

Abstract
Background
In 2002, Hockey Canada changed the age classifications for minor ice hockey. Previously, 10- and 11-year-old children played at the Atom level (no bodychecking), and 12- and 13-year-old children played at the Peewee level (bodychecking allowed). After the policy change, 11-year-old players were placed in the Peewee division with 12-year-old players; the Atom division included 9- and 10-year-old players. The objective of this study was to examine the effect that the policy change had on injuries to 11-year-old players and compare this information with injury trends among 10- and 12-year-old players.
Methods
The study location was the Capital Health region, which serves the greater Edmonton area in Alberta. Capital Health maintains a database of all emergency department visits in the region. A search of the database identified 10-, 11- and 12-year-old players admitted to 7 emergency departments with hockey-related injuries during the 2 years before and the 2 years after the policy change. We also conducted a chart review for the 11-year-old players, extracting detailed information on the nature and circumstances of their injuries for the same period.
Results
The rate of injuries sustained by 11-year-old children playing at the Peewee level (with bodychecking) increased significantly compared with the rate among 11-year-0ld players at the Atom level (rate ratio [RR] 1.9, 95% confidence interval [CI] 1.4–2.4). The rate of severe injuries was more than 2 times greater among 11-year-old Peewee players than among 11-year-old Atom players (RR 2.4, 95% CI 1.6–3.6). Injury rates among the 10-year-old players (bodychecking never allowed) and the 12-year-old players (bodychecking always allowed) changed little over the study period.
Interpretation
The introduction of bodychecking to 11-year-old players was associated with a large increase in injury rates. From a public health perspective, the age at which bodychecking is introduced in minor hockey should be raised.
Ice hockey is recognized as Canada's national sport, with over 500 000 youth registered each year in minor hockey.1 Unfortunately, hockey-related injuries are among the most common sustained by children during sport and recreational activities.2
Most injuries in minor hockey (50%–86%) are caused by bodychecking.3 Few studies have examined the effects of bodychecking in the younger (9–12 year) groups; those that have have reached conflicting conclusions.4–8
A policy change by Hockey Canada at the beginning of the 2002/03 hockey season moved 11-year-old players in Alberta from the Atom level (bodychecking not permitted) to the Peewee level (bodychecking permitted).9 The objective of this study was to examine changes in the profile and rates of injuries before and after the policy change among 11-year-old players and to compare these trends with trends among 10- and 12-year-old players.
Methods
The Capital Health region serves the greater Edmonton area in Alberta. At the time of the study, there were 7 emergency departments in the region. For all emergency department admissions, Capital Health maintains the Ambulatory Care Classification System (ACCS) database. Discharge abstracts are completed for each emergency department visit by trained medical record nosologists who enter demographic, diagnostic and procedural information using the International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM), before Apr. 1, 2002, and the International Classification of Diseases, Tenth Revision (ICD-10), after Apr. 1, 2002. The discharge abstract also includes an independent sport/recreation (SR) coding system that provides information on more than 120 SR-related injuries, including a code for hockey-related injuries (SR code 054).10
We searched the ACCS database for records of children aged 10, 11 and 12 years who were injured playing ice hockey during the season (September to April) in 2000/01 to 2003/04. Depending on their date of birth, 11-year-old children either played at the Atom level (no bodychecking allowed) before the Hockey Canada policy change came into effect or played at the Peewee level (bodychecking permitted) after the policy change came into effect. Ten-year-old children playing at the Atom level were never allowed to bodycheck, and 12-year-old children playing at the Peewee level were always allowed to bodycheck.
First we conducted a chart audit of the 11-year-old children with hockey-related injuries. We divided these players into 2 groups. The first group included those born between Jan. 1, 1989, and Dec. 31, 1990, who played at the Atom level (no bodychecking allowed) before the policy change came into effect and who presented to an emergency department with a hockey-related injury during the 2000/01 or 2001/02 season. The second group included 11-year-old children born between Jan. 1, 1991, and Dec. 31, 1992, who played at the Peewee level (bodychecking permitted) after the policy change and who presented to an emergency department during the 2002/03 or 2003/04 season.
Charts were excluded from the audit if the children did not reside in the Capital Health region at the time of injury, were not playing organized hockey, were playing a sport other than ice hockey (e.g., street or ball hockey, roller hockey) or visited the emergency department for follow-up (i.e., not the index visit for the injury), or if the reason for the emergency department admission was not injury related (i.e., a miscoded medical problem).
