

Abstract
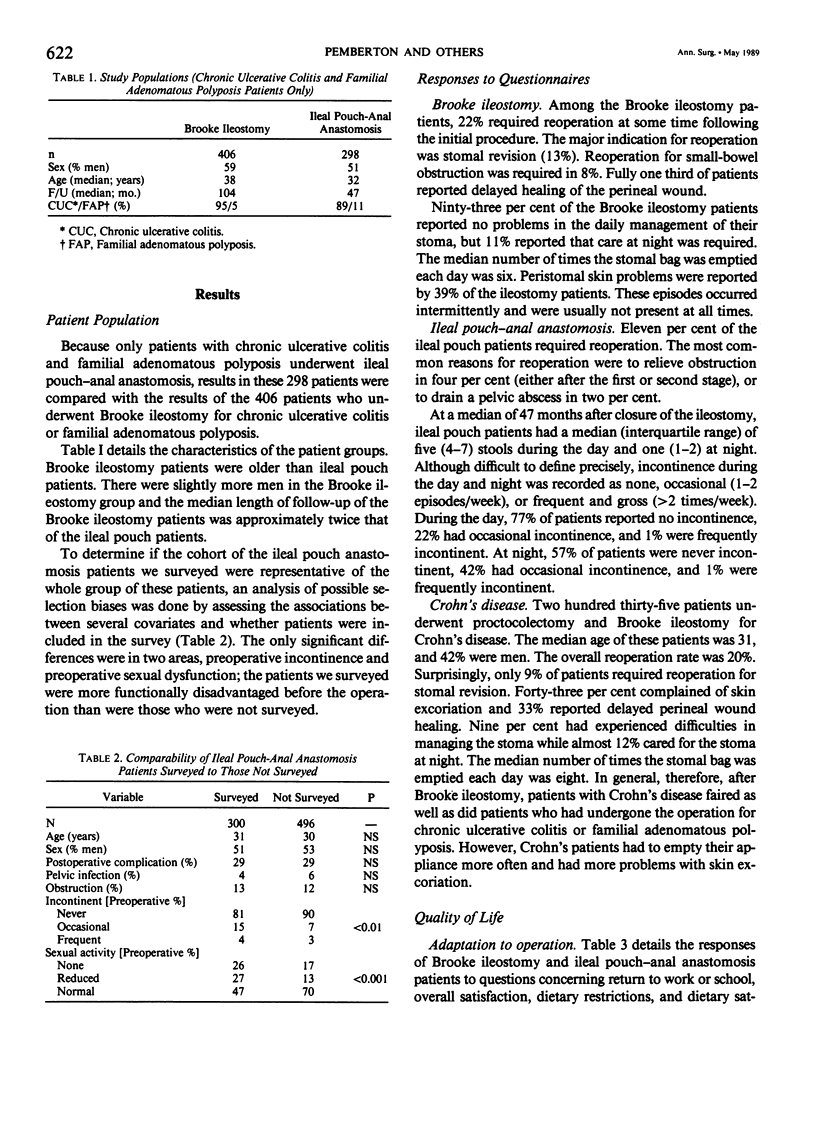
Although the clinical results of Brooke ileostomy are good, patients are permanently incontinent of stool and gas. Alternative operations designed to restore enteric continence, such as ileal pouch-anal anastomosis, must not only be as safe and effective as Brooke ileostomy, but should provide an improved quality of life in order to establish long-term acceptability. Ileal pouch-anal anastomosis has been performed safely and good functional results have been reported. The quality of life after ileal pouch-anal anastomosis, however, has not been documented. Two hundred ninety-eight ileal pouch patients and 406 Brooke ileostomy patients who had the operations performed for chronic ulcerative colitis or familial adenomatous polyposis formed the basis of the study. After adjusting for age, diagnosis, and reoperation rate, logistic regression analysis of performance scores in seven different categories was used to discriminate between operations. Median follow-up was longer in Brooke ileostomy patients than in ileal pouch patients (104 months vs. 47 months, respectively), and Brooke ileostomy patients were slightly older (38 years vs. 32 years). A great majority of patients in each group were satisfied (93% Brooke ileostomy; 95% ileal pouch-anal anastomosis). Thirty-nine per cent of Brooke ileostomy patients, however, desired a change in the type of ileostomy they had. At 47 months, ileal pouch patients had a median of 5 stools per day and 1 at night, 77% did not experience any daytime incontinence, while 22% reported occasional spotting. In each performance category, the performance score discriminated between operations, with the probability of having had an ileal pouch-anal anastomosis operation increasing with improvement in performance scores (p less than 0.05). We concluded that after ileal pouch-anal anastomosis, patients experienced significant advantages in performing daily activities compared to patients with Brooke ileostomy and thus may experience a better quality of life. These results help further to establish ileal pouch-anal anastomosis as a safe, attractive, and valid alternative to Brooke ileostomy.
