

Abstract
Most pediatricians and family physicians believe that children with pectus excavatum require surgery only for cosmetic indications and then only in teenagers. We believe pectus excavatum should be repaired in childhood (1) to relieve structural compression of the chest and allow normal growth of the thorax; (2) to prevent pulmonary and cardiac dysfunction in teenagers and adults; and (3) to obviate the cosmetic impact that may cause a child to avoid sports and gymnastics. Preoperative CT scans now help select those children who need repair to prevent progressive deformities. Pulmonary function studies during vigorous exercise can document respiratory dysfunction in teenagers. These features are reversible if repair is completed before the pubertal growth spurt. The ideal age for repair is 4 to 6 years, which permits enough emotional maturity for a positive hospital experience and avoids later psychological effects. Repair at an earlier age has no operative advantages. Our operative technique consists of the removal of three to four overgrown costal cartilages, repositioning of the sternum with a transverse osteotomy, and internal support using the child's lowest normal ribs, avoiding any prosthetic support. To prevent recurrence in teenagers, we add a temporary bar beneath the sternum to prevent depression of the sternum from the weight of the chest-wall muscle mass. Six hundred sixty-four patients have been followed for 1 to 40 years; 95% have excellent long-term results and only 5% have mild to moderate recurrences. Our current techniques of patient selection and surgery will be presented.
