46, which has been shown to provide valid and reliable scores of each dimension of social behaviour.42,47,49,50
The steps required for construction of event-level scale scores for agreeable, quarrelsome, dominant and submissive behaviours were the following: (1) calculation of a score for each scale by computing the mean frequency of behaviours corresponding to the scale, and (2) construction of ipsatized scores by subtracting mean frequency for all behaviours from each scale score. These ipsatized scores thus reflect the frequency with which agreeable, quarrelsome, dominant and submissive behaviours were marked, adjusted for the general rate of behaviour marking (in other words, scaling effects have been removed). Given that people usually mark quarrelsome and submissive behaviours less often, ipsatized scores for quarrelsome and submissive behaviours are on average lower than those for dominant and agreeable behaviours, and are frequently negative.
Measurement of social perception
Each form also included an 11 × 11 interpersonal grid.51 By placing a single mark, participants indicated to what extent they perceived their social interaction partner as quarrelsome versus agreeable, and dominant versus submissive. When in a group, participants only rated the behaviour of the person with whom they primarily interacted. When a primary interaction partner could not be identified, participants were instructed to leave the grid blank (this was the case for 11% of all interactions recorded).
For each event, scores on the 2 dimensions of the interpersonal grid were coded using a number between 1 and 11. Higher scores on the horizontal dimension indicated greater perceived dominance. Higher scores on the vertical dimension indicated greater perceived agreeableness.
Study overview
A significant social interaction was defined as lasting at least 5 minutes and involving a spoken conversation between at least 2 people. Participants were asked to complete a record form as soon as a social interaction ended, using a maximum of 10 record forms a day. The completion of record forms was dispersed throughout the day. All participants received packages containing tryptophan or placebo tablets, record forms and pre-addressed, stamped envelopes for each day's forms. On each day, they also recorded the time they took each tablet, and women were asked to indicate if they were menstruating. Participants received the materials for the first study phase at the end of the screening procedure, and they received another set of materials for the second study phase during a meeting in the laboratory in between the 2 phases. BDI scores were obtained during screening and after each study phase. At the end of the study, participants were asked during which phase they thought they were taking tryptophan.
Data analysis
Data were analyzed after the exclusion of all events sampled within 1 hour of alcohol ingestion (7.0% of over 7000 events). The number of such interactions that took place during tryptophan treatment was not significantly different from the number that took place when participants received placebo.
In the primary analyses, treatment (tryptophan, placebo) was considered a within-subjects factor. Period, a second within-subjects factor, divided each phase into 5 periods of 3 days. Treatment order (tryptophan first, placebo first) and gender (men, women) were the between-subjects factors. Main effects were entered first, followed by their 2-way and 3-way interactions. All statistical analyses were performed twice. First, analogous to our previous study, the first 3 days of each treatment phase were excluded, and only the data from the final 12 days of each treatment phase were used (periods 2–5). Second, all analyses were repeated with all 15 days included (periods 1–5). The results did not change, but in order to maintain consistency with our previous study only the former analyses are presented below.
Based on the outcome of F tests and t tests, effect-size calculations were performed for each significant effect of tryptophan.52 The formula r2 = t2/(t2 + df) was used, where r is the effect-size correlation, t is the square root of the F test (F = t2) in the case of a main effect or the value of the post hoc t test in the case of an interaction effect, and df is the number of denominator degrees of freedom in the F test or t test. Cohen's d values were calculated from effect-size correlations using r2 = d2/(d2 + 4).
To examine how much of the behavioural and perceptual changes could be explained by the observed changes in affect valence, secondary covariate analyses were also performed. The analyses for the 4 social behaviour variables and the 2 social perception variables were repeated using 3 main effects (treatment, treatment order, gender) and their interactions, with affect valence added as a covariate.
The number of record forms varied per day, per period and per person, thus resulting in different numbers of observations between as well as within individuals. Therefore, we used mixed linear modelling with maximum likelihood estimation (PROC MIXED in SAS 8.2). Treatment differences were calculated for the principal outcome measures with statistical significance set at p < 0.05. Tukey corrections were used for multiple comparisons in post hoc tests. Estimated least squares means and standard errors of the mean (SEM) are given for significant treatment differences.
Results
At the end of the study, participants were asked when they thought they were taking tryptophan. Of the men, 60% guessed correctly. Of the women, 63% did. This was not significantly different from chance, even when treatment order was taken into account.
Effects of tryptophan on affect
For affect arousal and affect valence, positive and negative affect, and the composite affect score, analyses were conducted with 4 main effects (treatment, order, gender, period) and their 2-way and 3-way interactions.
Affect arousal
The treatment × order × gender interaction was significant (F1,35 = 5.41, p = 0.026), but none of the post hoc tests were. No other effects were found.
