

Abstract
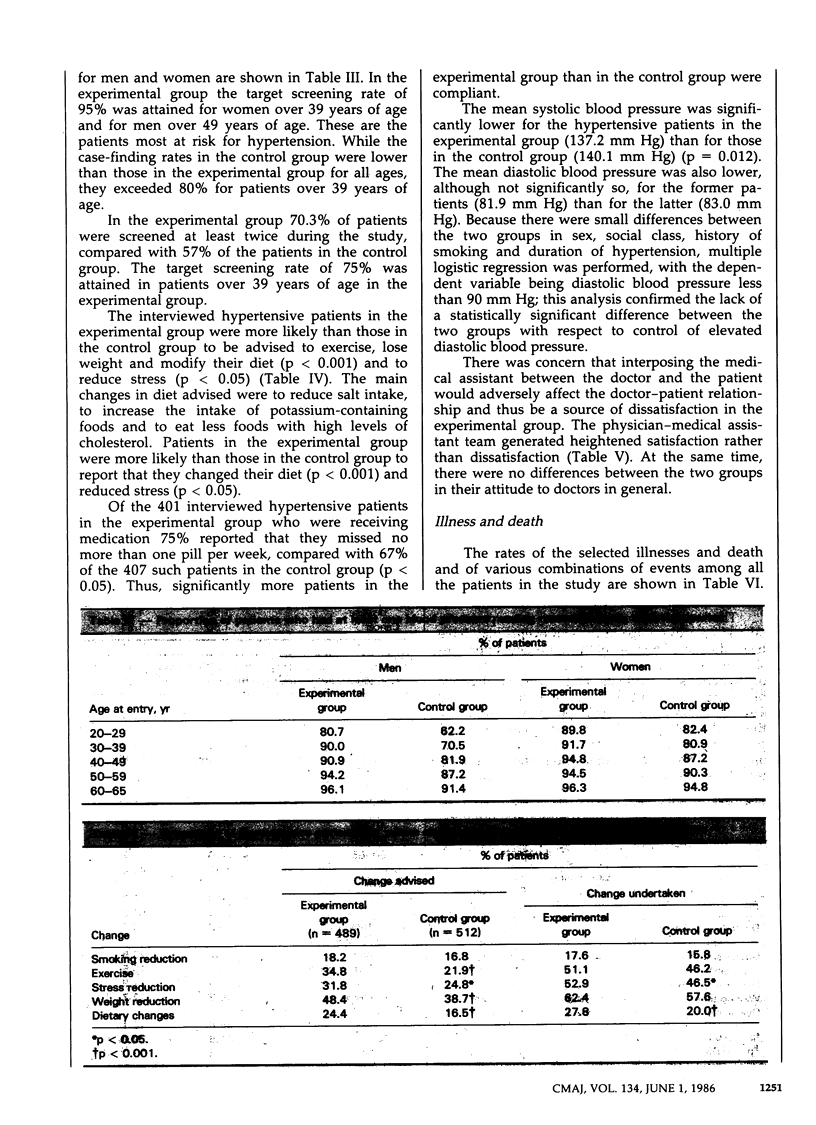
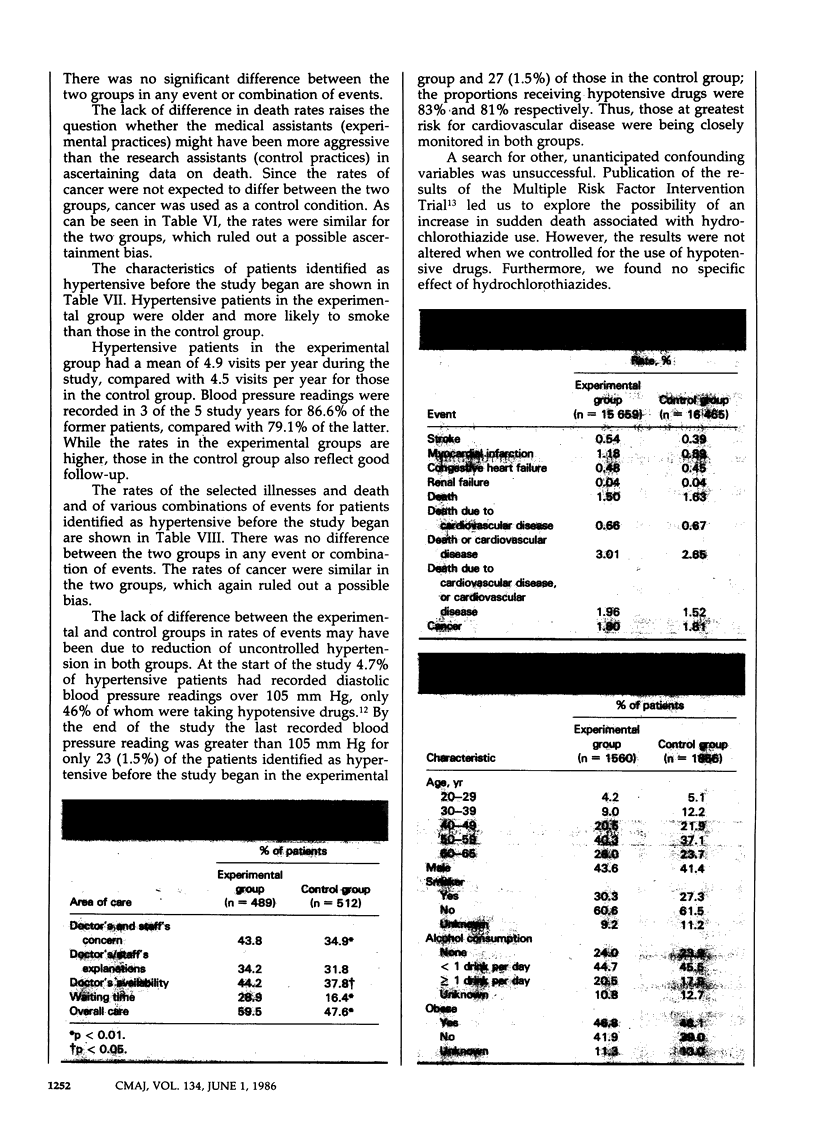
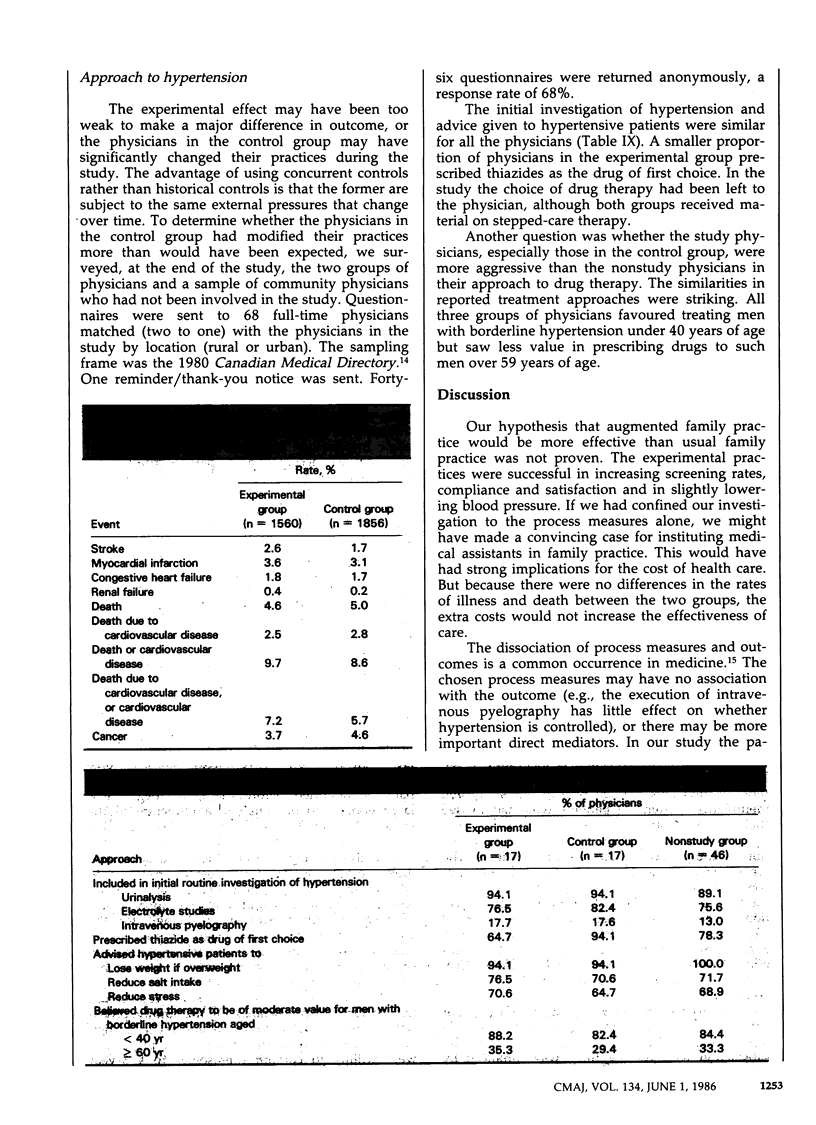
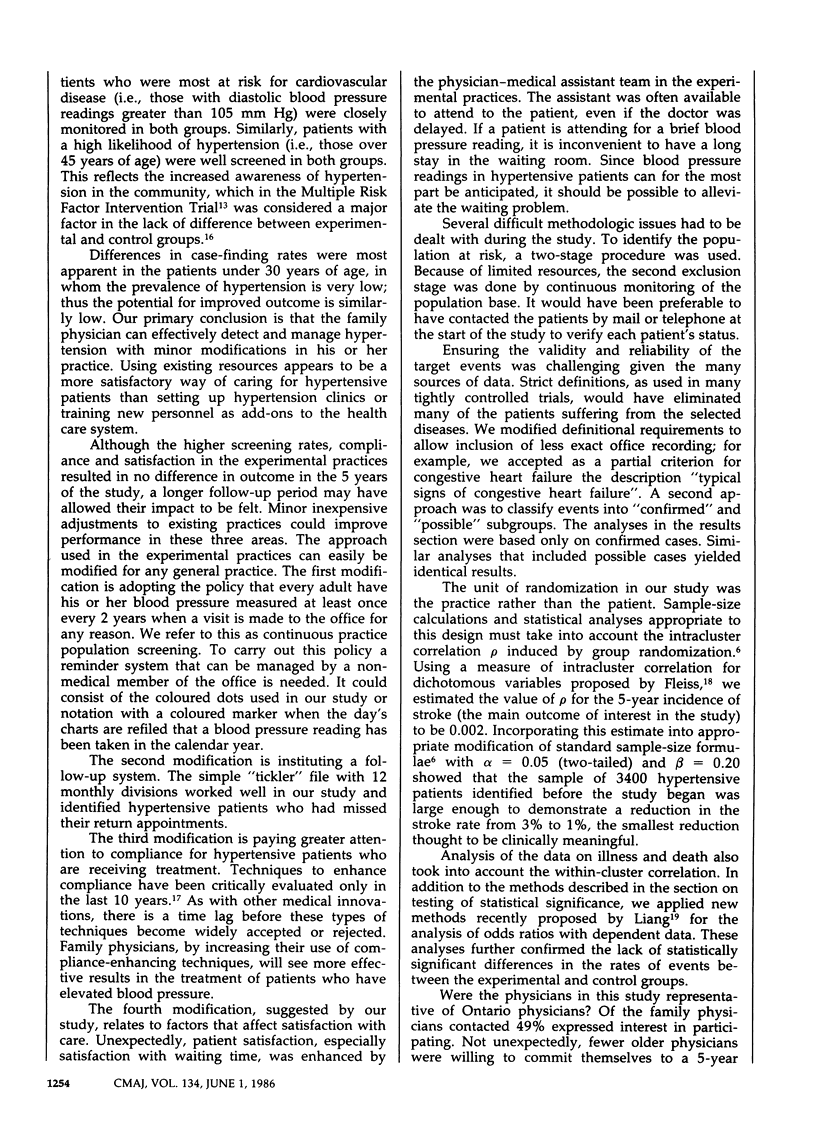
To test a new approach to detecting and managing hypertension, 34 family practices in southwestern Ontario that comprised 32 124 patients aged 20 to 65 years were randomly assigned in a 5-year study to either undertake a system of care in which a medical assistant oversaw screening and attended to education, compliance and follow-up (experimental group) or continue their usual practices (control group). The 17 physicians in the experimental practices (15 659 patients) were matched with the 17 in the control practices (16 465 patients) according to size of the community, sex, level of practice activity and length of time in practice. Hypertension was defined as at least two diastolic blood pressure readings over 90 mm Hg. More