Full text
PDF






Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- BROOKE B. N. Outcome of surgery for ulcerative colitis. Lancet. 1956 Sep 15;271(6942):532–536. doi: 10.1016/s0140-6736(56)92021-9. [DOI] [PubMed] [Google Scholar]
- BROOKE B. N. The management of an ileostomy, including its complications. Lancet. 1952 Jul 19;2(6725):102–104. doi: 10.1016/s0140-6736(52)92149-1. [DOI] [PubMed] [Google Scholar]
- Ballantyne G. H., Pemberton J. H., Beart R. W., Jr, Wolff B. G., Dozois R. R. Ileal J pouch-anal anastomosis. Current technique. Dis Colon Rectum. 1985 Mar;28(3):197–202. doi: 10.1007/BF02554246. [DOI] [PubMed] [Google Scholar]
- Becker J. M., Raymond J. L. Ileal pouch-anal anastomosis. A single surgeon's experience with 100 consecutive cases. Ann Surg. 1986 Oct;204(4):375–383. doi: 10.1097/00000658-198610000-00005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Boné J., Sorensen F. H. Life with a conventional heostomy. Dis Colon Rectum. 1974 Mar-Apr;17(2):194–199. doi: 10.1007/BF02588103. [DOI] [PubMed] [Google Scholar]
- Burnham W. R., Lennard-Jones J. E., Brooke B. N. Sexual problems among married ileostomists. Survey conducted by The Ileostomy Association of Great Britain and Ireland. Gut. 1977 Aug;18(8):673–677. doi: 10.1136/gut.18.8.673. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cohen Z., McLeod R. S. Proctocolectomy and ileoanal anastomosis with J-shaped or S-shaped ileal pouch. World J Surg. 1988 Apr;12(2):164–168. doi: 10.1007/BF01658048. [DOI] [PubMed] [Google Scholar]
- Druss R. G., O'Connor J. F., Prudden J. F., Stern L. O. Psychologic response to colectomy. Arch Gen Psychiatry. 1968 Jan;18(1):53–59. doi: 10.1001/archpsyc.1968.01740010055008. [DOI] [PubMed] [Google Scholar]
- Failes D. The Kock continent ileostomy: a preliminary report. Aust N Z J Surg. 1976 May;46(2):125–130. doi: 10.1111/j.1445-2197.1976.tb03214.x. [DOI] [PubMed] [Google Scholar]
- Grüner O. P., Naas R., Fretheim B., Gjone E. Marital status and sexual adjustment after colectomy. Results in 178 patients operated on for ulcerative colitis. Scand J Gastroenterol. 1977;12(2):193–197. doi: 10.1203/00006450-199404000-00018. [DOI] [PubMed] [Google Scholar]
- Kock N. G., Darle N., Hultén L., Kewenter J., Myrvold H., Philipson B. Ileostomy. Curr Probl Surg. 1977 Aug;14(8):1–52. doi: 10.1016/s0011-3840(77)80065-8. [DOI] [PubMed] [Google Scholar]
- Kock N. G., Darle N., Kewenter J., Myrvold H., Philipson B. The quality of life after proctocolectomy and ileostomy: a study of patients with conventional ileostomies converted to continent ileostomies. Dis Colon Rectum. 1974 May-Jun;17(3):287–292. doi: 10.1007/BF02586968. [DOI] [PubMed] [Google Scholar]