Affect valence
There was a significant period effect (F3,114 = 7.68, p < 0.001): affect valence was significantly lower in period 3 than in periods 4 (t114 = –4.20, p < 0.001) and 5 (t114 = –3.97, p < 0.001). There was a significant treatment effect (F1,38 = 5.38, p = 0.026) and a significant treatment × order interaction (F1,36 = 16.81, p < 0.001). Tryptophan increased the pleasantness of affect in those participants who received tryptophan second (placebo v. tryptophan: 5.75 [SEM 0.14] v. 6.16 [SEM 0.14], t36 = –4.55, p < 0.001), but not in those who received tryptophan first (placebo v. tryptophan: 5.98 [SEM 0.14] v. 5.89 [SEM 0.14], t36 = 1.15, p = 0.26; Fig. 1). Cohen's d for affect valence in those who took tryptophan second was 1.5 (based on an r of 0.60), which is indicative of a large treatment effect.
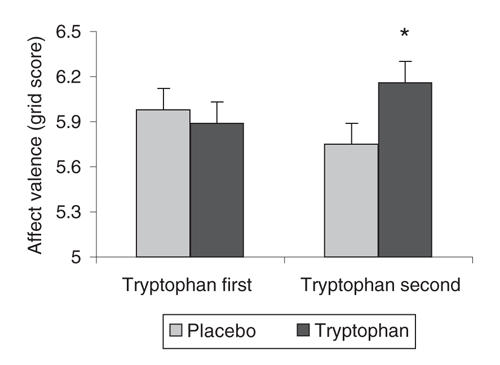
Fig. 1: Affect valence during tryptophan and placebo phases of treatment (values are estimated least squares means and standard errors). The horizontal axis crosses the vertical axis at 5 to indicate the middle of the individual axes on the affect grid. Tryptophan increased the pleasantness of affect in participants who received tryptophan second (*p < 0.001).
Positive and negative affect and the composite affect score
The analyses for the positive and negative affect variables and for the composite affect measure showed results that were very similar to those for affect valence. Thus, for positive affect, there was a treatment effect (F1,38 = 21.29, p < 0.001) and a treatment × order interaction (F1,36 = 7.35, p = 0.010), as well as an effect of period (F3,114 = 9.88, p < 0.001). Positive affect was lower on placebo than on tryptophan when tryptophan was given second (t36 = –5.12, p < 0.001) but not when tryptophan was given first (t36 = –1.46, p = 0.47), and it was lower in period 3 than in periods 2 (t114 = 3.09, p = 0.013), 4 (t114 = –5.10, p < 0.001) and 5 (t114 = –4.10, p < 0.001). There was also a significant tryptophan × order × period interaction (F3,108 = 2.80, p = 0.044) that showed no significant treatment differences post hoc.
For negative affect, there was again a treatment effect (F1,38 = 8.55, p = 0.006) and a treatment × order interaction (F1,36 = 21.36, p < 0.001), and an effect of period (F3,114 = 7.24, p < 0.001). An additional tryptophan × order × period interaction (F3,108 = 4.80, p = 0.004) showed that the negative affect–lowering effect of tryptophan in those who received tryptophan second was significant only in period 3 (t108 = 3.80, p = 0.021).
For the composite affect score, the main effect of treatment (F1,38 = 18.05, p < 0.001), the treatment × order interaction (F1,36 = 15.25, p < 0.001), the main effect of period (F3,114 = 9.98, p < 0.001) and the tryptophan × order × period interaction (F3,108 = 4.32, p = 0.006) were again all significant. Tryptophan improved affect in those who received tryptophan second exclusively in periods 3 (t108 = –3.83, p = 0.019) and 4 (t108 = –3.60, p = 0.039).
Effects of tryptophan on behaviour
For each behavioural variable, the analyses were first conducted with 4 main effects (treatment, order, gender, period) and their 2-way and 3-way interactions. Second, given the finding that tryptophan improved affect, covariate analyses were conducted for each variable, with 3 main effects (treatment, order, gender) and their 2-way and 3-way interactions, and affect valence as a covariate.
Quarrelsome behaviour
In the primary analyses, there was a significant main effect of treatment (F1,38 = 5.22, p = 0.028), and no interaction with gender or with treatment order. Tryptophan decreased quarrelsome behaviours (placebo v. tryptophan: –11.0 [SEM 0.92] v. –12.3 [SEM 0.93]; Fig. 2a). The r for quarrelsomeness was 0.35, thus yielding a Cohen's d value of 0.74 (medium effect size).
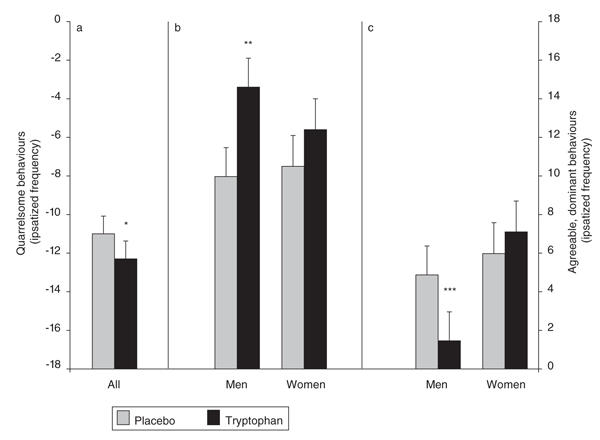
Fig. 2: Daily ipsatized frequencies of (a) quarrelsome, (b) agreeable and (c) dominant behaviours during tryptophan and placebo phases of treatment (values are estimated least squares means and standard errors). A description of the ipsatizing procedure can be found in the Methods section. Tryptophan decreased quarrelsomeness (*p = 0.028). In men, tryptophan also increased agreeableness (**p < 0.001) and decreased dominance (***p = 0.002).