Charts that met the inclusion criteria were reviewed by 2 trained research assistants. A standardized form was used to collect demographic characteristics, details about the initial presentation to the emergency department, the anatomic location (e.g., head or face, neck) and nature (e.g., fracture, concussion) of the injury, severity, circumstances of the injury, symptoms, emergency department examination and investigations ordered, treatment provided in the emergency department and discharge status (admitted to hospital or discharged).
The injuries were classified into 3 categories: nonbody contact, body contact and unspecified. The nonbody-contact category included injuries due to pucks, sticks (including crosschecking), falls, running into the boards, and an “other” category. The body-contact category included injuries from being bodychecked (into the boards or not), injuries sustained while initiating bodychecks and injuries from unintentional body contact.
Severe injuries included concussion or other head injury, any bone fracture, neck sprain or strain, and injury requiring hospital admission or transfer to a different hospital. Injury location was classified as lower extremity, upper extremity, head or face (mouth, nose, ear, eye, head, face), neck (neck, cervical spine) and trunk (ribs, thorax, lumbar spine, spleen, abdomen).
We also conducted a trend analysis by deriving rates of hockey-related injuries using the ACCS data for hockey-related injuries among the 10-, 11- and 12-year-old players for the 2000/01 to 2003/04 hockey seasons. To determine the rates, we used 2 denominators: one based on the number of registered players and the other on population data for the Capigal Health region. The estimated number of registered 10-, 11- and 12-year-old players for each of the 4 hockey seasons was obtained from information from minor hockey associations in the greater Edmonton area. Player registration data were not available by age for all years; however, registration data were available by level of play (e.g., Atom, Peewee). To obtain the number of players at each level, we assumed an equal distribution of children in each 2-year age group. For example, for the first 2 seasons, we assumed that half of the Atom players were 10 years old and the other half were 11 years old. This assumption was reasonably based on Edmonton Minor Hockey Association data, which showed that 51.5% of Atom players were 11 years old in 2001/02 and 48.7% of Peewee players were 11 years old in 2002/03 (Doug Lemermeyer, Edmonton Minor Hockey Association, Edmonton, Alta.: Number of registrants in Edmonton Minor Hockey Association [unpublished data]; personal communication, 2005).
Total registrations from 1997/98 to 2004/05 in the Edmonton Minor Hockey Association were available, except for 2002/03. We imputed the 2002/03 numbers using linear regression. The regression equation for the Peewee age classification was 7.5942*x + 1423.3; “x” in this equation equaled 6 (i.e., 2002/03 was the sixth year of data in our array). Therefore, for 2002/03 we had an estimated 1378 registrants. This number was then added to the other hockey associations in the Capital Health region to derive a total for the region. We were unable to obtain any registration data from 3 smaller local regions (Sherwood Park, Strathcona County or Beaumont) over the study period, which would result in an overestimate of the injury rate based on registration numbers.
For the population-based denominator, we obtained data on the number of 10-, 11- and 12-year-old children in the Capital Health region over the same period from the Capital Health Population Health and Research Department.11 Because these data were available by calendar year only (and a single hockey season covers part of 2 calendar years), we used the 2001 age-specific population estimates for the years before the policy change and the 2003 estimates for the years after the policy change.
The rates of injury per 1000 registered 11-year-old hockey players and per 1000 11-year-old children in the general population were calculated for each of the non-bodychecking and bodychecking cohorts before and after the policy change. From these data, we calculated rate ratios (RRs) and 95% confidence intervals (CIs)12 for comparisons of all injuries, and by injury type, location, severity and cause, during the periods before and after the policy change. The trends in injury rates among the 10- and 12-year-old players before and after the policy change were also examined.
Since we imputed the number of registered players in the 2002/03 season, a sensitivity analysis was conducted to compare the results to the situation where the number of players increased or decreased enough to change the interpretation of our results. Numerators for the sensitivity analysis were based on the chart review data.
This study was approved by the Health Research Ethics Board (Panel B: Health Research) at the University of Alberta.
Results
Injuries among 11-year-old players
Initially, a total of 278 charts for 11-year-old players were identified from the ACCS database. Of these, 45 (16.2%) were excluded from further analysis (Fig. 1). There were no significant differences between the Atom (no bodychecking) and Peewee (bodychecking permitted) groups regarding the number or reasons for exclusion. Overall, 233 injured players were included in the chart review.
