

Abstract
OBJECTIVE
We investigated naturally occurring feedback incidents to substantiate literature-based recommended techniques for giving feedback effectively.
SETTING
A faculty development course for improving the teaching of the medical interview, with opportunities for participants to receive feedback.
PARTICIPANTS
Seventy-four course participants (clinician-educators from a wide range of medical disciplines, and several behavioral scientists).
MEASUREMENTS AND MAIN RESULTS
We used qualitative and quantitative approaches. Participants provided narratives of helpful and unhelpful incidents experienced during the course and then rated their own narratives using a semantic-differential survey. We found strong agreement between the two approaches, and congruence between our data and the recommended literature. Giving feedback effectively includes: establishing an appropriate interpersonal climate; using an appropriate location; establishing mutually agreed upon goals; eliciting the learner's thoughts and feelings; reflecting on observed behaviors; being nonjudgmental; relating feedback to specific behaviors; offering the right amount of feeback; and offering suggestions for improvement.
CONCLUSIONS
Feedback techniques experienced by respondents substantiate the literature-based recommendations, and corrective feedback is regarded as helpful when delivered appropriately. A model for providing feedback is offered.
Keywords: giving feedback, faculty development, narrative inquiry, semantic differential
Feedback is central to medical education in promoting learning and ensuring that standards are met. Unfortunately, it is a difficult component of clinical teaching, and clinical teachers often avoid this aspect of their responsibilities.1 In a survey of residents' perceptions of the evaluation process at a large academic medical center, where residents and staff are evaluated on standard written forms at the end of each rotation, only 8% of residents (n= 65) reported being “very satisfied” with the feedback process. Eighty percent of the residents reported never or infrequently receiving corrective feedback from their attending physicians, 20% reported sometimes receiving corrective feedback, and none reported receiving it often. Moreover, 17% of the residents reported never or infrequently receiving reinforcing feedback, 52% reported receiving it sometimes, and 31% reported receiving it often.2 In faculty development courses clinical teachers frequently indicate that their greatest need is to learn how to give feedback more effectively (Hewson, personal experience). Difficulty in giving feedback may be based on reluctance to give offense or provoke undue defensiveness in the medical students.1
Numerous authors in both medical and business education have proposed several techniques necessary for giving effective feedback.1, 3, 4 These are listed in Table 1 in the form of nine recommended techniques (as well as the converse nonrecommended techniques). There is, however, little data to substantiate these recommended techniques, especially in medical education.
Table 1.
Bipolar Descriptors of Recommended and Nonrecommended Feedback Techniques
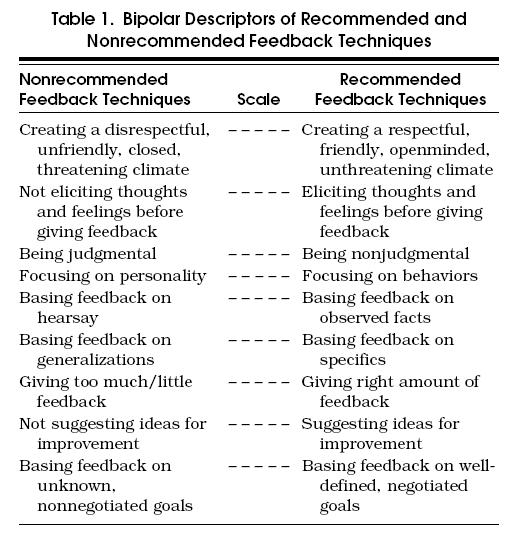
We aimed to substantiate the recommendations found in the literature and to clarify and elaborate on these recommendations. We made the assumption that if a person perceives an incident involving feedback to be helpful (whether the feedback is corrective or reinforcing), the feedback technique(s) used are probably effective. Conversely, if a person perceives a feedback incident as unhelpful (whether the feedback is corrective or reinforcing), the feedback techniques used are probably ineffective. We hypothesized that recommended feedback techniques would be associated with feedback incidents perceived as helpful, and nonrecommended feedback techniques would be associated with the feedback incidents perceived as unhelpful, and we expected a reciprocal relation between the recommended and nonrecommended techniques.