In the secondary (covariate) analyses, more positive affect during social interactions was associated with lower levels of quarrelsomeness (F1,5143 = 813.42, p < 0.001). The effect of tryptophan was no longer significant when affect valence was controlled for (F1,35 = 1.68, p = 0.20).
Agreeable behaviour
Both the main effect of treatment (F1,38 = 23.43, p < 0.001) and the treatment × gender interaction (F1,35 = 4.28, p = 0.046) were significant in the primary analyses. Tryptophan increased agreeableness in both men (placebo v. tryptophan: 9.97 [SEM 1.5] v. 14.6 [SEM 1.5]) and women (placebo v. tryptophan: 10.5 [SEM 1.6] v. 12.4 [SEM 1.6]), although the effect was only significant in the men (t35 = –4.97, p < 0.001 for men; t35 = –1.99, p= 0.21 for women; Fig. 2b). The treatment effect size for men was large, based on an r value of 0.64 and a Cohen's d of 1.7.
In the secondary analyses, more positive affect was associated with higher levels of agreeableness (F1,5143 = 933.05, p < 0.001). Whereas the tryptophan × gender interaction was no longer significant (F1,35 = 3.36, p = 0.08), a significant main effect of tryptophan remained (F1,35 = 15.29, p < 0.001). When affect valence was controlled for statistically, levels of agreeable behaviours were higher on tryptophan (13.0 [SEM 1.1]) than on placebo (10.6 [SEM 1.1]) across genders.
Dominant behaviour
The primary analysis revealed a treatment × gender effect (F1,36 = 13.62, p < 0.001; Fig. 2c). Tryptophan decreased dominance in the men (placebo v. tryptophan: 4.87 [SEM 1.5] v. 1.46 [SEM 1.5], t36 = 3.96, p = 0.002), but there was no significant change in the women (placebo v. tryptophan: 5.98 [SEM 1.6] v. 7.10 [SEM 1.6], t36 = –1.27, p = 0.58). The treatment effect size for men was large (r = 0.56, Cohen's d = 1.3).
In the secondary analyses, more positive affect was associated with lower levels of dominance (F1,5143 = 5.60, p = 0.018). The tryptophan × gender interaction was maintained when controlling for affect valence (F1,35 = 12.58, p = 0.001), and no other effects were found.
Submissive behaviour
Neither the primary nor the secondary analysis revealed any significant effects.
Effects of tryptophan on perceptions of others
Primary and secondary analyses were identical to those conducted for the behavioural variables.
Perceptions of agreeableness
In the primary analysis, there was a significant period effect (F3,114 = 4.95, p = 0.003): as was the case for affect valence, perceptions of agreeableness were significantly lower in period 3 than in periods 4 (t114 = –2.97, p = 0.019) and 5 (t114 = –3.17, p = 0.010). Both the treatment × order interaction (F1,36 = 8.32, p = 0.007) and the treatment × order × gender interaction (F1,35 = 4.76, p = 0.036; Fig. 3a) were also significant. Post hoc testing of the 3-way interaction indicated that only men who received tryptophan in the second half of the study perceived their interaction partners as more agreeable when on tryptophan (placebo v. tryptophan: 7.69 [SEM 0.32] v. 8.23 [SEM 0.32], t35 = –3.61, p = 0.019). There was no such effect in men who received tryptophan first (placebo v. tryptophan: 7.79 [SEM 0.32] v. 7.58 [SEM 0.32], t35 = 1.45, p = 0.83) or in women, whether they received tryptophan first (placebo v. tryptophan: 7.69 [SEM 0.32] v. 7.60 [SEM 0.33], t35 = 0.60, p > 0.99) or second (7.81 [SEM 0.34] v. 7.81 [SEM 0.34], t35 = –0.05, p > 0.99). Based on an r value of 0.52 and a Cohen's d of 1.2, the treatment effect size for perceptions of agreeableness in men who received tryptophan second was again large.