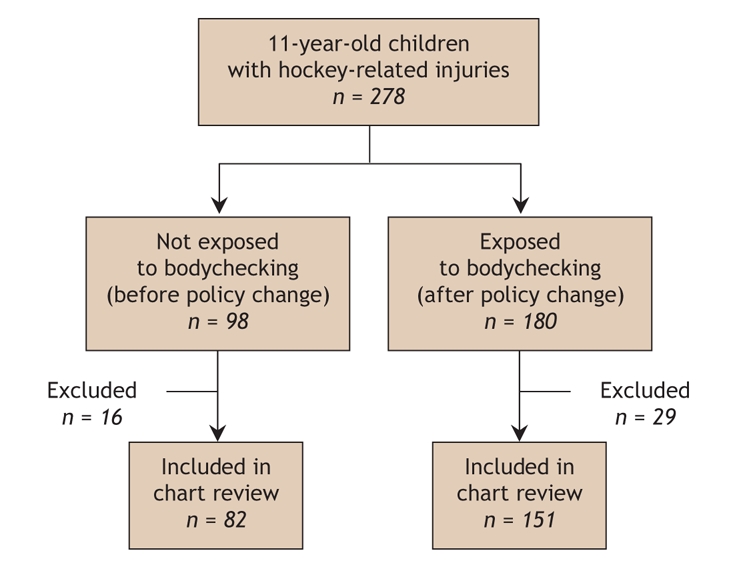
Fig. 1: Case identification of 11-year-old children with hockey-related injuries during the 2000/01 to 2003/04 hockey seasons in the Capital Health region of Alberta. (See Methods for reasons for exclusion.)
Most of the 11-year-old injured players were male (70 [85.4%] in the non-bodychecking group and 144 [95.4%] in the bodychecking group). Of the 233 patients, 14 had 2 distinct injuries that required separate treatments, and 1 had 3 distinct injuries, for a total of 249 injuries (90 sustained by those not exposed to bodychecking and 159 by those exposed to bodychecking).
The rate of injury based on player registration data was 40.6 per 1000 11-year-old players in the non-bodychecking group and 85.5 per 1000 11-year-old players in the bodychecking group, for a rate ratio of 2.1 (95% CI 1.6–2.8) (Table 1). Population figures produced a similar rate ratio (RR 1.9, 95% CI 1.4–2.4). Because the population figures provide a more conservative estimate (i.e., RRs are closer to 1.0), we present these in the remainder of the report. The population-based RR for males was 2.1 (95% CI 1.6–2.8) and for females, 0.6 (95% CI 0.2–1.5).
Table 1

There were 18 injuries (20.0%) to the head or face area among the 11-year-old players in the non-bodychecking group, compared with 38 such injuries (23.9%) in the bodychecking group (Table 2). The population-based RR for such injuries was 2.1 (95% CI 1.2–3.7) and for injuries to the neck area, 1.3 (95% CI 0.6–2.8).
Table 2
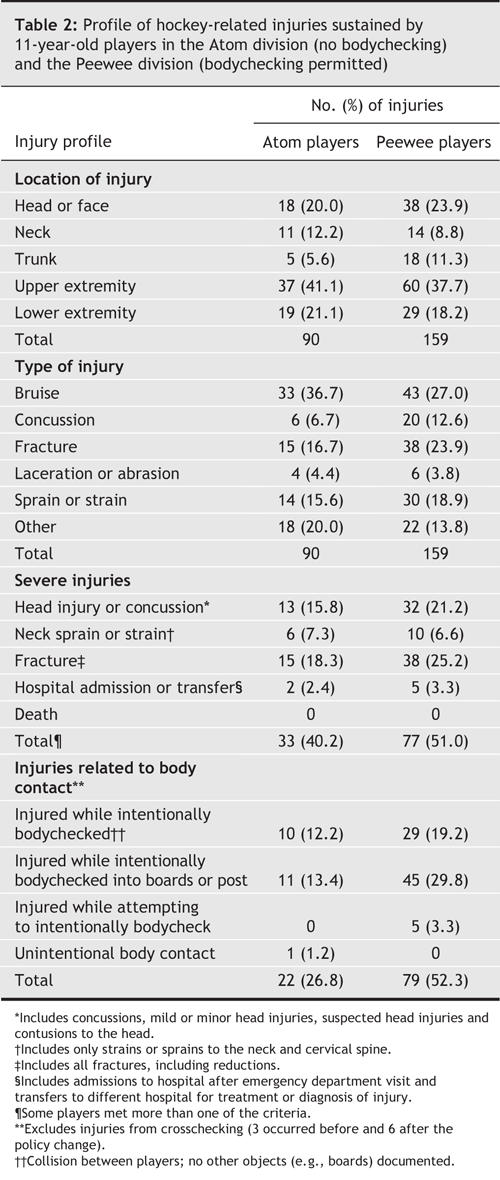
Concussions and fractures were significantly more common in the bodychecking group: the population-based RR for concussions was 3.4 (95% CI 1.4–8.4) and for fractures, 2.6 (95% CI 1.4–4.7).