patients in the experimental group than in the control group were screened at least once (91% v. 80%); the former were more likely to have lower systolic blood pressure (p less than 0.02), to be compliant (p less than 0.05) and to be very satisfied with care (p less than 0.01). There were no significant differences between the two groups in the rates of illness and death due to cardiovascular disease for all patients or for hypertensive patients. The unassisted family physician can provide effective care for hypertensive patients. However, minor modifications in the physician's practices can improve care.
Full text
PDF
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Birkett N. J., Donner A. P., Maynard M. Prevalence and control of hypertension in an Ontario county. Can Med Assoc J. 1985 May 1;132(9):1019–1024. [PMC free article] [PubMed] [Google Scholar]
- Donner A., Birkett N., Buck C. Randomization by cluster. Sample size requirements and analysis. Am J Epidemiol. 1981 Dec;114(6):906–914. doi: 10.1093/oxfordjournals.aje.a113261. [DOI] [PubMed] [Google Scholar]
- Dunn E., Hilditch J., Chipman M., Hardacre G., Morrison M. Diagnosis and management of hypertension: the stated practices of family physicians. Can Med Assoc J. 1984 Apr 15;130(8):985–988. [PMC free article] [PubMed] [Google Scholar]
- Hart J. T. Semicontinuous screening of a whole community for hypertension. Lancet. 1970 Aug 1;2(7666):223–226. doi: 10.1016/s0140-6736(70)92582-1. [DOI] [PubMed] [Google Scholar]
- Heller R. F., Rose G. Current management of hypertension in general practice. Br Med J. 1977 Jun 4;1(6074):1442–1444. doi: 10.1136/bmj.1.6074.1442. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Luepker R. V., Grimm R. H., Taylor H. L. The effect of "usual care" on cardiovascular risk factors in a clinical trial. Control Clin Trials. 1984 Mar;5(1):47–53. doi: 10.1016/0197-2456(84)90149-1. [DOI] [PubMed] [Google Scholar]
- Schoenberger J. A., Stamler J., Shekelle R. B., Shekelle S. Current status of hypertension control in an industrial population. JAMA. 1972 Oct 30;222(5):559–562. [PubMed] [Google Scholar]
- Spitzer W. O. The nurse practitioner revisited. Slow death of a good idea. N Engl J Med. 1984 Apr 19;310(16):1049–1051. doi: 10.1056/NEJM198404193101610. [DOI] [PubMed] [Google Scholar]
- Wright B. M., Dore C. F. A random-zero sphygmomanometer. Lancet. 1970 Feb 14;1(7642):337–338. doi: 10.1016/s0140-6736(70)90709-9. [DOI] [PubMed] [Google Scholar]
- Zyzanski S. J., Hulka B. S., Cassel J. C. Scale for the measurement of "satisfaction" with medical care: modifications in content, format and scoring. Med Care. 1974 Jul;12(7):611–620. doi: 10.1097/00005650-197407000-00007. [DOI] [PubMed] [Google Scholar]