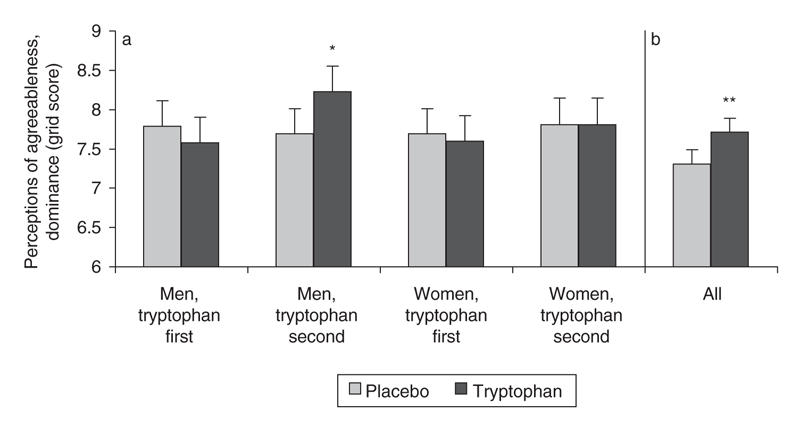
Fig. 3: Perceptions of (a) agreeableness and (b) dominance during tryptophan and placebo phases of treatment (values are estimated least squares means and standard errors). The horizontal axis crosses the vertical axis at 6 to indicate the middle of the individual axes on the interpersonal grid. Tryptophan increased perceived agreeableness in others in men who received tryptophan second (*p = 0.019). Tryptophan also increased perceived dominance in others (**p < 0.001).
In the secondary analysis, more positive affect was associated with higher perceived agreeableness in others (F1,4582 = 3190.90, p < 0.001). Whereas the tryptophan × gender × order interaction was again significant (F1,35 = 4.50, p = 0.041), none of the post hoc contrasts were.
Perceptions of dominance
The primary analysis revealed a main effect for treatment (F1,38= 53.16, p < 0.001). Compared with placebo, participants on tryptophan perceived others as more dominant (placebo v. tryptophan: 7.31 (SEM 0.18) v. 7.77 (SEM 0.18); Fig. 3b). The treatment effect size was large (r value = 0.76, Cohen's d = 2.4).
In the secondary analysis, more positive affect was associated with higher perceived dominance in others (F1,4577 = 89.31, p < 0.001), and the tryptophan effect was maintained (F1,35 = 45.64, p < 0.001).
Influence of menstrual cycle
The results did not change when women's premenstrual days were excluded (data not shown).
Discussion
Tryptophan treatment significantly decreased quarrelsome behaviours in all participants. Agreeable behaviours were increased and dominant behaviours decreased in the men. When affect valence was controlled for statistically, tryptophan increased agreeable behaviours in both men and women. Others were perceived as more agreeable by the men, and as more dominant by all. Affect was significantly improved in participants who received tryptophan second and moderated the effects of tryptophan on quarrelsomeness (but none of tryptophan's other effects). Overall, the primary analyses were indicative of medium-to-large treatment effect sizes.
This is the second study to show that tryptophan supplementation may not only reduce aggressive behaviours in experimental laboratory situations8,11 but also decrease quarrelsome behaviours in daily life.24 More important, this is the first study to show that tryptophan can also enhance agreeable behaviours in everyday social interactions. Given that participants in the present study, unlike those in our previous study,24 were selected on the basis of being highly quarrelsome, it is suggested that the extent to which tryptophan may enhance social affiliation depends on who is taking it. Similar to the notion that antidepressants elevate mood in depressed patients but not in euthymic people, and that serotonergic manipulations affect laboratory-measured aggression mostly in aggressive people,29–31 tryptophan may increase everyday agreeableness only in quarrelsome people. In addition, although this is not a direct comparison because the data were obtained from different studies, the treatment effect size for quarrelsomeness in the present study was greater than that in our previous study of unselected people (0.74 this study v. 0.54 previous study).24
This shift toward more socially constructive behaviours may be especially important for quarrelsome individuals. Participants in the present study (n = 39), who initially reported high levels of anger, hostility and irritability on selection measures, were indeed more quarrelsome and less agreeable than participants in our previous study (n = 98; overall mean level of quarrelsomeness during the placebo phase: –10.6 [standard deviation {SD} 6.5] this study v. –15.1 [SD 7.4] previous study, t135 = –3.39, p < 0.001; overall mean level of agreeableness during the placebo phase: 10.0 [SD 7.8] this study v. 13.9 [SD 6.4] previous study, t135 = 3.03, p = 0.003).24 Quarrelsome people are considered at risk for a variety of mental as well as physical illnesses.25–28 An increase in serotonin function that lowers quarrelsomeness and enhances agreeableness may improve social relationships and augment the benefits derived from such relationships that contribute to health.
The apparent ability of serotonin to promote positive social behaviours is also of interest, because the serotonin system has traditionally been thought of as an impulse-control system, inhibiting a wide range of behaviours that may be disadvantageous to an individual's survival.53,54 Yet the present study shows that serotonin not only inhibits negative behaviours but may also stimulate certain behaviours thought to be beneficial to social functioning and health. There have been a few laboratory studies in healthy volunteers showing similar effects of treatment with selective serotonin reuptake inhibitors on a measure of social affiliation: both Knutson et al22 and Tse and Bond23 observed an increase in cooperative behaviours measured during an experimental task involving dyadic interaction. The present study thus adds to a small body of evidence indicating that an increase in serotonin function may result not only in behavioural inhibition but also in facilitation of positive behaviours in response to social stimuli.