Significantly more 11-year-old players in the bodychecking group than in the non-bodychecking group sustained injuries that were classified as severe (77 [51.0%] v. 33 [40.2%]; population-based RR 2.4, 95% CI 1.6–3.6) (Table 2).
Injuries from body contact occurred more frequently in the bodychecking group than in the non-bodychecking group (79 [52.3%] v. 22 [26.8%]; population-based RR 3.6, 95% CI 2.3–5.8). Nine injuries involving crosschecking were not included in the body-contact category; 3 occurred before and 6 after the policy change.
Changes in injury rates over time
During the 4-year study period, 945 hockey-related injuries were sustained by the 10-, 11- and 12-year-old players. Neither the 10- nor the 12-year-old players had significantly more hockey-related injuries after the policy change than before the change (population-based RR 0.8, 95% CI 0.6–1.2; and 1.0, 95% CI 0.8–1.2, respectively). However, among the 11-year-old players, significantly more injuries were sustained after the policy change (population-based RR 1.9, 95% CI 1.4–2.4). Population-based RRs by body region for the 3 age groups are presented in Fig. 2.
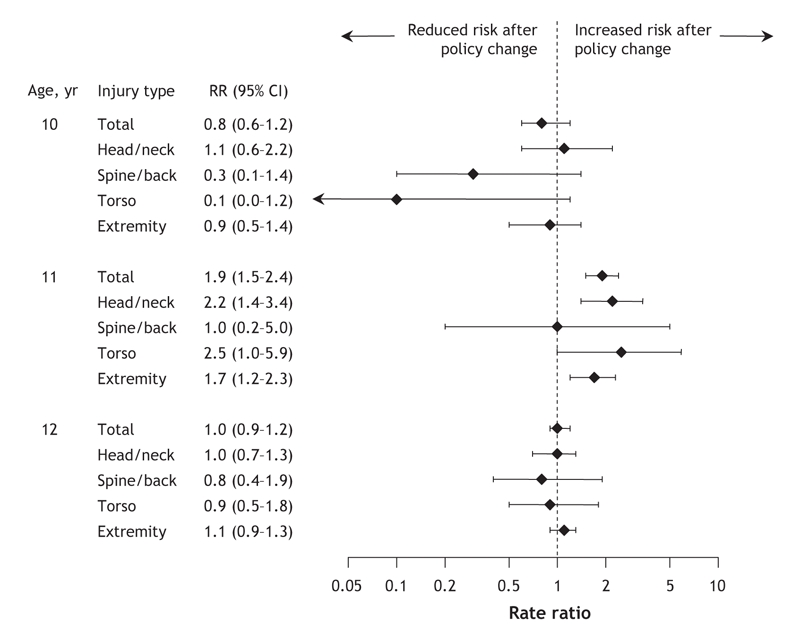
Fig. 2: Population-based rate ratios (RRs) for hockey-related injuries by body region among 10-, 11- and 12-year-old hockey players after policy change to move 11-year-old players from the Atom division (no bodychecking) to the Peewee division (bodychecking permitted). Error bars represent 95% confidence intervals (CIs).
Sensitivity analysis
The results of the sensitivity analysis demonstrate that an increase of more than 53% in the number of 11-year-old registered players in the Peewee division, or a decrease of 35% in the number of 11-year-old players in the Atom division, would be required to make the differences in the number of injuries nonsignificant.
Interpretation
We report the effect of a policy change that lowered the age of hockey players at the Peewee level (bodychecking permitted) from 12 to 11 years. Our results clearly show that 11-year-old players exposed to bodychecking after the policy change had an injury rate twice that of 11-year-old players not exposed to bodychecking before the policy change. The rate of severe injuries was more than 2 times greater among 11-year-old players exposed to bodychecking than among those not exposed to bodychecking. The rates of injury by body region in most cases increased significantly among 11-year-old players following the policy change, with no significant change in injury rates among the 10- and 12-year-old players over the study period.