Full text
PDF


Images in this article
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- BEVEGARD S. Postural circulatory changes at rest and during exercise in patients with funnel chest, with special reference to factors affecting the stroke volume. Acta Med Scand. 1962 Jun;171:695–713. [PubMed] [Google Scholar]
- Beiser G. D., Epstein S. E., Stampfer M., Goldstein R. E., Noland S. P., Levitsky S. Impairment of cardiac function in patients with pectus excavatum, with improvement after operative correction. N Engl J Med. 1972 Aug 10;287(6):267–272. doi: 10.1056/NEJM197208102870602. [DOI] [PubMed] [Google Scholar]
- Blickman J. G., Rosen P. R., Welch K. J., Papanicolaou N., Treves S. T. Pectus excavatum in children: pulmonary scintigraphy before and after corrective surgery. Radiology. 1985 Sep;156(3):781–782. doi: 10.1148/radiology.156.3.4023243. [DOI] [PubMed] [Google Scholar]
- Cahill J. L., Lees G. M., Robertson H. T. A summary of preoperative and postoperative cardiorespiratory performance in patients undergoing pectus excavatum and carinatum repair. J Pediatr Surg. 1984 Aug;19(4):430–433. doi: 10.1016/s0022-3468(84)80268-7. [DOI] [PubMed] [Google Scholar]
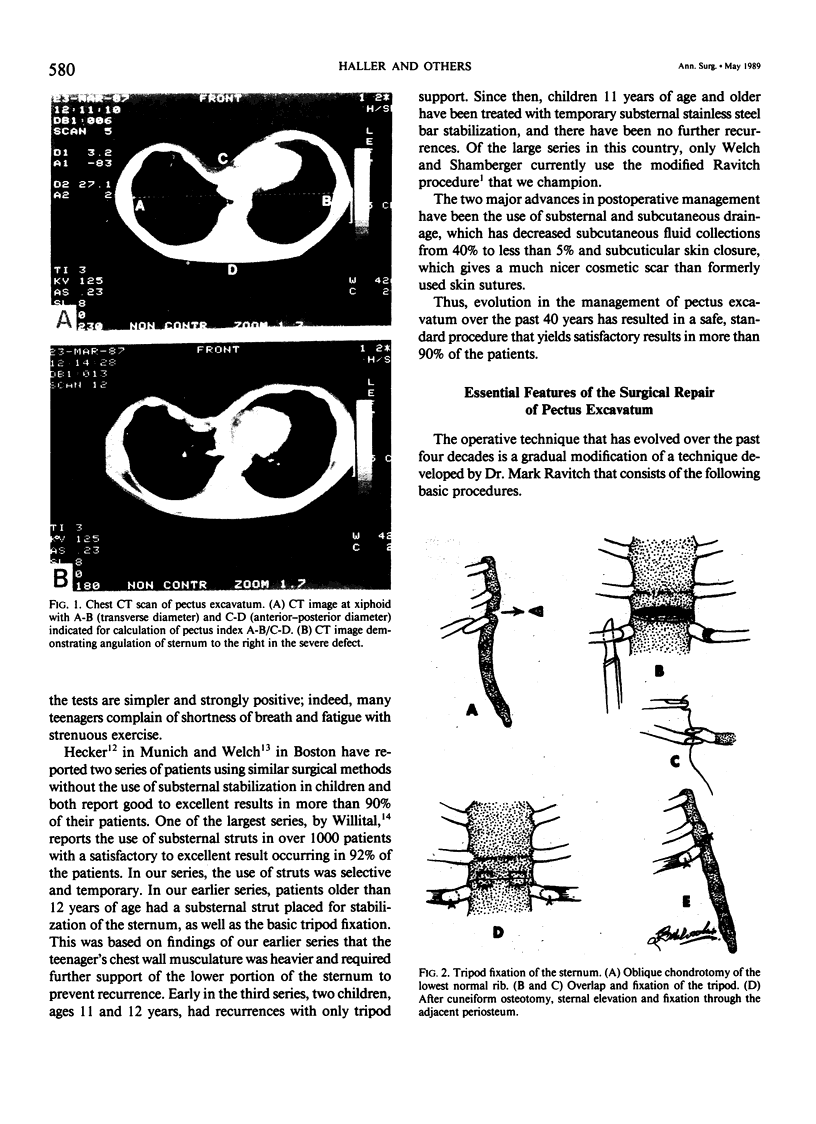
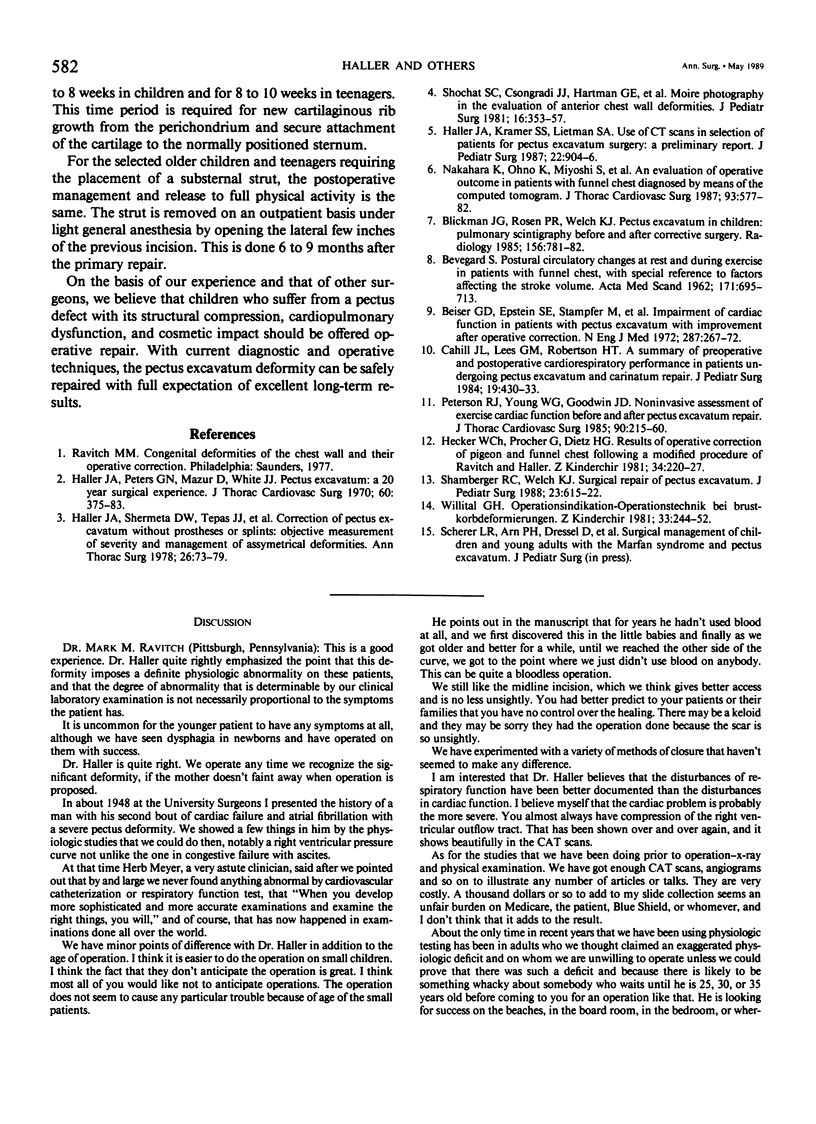
- Haller J. A., Jr, Kramer S. S., Lietman S. A. Use of CT scans in selection of patients for pectus excavatum surgery: a preliminary report. J Pediatr Surg. 1987 Oct;22(10):904–906. doi: 10.1016/s0022-3468(87)80585-7. [DOI] [PubMed] [Google Scholar]