In line with the idea that a positive shift in quarrelsomeness–agreeableness may enhance personal well-being, tryptophan also improved affect during social interactions: participants reported more positive and fewer negative emotions when taking tryptophan and rated their interactions as more pleasant. The data from our previous study suggest that a change in mood is not necessary for a change in quarrelsomeness–agreeableness to occur.24 In the present study, the covariate analyses indicated that the effect of tryptophan on quarrelsomeness could be accounted for by a person's level of affect valence during social interactions. This suggests that tryptophan decreased aspects of affect valence such as irritability along with quarrelsome behaviour, which is what would be expected. The decline in quarrelsomeness may be the result in whole or in part of improved affect or, alternatively, an increase in serotonin may have a direct effect on both the mood and the behaviour. In contrast, the main effect of tryptophan on agreeableness remained significant even after affect valence had been added as a covariate, which suggests that tryptophan enhanced agreeable behaviours independent of its effects on mood. Thus, affect valence alone could not account for the observed changes in agreeable behaviour. It seems plausible that the improvement in mood was at least partially initiated when participants' behaviours during social interactions became more pro-social, which may have lead to reciprocated agreeable behaviour from others.
In our previous study, tryptophan decreased quarrelsomeness only when tryptophan was given second, that is, when the tryptophan phase followed the placebo phase.24 We hypothesized that the explanation for this carryover effect was less likely to be pharmacological (tryptophan is metabolized within 8 hours)55 than psychological: when tryptophan was given first, it may have altered the tone of interactions, which then persisted during the subsequent placebo phase. In the present study, tryptophan decreased quarrelsomeness whether it was given first or second. This could be due either to the longer washout period in this study or to the higher placebo levels of quarrelsomeness for this group.
An important addition to the present study was the assessment of perceptions of others' behaviours using the interpersonal grid.51 There was an interaction between treatment and order and gender for perceptions of agreeableness. Only male participants who received tryptophan second perceived their interaction partners as more agreeable when on tryptophan. The fact that the effect of tryptophan on perceptions of agreeableness was limited to men is consistent with its effect on behaviour. The treatment × order interaction suggests that male participants may have required the contrast of attending to others' agreeableness during placebo to observe the change in others that occurred during subsequent tryptophan treatment. In future treatment studies, this issue could be addressed using an initial placebo-only run-in phase. However, it may also be an indication of a carryover effect similar to that observed for quarrelsomeness in the previous study. Although a visual inspection of the raw data revealed no apparent linear trend over time, as may have been expected if the effects of tryptophan on one day were carried over into the next, time-related treatment effects are likely to have been confounded by the day of the week.42,56 Whereas weekly cyclicity may have dampened linear trends over time, the present finding on perceptions of agreeableness at least suggests that some effects of tryptophan may persist for days beyond its last administration, possibly because there is a change in both participants and their interaction partners. If this is so, then the order effect should be abolished by increasing the length of time of the washout period between treatments. Further research is also necessary to examine whether the behavioural changes followed or led the perceptual changes. For example, future study designs could include pairs of frequently interacting participants who would rate both their own and the other's behaviour, while only one of each pair would undergo double-blind placebo-controlled treatment.
In the men, tryptophan also decreased dominance, without increasing submissiveness. Separate influences on dominance and submissiveness have also been found in other domains, such as situational influences.50 According to the interpersonal circumplex model, the dominant–submissive and quarrelsome–agreeable axes are independent so, for example, individuals can act either in an agreeable–dominant or in an agreeable–submissive way.45–48 Within the interpersonal circumplex, tryptophan treatment in the men thus induced a shift away from quarrelsome–dominance toward agreeable–submissiveness. Whereas an agreeable–dominant behavioural pattern is generally considered socially constructive, behaving in a more agreeable–submissive manner can also be adaptive, especially in those who exhibit a high degree of quarrelsomeness. The male participants in the present study (n = 20) were less dominant compared with those in the previous study (n = 51; overall means during the placebo phase: 3.93 [SD 7.2] this study v. 8.88 [SD 6.1] previous study, t69 = 2.92, p = 0.005). On placebo, they were also quarrelsome and disagreeable, which in combination with low dominance may be perceived as being socially withdrawn.51 A tryptophan-induced move toward agreeable low dominance may be perceived as politely deferring to others and may promote opportunities for social bonding. It remains unclear why tryptophan did not change dominance in the women (n = 19), but their levels of dominant behaviours were not unusually low compared with the previous study (n = 47) as was the case for the men (overall means during the placebo phase: 5.64 [SD 7.3] this study v. 7.02 [SD 6.6] previous study, t64 = 0.74, p = 0.46).