The results of our study support previous research that compared bodychecking cohorts with nonbodychecking cohorts. Researchers compared injury rates among 28 bodychecking Peewee teams (12–13 years old) and 21 nonbodychecking Peewee teams in Quebec for one season.6,7 They found a 12-fold greater fracture rate in the bodychecking leagues. Macpherson and colleagues4 used data from the Canadian Hospitals Injury Reporting and Prevention Program (CHIRPP) to compare hockey-related injuries in Quebec (where bodychecking is implemented at the Bantam level) with those in Ontario (where bodychecking is implemented at the Atom level). The researchers found a higher proportion of head injuries and fractures in the bodychecking leagues compared with the non-bodychecking leagues among the Atom (10–11 years old), Peewee (12–13 years old) and Bantam (14–15 years old) players. Willer and colleagues8 examined hockey-related injury rates among players aged 4–18 years. In the Atom, Peewee and Bantam groups, the leagues that allowed bodychecking had greater rates of injury; however, the implications of these data have been debated.13 In a study involving 9- to 11-year-old hockey players in Ontario during the 1998/99 to 2000/01 hockey seasons, Montelpare and McPherson5 concluded that “the introduction of bodychecking at the Atom age level ... did not cause an increase in the number of claims for injuries to the CHA (Canadian Hockey Association) insurance group.” However, when using a denominator of estimated athlete exposures instead of players, the rate of injury was about 3 times higher in the bodychecking league than in the non-bodychecking league. Increases in the self-reported injury rate among those allowed to bodycheck were also evident.
Some argue that if 11-year-old players were taught to bodycheck properly, then the differences in injury rates would disappear. However, research conducted at the Bantam level (14- and 15-year-old players) has shown that teaching proper bodychecking technique has little influence on injury rates.14 Others might argue that if children were taught bodychecking at an early age, they would be less susceptible to contact-related injuries as they grow older. Yet Macpherson and colleagues4 observed a greater risk of checking-related injury among players aged 10–13 years in Ontario (bodychecking allowed at the Atom level) than in Quebec (bodychecking delayed until Bantam). The evidence suggests that significant harm, and no discernable health benefit, accompanies the introduction of bodychecking at a younger age.
No study is without limitations. Emergency physicians were not always comprehensive in their documentation, and some charts did not provide detailed injury information. We did not examine patient records from other health care providers, so the magnitude of injuries was underestimated. The number of registered players was only partially available for the study period and, where there were missing data, we used imputed values. We also have no way of knowing whether injured children were in a bodychecking or non-bodychecking league. Finally, before the policy change, 11-year-old children were the oldest players in the Atom division; after the change, 11-year-old children were the youngest players in the Peewee division, which may have affected the comparison before and after the policy change.
Our results indicate that the introduction of bodychecking increased the rate of injuries among 11-year-old hockey players. To reduce the number of injuries sustained in minor hockey, the age at which bodychecking is introduced should be raised. Based on the existing evidence, and the precautionary principle,15 this move would protect children from serious and potentially permanent injury.
@ See related article page 163
Acknowledgments
We thank Capital Health for funding this study, the Capital Health Medical Records Departments for their cooperation and Virginia Willis for assistance with chart data abstraction. We also acknowledge the in-kind contribution of the Alberta Centre for Injury Control and Research in providing infrastructure and project-related resources for Amy Couperthwaite and Joseph Sommerfeldt. Finally, we thank Sandra Blitz for her assistance with Fig. 2.
Footnotes
This article has been peer reviewed.
Contributors: Brent Hagel, Josh Marko, Donna Dryden and Brian Rowe contributed to the study conception and design and the acquisition of funding. Josh Marko, Amy Couperthwaite and Joseph Sommerfeldt contributed to the acquisition of the primary data. Brent Hagel, Donna Dryden, Amy Couperthwaite and Joseph Sommerfeldt contributed to the drafting of the article. All of the authors contributed to the analysis and interpretation of the data and revision of the article for important intellectual content and gave final approval for publication.
