

Abstract
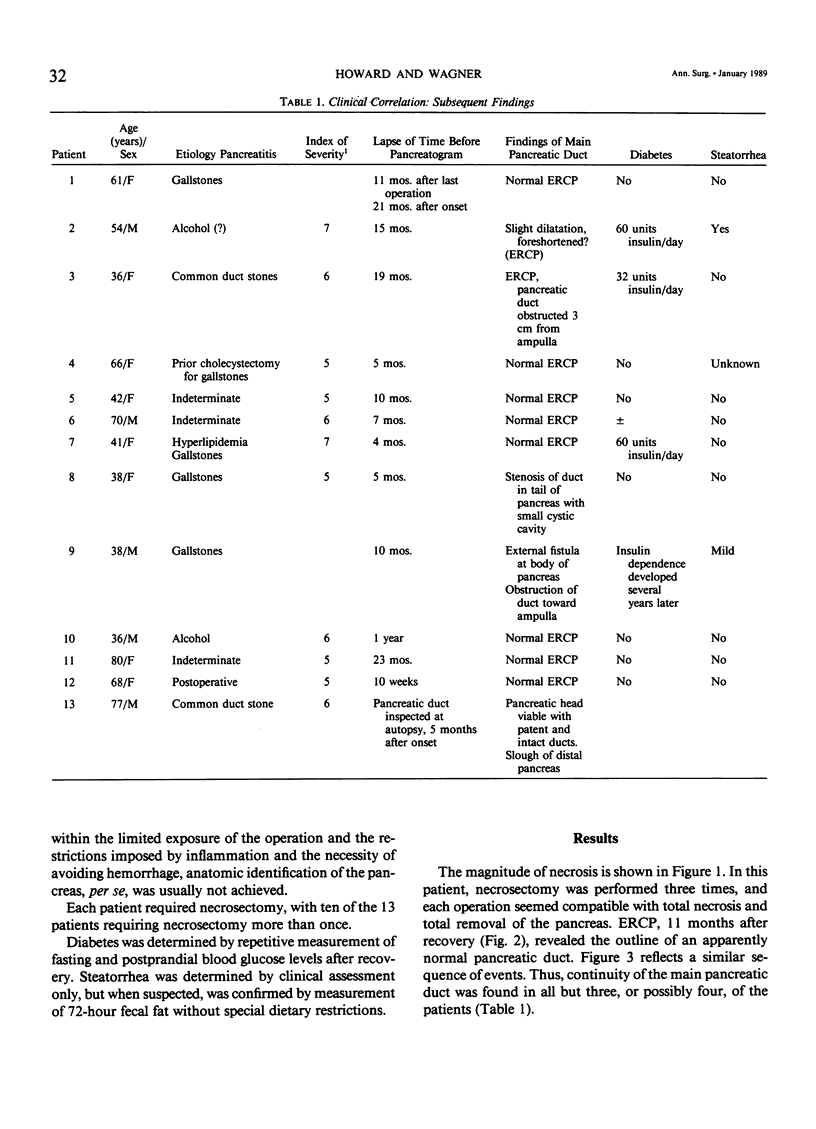
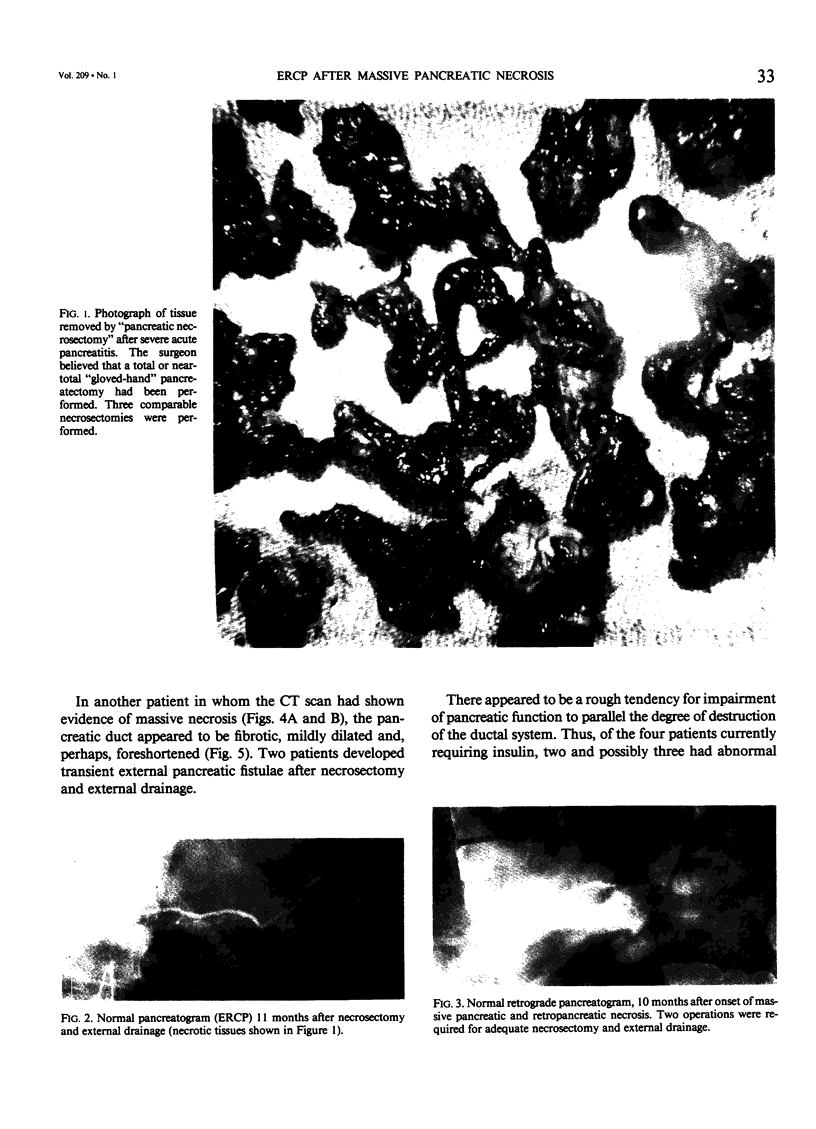
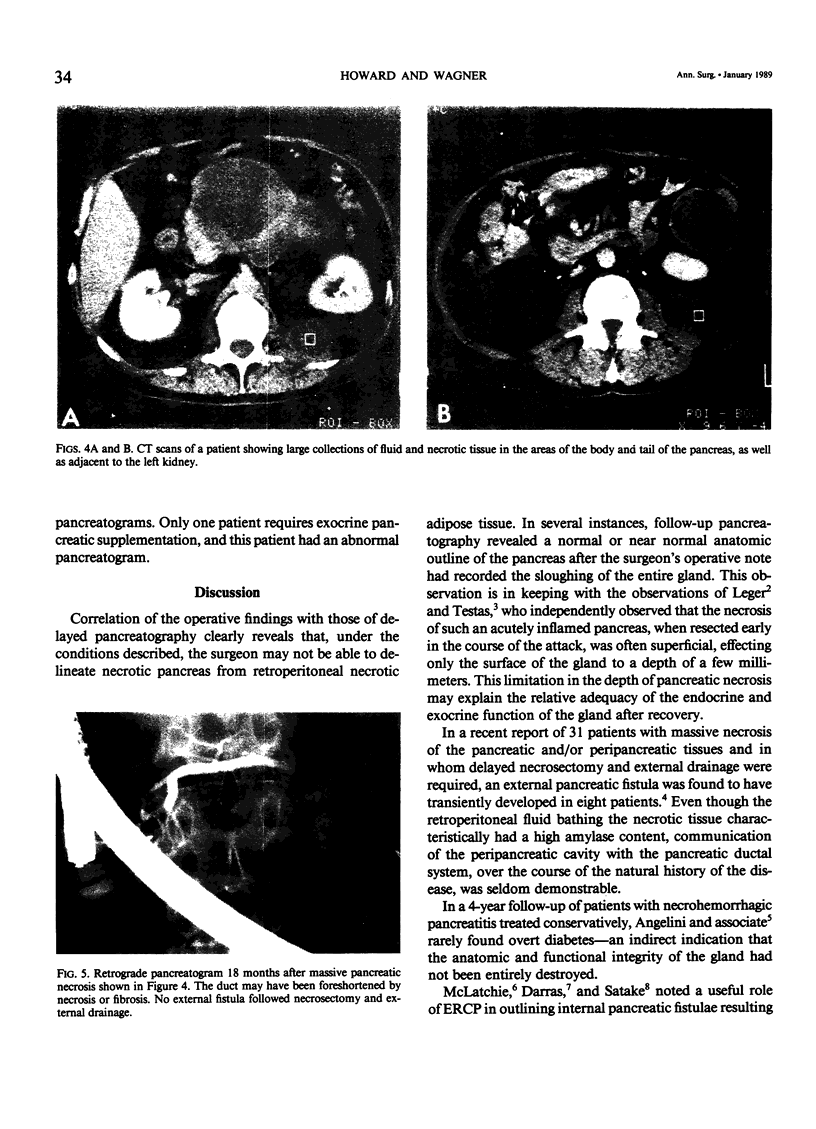
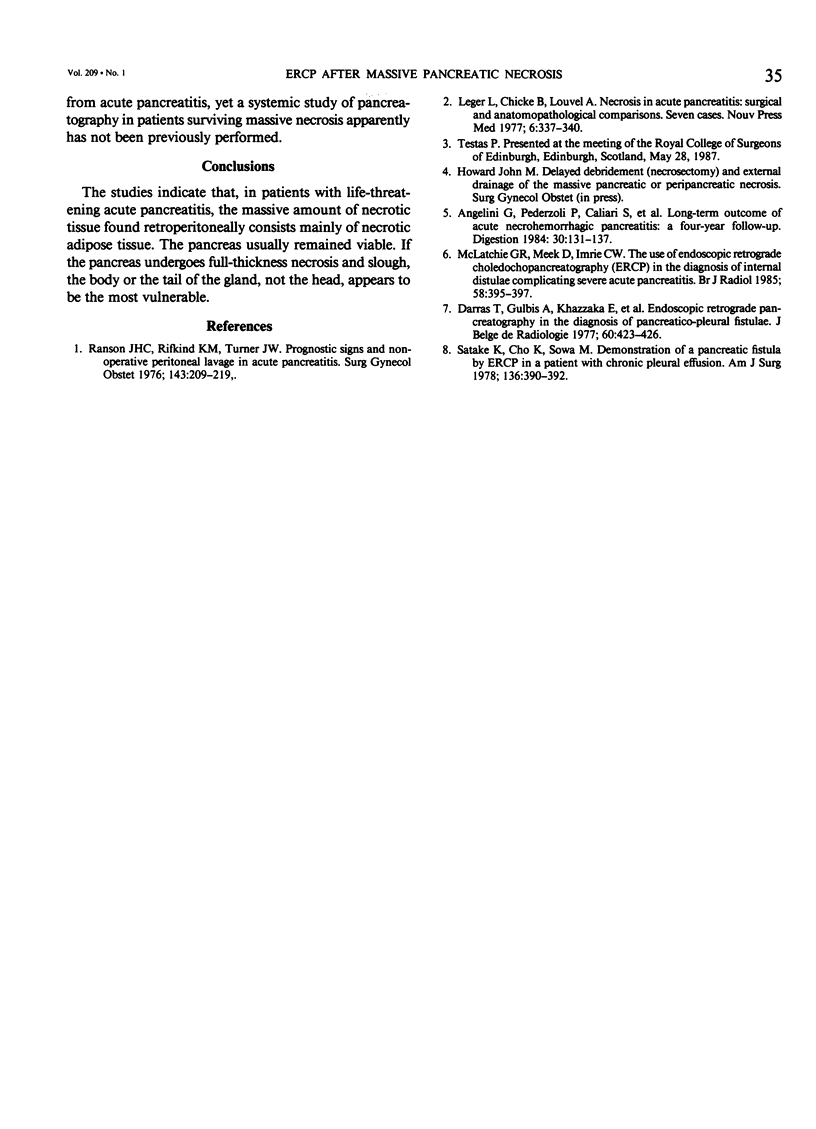
Massive retroperitoneal necrosis may follow life-threatening acute pancreatitis. At delayed operation, the surgeon may not be able to delineate dead pancreas from dead adipose tissue. The question arises: has "gloved hand" debridement resulted in pancreatectomy? The histologists report only "necrotic debris, of uncertain origin." To obtain objective data, pancreatography was performed in 13 patients, 10 weeks to 23 months after onset of massive pancreatic necrosis. Each patient had required delayed laparotomy for debridement and external drainage at some earlier stage of their illness. Pancreatography was correlated with the clinical assessment of diabetes and steatorrhea. Except in specific cases involving internal fistulae, pancreatography has not been previously reported in such patients. The results demonstrate that