Tryptophan increased ratings of dominant behaviour in others in all participants, yet only the men responded with reduced dominance. Perceptions of dominance may have increased when participants were taking tryptophan, because they were taking more notice of how other people behaved toward them. Further, there is some evidence that interactions with dominant others that result in less dominance may increase liking of the other more than similar interactions that result in more dominance.57 The decline in dominance observed in the men may thus have contributed to their enhanced social affiliation. Whatever the mechanism, further research into the role of serotonin in perceptions of others and their influence on the flow of social interactions is warranted, for example, given that distorted social perceptions are common in mental disorders such as depression and social phobia.58–60
In conclusion, this study has shown that an increase in brain serotonin, induced pharmacologically by means of oral tryptophan supplementation, can lead not only to a decrease in quarrelsome behaviours but also, in individuals with elevated trait levels of quarrelsomeness, to an increase in agreeable behaviours. Changes in dominance may also vary with the characteristics of those taking tryptophan. Further, as the present study has shown that tryptophan can change perceptions of others, it is important to consider the dynamic quality of human social interactions in understanding how serotonin influences behaviour. The observed improvement in affect was associated with the decrease in quarrelsomeness but not with any of the other behavioural and perceptual changes. Overall, tryptophan had a positive effect on social interactions in everyday life. Given that participants initially reported problems during their social interactions, and given the importance of good social functioning for well-being and health, the improvement in both social behaviour and mood is noteworthy.
Acknowledgments
We thank ICN Canada (now Valeant Canada), which markets tryptophan (Tryptan) as a prescription drug in Canada, for providing the tablets of tryptophan and placebo free of charge.
Footnotes
Contributors: Ms. aan het Rot and Drs. Moskowitz and Young conceived of the study and analyzed the data. Ms. aan het Rot and Dr. Pinard acquired the data. Ms. aan het Rot and Dr. Moskowitz wrote the article. All authors critically reviewed the article and gave final approval for publication.
This research was supported by a grant from the Canadian Institutes of Health Research to Dr. Young (MOP 15005). Ms. aan het Rot was the recipient of a McGill University Health Centre Studentship.
Competing interests: None declared for Ms. aan het Rot and Drs. Moskowitz and Pinard. ICN Canada (now Valeant Canada) provided Dr. Young with the tryptophan (Tryptan) and placebo tablets without charge.
Correspondence to: Ms. Marije aan het Rot, Department of Psychiatry, McGill University, 1033 Pine Ave. W, Montréal QC H3A 1A1; fax 514 398-4370; marije.aanhetrot@mail.mcgill.ca
References
- 1.Brown GL, Ebert MH, Goyer PF, et al. Aggression, suicide, and serotonin: relationships to CSF amine metabolites. Am J Psychiatry 1982;139:741-6. [DOI] [PubMed]
- 2.Cleare AJ, Bond AJ. Does central serotonergic function correlate inversely with aggression? A study using D-fenfluramine in healthy subjects. Psychiatry Res 1997;69:89-95. [DOI] [PubMed]
- 3.Higley JD, King ST, Hasert MF, et al. Stability of interindividual differences in serotonin function and its relationship to severe aggression and competent social behavior in rhesus macaque females. Neuropsychopharmacology 1996;14:67-76. [DOI] [PubMed]
- 4.Higley JD, Mehlman PT, Poland RE, et al. CSF testosterone and 5-HIAA correlate with different types of aggressive behaviors. Biol Psychiatry 1996;40:1067-82. [DOI] [PubMed]
- 5.Mehlman P, Higley J, Faucher I, et al. Low CSF 5-HIAA concentrations and severe aggression and impaired impulse control in nonhuman primates. Am J Psychiatry 1994;151:1485-91. [DOI] [PubMed]
- 6.Higley JD, Mehlman PT, Higley SB, et al. Excessive mortality in young free-ranging male nonhuman primates with low cerebrospinal fluid 5-hydroxyindoleacetic acid concentrations. Arch Gen Psychiatry 1996;53:537-43. [DOI] [PubMed]
- 7.Westergaard GC, Cleveland A, Trenkle MK, et al. CSF 5-HIAA concentration as an early screening tool for predicting significant life history outcomes in female specific-pathogen-free (SPF) rhesus macaques (Macaca mulatta) maintained in captive breeding groups. J Med Primatol 2003;32:95-104. [DOI] [PubMed]
- 8.Bond AJ, Wingrove J, Critchlow DG. Tryptophan depletion increases aggression in women during the premenstrual phase. Psychopharmacology (Berl) 2001;156:477-80. [DOI] [PubMed]
- 9.Chamberlain B, Ervin FR, Pihl RO, et al. The effect of raising or lowering tryptophan levels on aggression in vervet monkeys. Pharmacol Biochem Behav 1987;28:503-10. [DOI] [PubMed]
- 10.Raleigh MJ, Brammer GL, Ritvo ER, et al. Effects of chronic fenfluramine on blood serotonin, cerebrospinal fluid metabolites, and behavior in monkeys. Psychopharmacology (Berl) 1986;90:503-8. [DOI] [PubMed]
- 11.Smith SE, Pihl RO, Young SN, et al. Elevation and reduction of plasma tryptophan and their effects on aggression and perceptual sensitivity in normal males. Aggress Behav 1987;12:393-407.