- Lyttle J. A., Parks A. G. Intersphincteric excision of the rectum. Br J Surg. 1977 Jun;64(6):413–416. doi: 10.1002/bjs.1800640611. [DOI] [PubMed] [Google Scholar]
- Metcalf A. M., Dozois R. R., Kelly K. A., Beart R. W., Jr, Wolff B. G. Ileal "J" pouch-anal anastomosis. Clinical outcome. Ann Surg. 1985 Dec;202(6):735–739. doi: 10.1097/00000658-198512000-00013. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Morowitz D. A., Kirsner J. B. Ileostomy in ulcerative colitis. A questionnaire study of 1,803 patients. Am J Surg. 1981 Mar;141(3):370–375. doi: 10.1016/0002-9610(81)90199-9. [DOI] [PubMed] [Google Scholar]
- Nicholls R. J., Pezim M. E. Restorative proctocolectomy with ileal reservoir for ulcerative colitis and familial adenomatous polyposis: a comparison of three reservoir designs. Br J Surg. 1985 Jun;72(6):470–474. doi: 10.1002/bjs.1800720622. [DOI] [PubMed] [Google Scholar]
- Pemberton J. H., Kelly K. A., Beart R. W., Jr, Dozois R. R., Wolff B. G., Ilstrup D. M. Ileal pouch-anal anastomosis for chronic ulcerative colitis. Long-term results. Ann Surg. 1987 Oct;206(4):504–513. doi: 10.1097/00000658-198710000-00011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rhodes J. B., Kirsner J. B. The early and late course of patients with ulcerative colitis after ileostomy and colectomy. Surg Gynecol Obstet. 1965 Dec;121(6):1303–1314. [PubMed] [Google Scholar]
- Roy P. H., Sauer W. G., Beahrs O. H., Farrow G. M. Experience with ileostomies. Evaluation of long-term rehabilitation in 497 patients. Am J Surg. 1970 Jan;119(1):77–86. doi: 10.1016/0002-9610(70)90016-4. [DOI] [PubMed] [Google Scholar]
- Sugarbaker P. H., Barofsky I., Rosenberg S. A., Gianola F. J. Quality of life assessment of patients in extremity sarcoma clinical trials. Surgery. 1982 Jan;91(1):17–23. [PubMed] [Google Scholar]
- Taylor B. M., Beart R. W., Jr, Dozois R. R., Kelly K. A., Phillips S. F. Straight ileoanal anastomosis v ileal pouch--anal anastomosis after colectomy and mucosal proctectomy. Arch Surg. 1983 Jun;118(6):696–701. doi: 10.1001/archsurg.1983.01390060018004. [DOI] [PubMed] [Google Scholar]
- WILSON E. THE REHABILITATION OF PATIENTS WITH AN ILEOSTOMY ESTABLISHED FOR ULCERATIVE COLITIS. Med J Aust. 1964 May 30;1:842–845. doi: 10.5694/j.1326-5377.1964.tb114356.x. [DOI] [PubMed] [Google Scholar]
- Watts J. M., de Dombal F. T., Goligher J. C. Long-term complications and prognosis following major surgery for ulcerative colitis. Br J Surg. 1966 Dec;53(12):1014–1023. doi: 10.1002/bjs.1800531203. [DOI] [PubMed] [Google Scholar]
- Williams N. S., Johnston D. The current status of mucosal proctectomy and ileo-anal anastomosis in the surgical treatment of ulcerative colitis and adenomatous polyposis. Br J Surg. 1985 Mar;72(3):159–168. doi: 10.1002/bjs.1800720302. [DOI] [PubMed] [Google Scholar]