the main pancreatic duct usually maintained its normal length and configuration. Necrosis or stricture of the main duct, if it occurred, was more likely to be followed by diabetes. Steatorrhea was clinically detected in a single patient only. The necrotic tissue, up to several kilograms in wet weight, is largely dead adipose tissue. The pancreas, especially its head, is resistant to necrosis, much more resistant than is the retroperitoneal fat.
Full text
PDF
Images in this article

Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Angelini G., Pederzoli P., Caliari S., Fratton S., Brocco G., Marzoli G., Bovo P., Cavallini G., Scuro L. A. Long-term outcome of acute necrohemorrhagic pancreatitis. A 4-year follow-up. Digestion. 1984;30(3):131–137. doi: 10.1159/000199097. [DOI] [PubMed] [Google Scholar]
- Darras T., Gulbis A., Khazzaka E., Massaer J., Van Cauter J. Endoscopic retrograde pancreatography in the diagnosis of pancreatico-pleural fistula. J Belge Radiol. 1977;60(5):423–426. [PubMed] [Google Scholar]
- Leger L., Chiche B., Louvel A. La nécrose dans les pancréatites aiguüs. Confrontations opératoires et anatomo-pathologiques. 7 observations. Nouv Presse Med. 1977 Feb 5;6(5):337–340. [PubMed] [Google Scholar]
- McLatchie G. R., Meek D., Imrie C. W. The use of endoscopic retrograde choledocho pancreatography (ERCP) in the diagnosis of internal fistulae complicating severe acute pancreatitis. Br J Radiol. 1985 May;58(689):395–397. doi: 10.1259/0007-1285-58-689-395. [DOI] [PubMed] [Google Scholar]
- Ranson J. H., Rifkind K. M., Turner J. W. Prognostic signs and nonoperative peritoneal lavage in acute pancreatitis. Surg Gynecol Obstet. 1976 Aug;143(2):209–219. [PubMed] [Google Scholar]
- Satake K., Cho K., Sowa M., Umeyama K., Tatsumi S., Mitani E., Kobayashi K. Demonstration of a pancreatic fistula by endoscopic pancreatography in a patient with chronic pleural effusion. Am J Surg. 1978 Sep;136(3):390–392. doi: 10.1016/0002-9610(78)90302-1. [DOI] [PubMed] [Google Scholar]