- 12.Coccaro EF, Kavoussi RJ. Fluoxetine and impulsive aggressive behavior in personality-disordered subjects. Arch Gen Psychiatry 1997;54:1081-8. [DOI] [PubMed]
- 13.Morand C, Young SN, Ervin FR. Clinical response of aggressive schizophrenics to oral tryptophan. Biol Psychiatry 1983;18:575-8. [PubMed]
- 14.Huber R, Smith K, Delago A, et al. Serotonin and aggressive motivation in crustaceans: altering the decision to retreat. Proc Natl Acad Sci U S A 1997;94:5939-42. [DOI] [PMC free article] [PubMed]
- 15.Kostowski W, Tarchalska B. The effects of some drugs affecting brain 5-HT on the aggressive behaviour and spontaneous electrical activity of the central nervous system of the ant, Formica rufa. Brain Res 1972;38:143-9. [DOI] [PubMed]
- 16.Livingstone MS, Harris-Warrick RM, Kravitz EA. Serotonin and octopamine produce opposite postures in lobsters. Science 1980;208:76-9. [DOI] [PubMed]
- 17.Yodyingyuad U, De la Riva C, Abbott DH, et al. Relationship between dominance hierarchy, cerebrospinal fluid levels of amine transmitter metabolites (5-hydroxyindole acetic acid and homovanillic acid) and plasma cortisol in monkeys. Neuroscience 1985;16:851-8. [DOI] [PubMed]
- 18.Raleigh MJ, McGuire MT, Brammer GL, et al. Serotonergic mechanisms promote dominance acquisition in adult male vervet monkeys. Brain Res 1991;559:181-90. [DOI] [PubMed]
- 19.Mehlman PT, Higley JD, Faucher I, et al. Correlation of CSF 5-HIAA concentration with sociality and the timing of emigration in free-ranging primates. Am J Psychiatry 1995;152:907-13. [DOI] [PubMed]
- 20.Raleigh MJ, McGuire MT. Animal analogues of ostracism: biological mechanisms and social consequences. Ethol Sociobiol 1986;7:53-66.
- 21.Raleigh MJ, McGuire MT, Brammer GL, et al. Social and environmental influences on blood serotonin concentrations in monkeys. Arch Gen Psychiatry 1984;41:405-10. [DOI] [PubMed]
- 22.Knutson B, Wolkowitz OM, Cole SW, et al. Selective alteration of personality and social behavior by serotonergic intervention. Am J Psychiatry 1998;155:373-9. [DOI] [PubMed]
- 23.Tse WS, Bond AJ. Serotonergic intervention affects both social dominance and affiliative behaviour. Psychopharmacology (Berl) 2002;161:324-30. [DOI] [PubMed]
- 24.Moskowitz DS, Pinard G, Zuroff DC, et al. The effect of tryptophan on social interaction in everyday life: a placebo-controlled study. Neuropsychopharmacology 2001;25:277-89. [DOI] [PubMed]
- 25.Conner KR, Duberstein PR, Conwell Y, et al. Reactive aggression and suicide: theory and evidence. Aggress Violent Behav 2003;8:413-32.
- 26.Troisi A, Moles A. Gender differences in depression: an ethological study of nonverbal behavior during interviews. J Psychiatr Res 1999; 33:243-50. [DOI] [PubMed]
- 27.Williams JE, Paton CC, Siegler IC, et al. Anger proneness predicts coronary heart disease risk: prospective analysis from the atherosclerosis risk in communities (ARIC) study. Circulation 2000;101: 2034-9. [DOI] [PubMed]
- 28.Yan LL, Liu K, Matthews KA, et al. Psychosocial factors and risk of hypertension: the Coronary Artery Risk Development in Young Adults (CARDIA) study. JAMA 2003;290:2138-48. [DOI] [PubMed]
- 29.Bjork JM, Dougherty DM, Moeller FG, et al. Differential behavioral effects of plasma tryptophan depletion and loading in aggressive and nonaggressive men. Neuropsychopharmacology 2000;22:357-69. [DOI] [PubMed]
- 30.Cleare AJ, Bond AJ. The effect of tryptophan depletion and enhancement on subjective and behavioural aggression in normal male subjects. Psychopharmacology (Berl) 1995;118:72-81. [DOI] [PubMed]
- 31.Finn PR, Young SN, Pihl RO, et al. The effects of acute plasma tryptophan manipulation on hostile mood: the influence of trait hostility. Aggress Behav 1998;24:173-85.
- 32.Beck AT, Rush A, Shaw B, et al. Cognitive therapy of depression. New York: Guilford Press; 1979.
- 33.Selzer ML, Vinokur A, Van Rooijen L. A self-administered Short Michigan Alcoholism Screening Test (SMAST). J Stud Alcohol 1975;36:117-26. [DOI] [PubMed]
- 34.Buss AH, Durkee A. An inventory for assessing different kinds of hostility. J Consult Psychol 1957;21:343-9. [DOI] [PubMed]
- 35.Costa PT, McCrae RR. Revised NEO Personality Inventory (NEO-PI-R) and NEO Five-Factor Inventory (NEO-FFI): professional manual. Odessa (FL): Psychological Assessment Resources; 1992.