This work was part of the Children's Hockey Injury Prevention (CHIP) initiative; a partnership project with Capital Health. Members of the CHIP Committee include (in alphabetical order) Marie Carlson (Capital Health, Population Health), Charlene Davis (Past President, Edmonton Minor Hockey Association), Adele Dorey (KIDSAFE Connection, Injury Prevention Program of the Stollery Children's Hospital), Donna Dryden (Department of Pediatrics, University of Alberta), Brent Hagel (Departments of Paediatrics and Community Health Sciences, University of Calgary), Michael Henry (Abells Henry Consultants), Josh Marko (Capital Health, Population Health), Bob McKim (Capital Health, Primary Care Division), Brian Rowe (Department of Emergency Medicine, University of Alberta) and Kim Sanderson (Project Coordinator, Strategic Services, City of Edmonton). Brian Rowe is supported by the Canadian Institutes of Health Research as a Canada Research Chair. Brent Hagel holds the recently appointed position of Professorship in Child Health and Wellness funded by the Alberta Children's Hospital Foundation, through the generous support of an anonymous donor and the Canadian National Railway Company.
Competing interests: None declared.
Correspondence to: Dr. Brian H. Rowe, Department of Emergency Medicine, University of Alberta, Rm. 1G1.43 Walter C. Mackenzie Centre, 8440–112 St., Edmonton AB T6G 2B7; fax 780 407-3982; brian.rowe@ualberta.ca
REFERENCES
- 1.Hockey Canada. About Hockey Canada. Available: www.hockeycanada.ca/index.cfm/ci_id/6698/la_id/1.htm (accessed 2005 Oct 24).
- 2.For the safety of Canadian children and youth. From injury data to preventive measures. Ottawa: Health Canada; 1997.
- 3.Benson BW, Meeuwisse WH. Ice hockey injuries. In: Maffulli N, Caine DJ, editors. Epidemiology of pediatric sports injuries: team sports. Basel: Karger; 2005. p. 62-95.
- 4.Macpherson A, Rothman L, Howard H. Body checking rules and childhood injuries in ice hockey. Pediatrics 2006;117:e143-7. [DOI] [PubMed]
- 5.Montelpare WJ, McPherson MN. Measuring the effects of initiating body checking at the Atom age level. In: Pearsall DJ, Ashare AB, editors. Safety in ice hockey: fourth volume. West Conshohocken (PA): American Society for Testing and Materials International; 2004. p. 70-84.
- 6.Regnier G, Boileau R, Marcotte G, et al. Effects of body checking in the pee-wee (12-and 13-years-old) division in the province of Quebec. In: Castaldi CR, Hoerner EF, editors. Safety in ice hockey. Philadelphia: American Society for Testing and Materials; 1989. p. 84-103.
- 7.Roy M, Bernard D, Roy B, et al. Body checking in pee wee hockey. Phys Sportsmed 1989;17:119-26. [DOI] [PubMed]
- 8.Willer B, Kroetsch B, Darling S, et al. Injury rates in house league, select, and representative youth ice hockey. Med Sci Sports Exerc 2005;37:1658-63. [DOI] [PubMed]
- 9.Hockey Canada. Age groupings in minor hockey will change for 2002-2003 season. Available: www.hockeycanada.ca/index.cfm/ci_id/10567/la_id/1.htm (accessed 2005 October 24).
- 10.Kelly KD, Lissel HL, Rowe BH, et al. Sport and recreation-related head injuries treated in the emergency department. Clin J Sport Med 2001;11:77-81. [DOI] [PubMed]
- 11.Capital Health Population Health and Research Department. Number of Alberta Health Care Insurance Plan registrants as of March 31, 2001–2003. Edmonton: Capital Health; 2005 (data obtained from the Ministry of Health and Wellness, Alberta).
- 12.Rothman K, Greenland S. Modern epidemiology. 2nd ed. Philadelphia: Lippincott-Raven; 1998.
- 13.Dryden D, Rowe BH, Hagel BE, et al. Bodychecking in youth hockey is dangerous [letter]. Med Sci Sports Exerc 2006;38:799. [DOI] [PubMed]
- 14.Trudel P, Bernard D, Boileau R, et al. Effects of an intervention strategy on body checking, penalties, and injuries in ice hockey. In: Ashare AB, editor. Safety in ice hockey: third volume. West Conshohocken (PA): American Society for Testing and Materials; 2000. p. 237-49.
- 15.Pless IB. Expanding the precautionary principle. Inj Prev 2003;9:1-2. [DOI] [PMC free article] [PubMed]