- Haller J. A., Jr, Peters G. N., Mazur D., White J. J. Pectus excavatum. A 20 year surgical experience. J Thorac Cardiovasc Surg. 1970 Sep;60(3):375–383. [PubMed] [Google Scholar]
- Haller J. A., Jr, Shermeta D. W., Tepas J. J., Bittner H. R., Golladay E. S. Correction of pectus excavatum without prostheses or splints: objective measurement of severity and management of asymmetrical deformities. Ann Thorac Surg. 1978 Jul;26(1):73–79. doi: 10.1016/s0003-4975(10)63635-1. [DOI] [PubMed] [Google Scholar]
- Nakahara K., Ohno K., Miyoshi S., Maeda H., Monden Y., Kawashima Y. An evaluation of operative outcome in patients with funnel chest diagnosed by means of the computed tomogram. J Thorac Cardiovasc Surg. 1987 Apr;93(4):577–582. [PubMed] [Google Scholar]
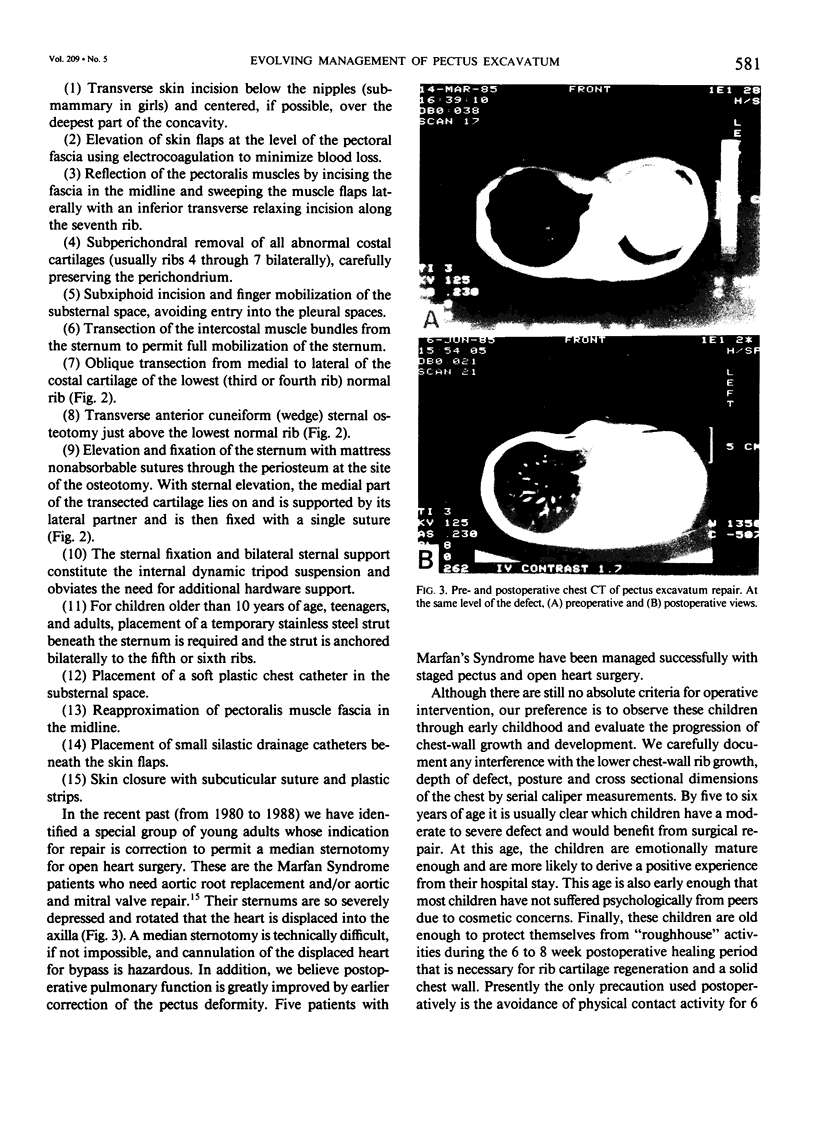
- Shamberger R. C., Welch K. J. Surgical repair of pectus excavatum. J Pediatr Surg. 1988 Jul;23(7):615–622. doi: 10.1016/s0022-3468(88)80629-8. [DOI] [PubMed] [Google Scholar]
- Shochat S. J., Csongradi J. J., Hartman G. E., Rinsky L. A. Moiré phototopography in the evaluation of anterior chest wall deformities. J Pediatr Surg. 1981 Jun;16(3):353–357. doi: 10.1016/s0022-3468(81)80694-x. [DOI] [PubMed] [Google Scholar]
- Willital G. H. Operationsindikation - Operationstechnik bei Brustkorbdeformierungen. Z Kinderchir. 1981 Jul;33(3):244–252. doi: 10.1055/s-2008-1063126. [DOI] [PubMed] [Google Scholar]