- 36.Seroczynski AD, Bergeman CS, Coccaro EF. Etiology of the impulsivity/aggression relationship: Genes or environment? Psychiatry Res 1999;86:41-57. [DOI] [PubMed]
- 37.Barratt E. Impulsiveness subtraits: arousal and information processing. In: Spence JT, Izard CE, editors. Motivation, emotion and personality. Amsterdam: Elsevier Science Inc.; 1985. p. 137-46.
- 38.Young SN, Gauthier S. Effect of tryptophan administration on tryptophan, 5-hydroxyindoleacetic acid and indoleacetic acid in human lumbar and cisternal cerebrospinal fluid. J Neurol Neurosurg Psychiatry 1981;44:323-7. [DOI] [PMC free article] [PubMed]
- 39.Benedict CR, Anderson GH, Sole MJ. The influence of oral tyrosine and tryptophan feeding on plasma catecholamines in man. Am J Clin Nutr 1983;38:429-35. [DOI] [PubMed]
- 40.Young SN. The clinical psychopharmacology of tryptophan. In: Wurtman RJ, Wurtman JJ, editors. Nutrition and the brain. Vol 7. New York: Raven Press; 1986. p. 49-88.
- 41.Young SN, Leyton M. The role of serotonin in human mood and social interaction. Insight from altered tryptophan levels. Pharmacol Biochem Behav 2002;71:1-9. [DOI] [PubMed]
- 42.Brown KW, Moskowitz DS. Dynamic stability: the rhythms of our daily lives. J Pers 1998;66:105-34. [DOI] [PubMed]
- 43.Diener E, Emmons RA. The independence of positive and negative affect. J Pers Soc Psychol 1984;47:1105-17. [DOI] [PubMed]
- 44.Russell JA, Weiss A, Mendelsohn GA. Affect grid: single item scale of pleasure and arousal. J Pers Soc Psychol 1989;57:493-502.
- 45.Carson RC. Interaction concepts of personality. Chicago (IL): Aldine; 1969.
- 46.Leary T. Interpersonal diagnosis of personality. New York: Ronald Press; 1957.
- 47.Moskowitz DS. Cross-situational generality and the interpersonal circumplex. J Pers Soc Psychol 1995;66:921-33.
- 48.Wiggins JS, Broughton R. The interpersonal circle: a structural model for the integration of personality research. In: Hogan R, Jones W, editors. Perspectives in personality. Vol 1. Greenwich (CT): JAI Press; 1985. p. 1-47.
- 49.Moskowitz DS, Suh EJ, Desaulniers J. Situational influences on gender differences in agency and communion. J Pers Soc Psychol 1994;66:753-61. [DOI] [PubMed]
- 50.Moskowitz DS, Coté S. Do interpersonal traits predict affect? A comparison of three models. J Pers Soc Psychol 1995;69:915-24.
- 51.Moskowitz DS, Zuroff DC. Assessing interpersonal perceptions using the interpersonal grid. Psychol Assess 2005;17:218-30. [DOI] [PubMed]
- 52.Rosnow RL, Rosenthal R. Computing contrasts, effect sizes, and counternulls on other people's published data: general procedures for research consumers. Psychol Methods 1996;1:331-40.
- 53.Soubrié P. [Serotonergic neurons and behavior]. J Pharmacol 1986;17:107-12. [PubMed]
- 54.Spoont MR. Modulatory role of serotonin in neural information processing: implications for human psychopathology. Psychol Bull 1992;112:330-50. [DOI] [PubMed]
- 55.Yuwiler A, Brammer GL, Morley JE, et al. Short-term and repetitive administration of oral tryptophan in normal men. Effects on blood tryptophan, serotonin, and kynurenine concentrations. Arch Gen Psychiatry 1981;38:619-26. [DOI] [PubMed]
- 56.Moskowitz DS, Brown KW, Coté S. Reconceptualizing stability: using time as a psychological dimension. Curr Direct Psychol Sci 1997;6:127-32.
- 57.Tiedens LZ, Fragale AR. Power moves: complementarity in dominant and submissive nonverbal behavior. J Pers Soc Psychol 2003;84:558-68. [DOI] [PubMed]
- 58.Bouhuys AL, Geerts E, Gordijn MC. Depressed patients' perceptions of facial emotions in depressed and remitted states are associated with relapse: a longitudinal study. J Nerv Ment Dis 1999;187:595-602. [DOI] [PubMed]
- 59.Gara MA, Woolfolk RL, Cohen BD, et al. Perception of self and other in major depression. J Abnorm Psychol 1993;102:93-100. [DOI] [PubMed]
- 60.Rapee RM, Heimberg RG. A cognitive-behavioral model of anxiety in social phobia. Behav Res Ther 1997;35:741-56. [DOI] [PubMed]