We investigated clinician teachers' personal experiences with receiving feedback in a course for improving the teaching of medical interviewing (the annual training course of the American Academy of Physician and Patient). This course is designed to help clinicians improve their patient-clinician communication skills, as well as to focus on how to teach these skills to medical trainees (residents and medical students).5 The 1-week course was participant-centered, experiential, interactive, and intensive. Small groups of four or five participants, each with a facilitator, worked together to improve their clinical communication and teaching skills. In six 2-hour training sessions, participants interviewed real patients (both inpatients and outpatients), simulated patients, residents, and medical students, and engaged in role plays of encounters involving interesting or provocative communication between clinicians and patients or between clinicians and their trainees. These encounters were then discussed in the working groups, which provided many opportunities for participants to receive feedback from peers, as well as from facilitators.
In many ways, the teaching methods used in the faculty development course were similar to those commonly used in teaching residents and medical students. In both situations, medical trainees and course participants first engage in unrehearsed medical encounters and are then given feedback. In clinical education, the feedback is given by attending physicians or residents, but in the training course it was given by participants' peers and the group facilitators.
METHODS
Setting and Study Population
The course participants (N= 83) consisted of academics from approximately 60 different medical institutions, mainly from the United States, but also from Canada and the United Kingdom. All participants, by definition, wanted to improve their skills in medical interviewing, and learn how to teach these skills to others. Of the 39 men and 44 women, 64 were physicians (representing a wide range of medical disciplines) and 19 were behavioral scientists (psychologists, social workers, nurses, public health specialists, and educators). Most participants (80%) were participating in the course for the first time. The course was staffed by 25 facilitators (physicians and behavioral scientists) who came from as many different institutions. The facilitators were not included in the study.
Data Sources
We collected data on feedback techniques (both reinforcing and corrective) used by feedback-givers in incidents perceived by recipients as helpful and unhelpful. We used both qualitative and quantitative methods. Qualitative methods were used to elicit narratives of feedback-giving incidents perceived by recipients as helpful and unhelpful.6, 7 The quantitative methods involved participants rating their own narratives using an instrument (semantic differential) to check the efficacy of the literature-based recommendations for giving feedback.8, 9
Narratives
At the conclusion of the 1-week course, each participant was asked to provide a short narrative of two selected course-related feedback incidents, one of which they judged as personally helpful, and the other as personally unhelpful. We used narrative inquiry, a qualitative research approach, involving open coding techniques designed to identify the meaning and significance of the complex interactions of giving feedback.6, 7 First, we characterized the feedback narrative as either corrective (negative) or reinforcing (positive). Then we analyzed the narratives in greater detail to identify discrete techniques. We coded these techniques and categorized them into similar conceptual groups.
Ratings
We sought to validate the literature-based recommended feedback techniques by asking the participants to rate their own narratives using a semantic-differential survey instrument.8, 9 The major advantage of the semantic differential is its ability to provide a profile showing the parameters of the meaning of the concept under study. We chose the semantic differential to measure and compare respondents' understanding of two concepts, corrective and reinforcing feedback. (Note: we were measuring neither the individuals nor the course.) We generated the semantic differential scales using unidimensional pairs of descriptors that were constructed by juxtaposing a recommended technique with its converse, a nonrecommended technique. All techniques were derived from the literature.1, 3, 4 The instrument thus had nine bipolar descriptors, each with a 5-point, bipolar rating scale. Respondents were requested to mark the place on the scale that most closely represented how well a descriptor (or its converse) was associated with the incident being described.Table 1 represents the bipolar scales.
Each scale was weighted (in terms of directionally) according to the literature, by arbitrarily assigning the range of the recommended techniques to be 3.1 to 5.0, and the range of the nonrecommended techniques to be 1.0 to 2.9. The neutral point was 3.0, which meant that either the technique was not descriptive of the incident, or the respondent could not decide, or did not understand the question. The directionality of the scales was purposely mixed on the instrument. The researchers gave all reported incidents (helpful and unhelpful) a score between 1 and 5 on each of the bipolar scales based on the position of the mark. An interpretive example follows: On the bipolar scale, “created a respectful climate versus created a disrespectful climate,” a specified helpful feedback incident that received a rating of 4.0 would indicate that the respondent associated the incident with the technique “created a respectful climate.” Conversely, a rating of 2.0 would mean that the respondent associated the incident with the technique “created a disrespectful climate.”
We calculated the mean scores and confidence intervals (CI) for the group on each scale and generated profiles of the two concepts: helpful and unhelpful feedback. We then calculated the Spearman rank correlation coefficient between the two sets of scores and calculated the difference between the mean scores to identify their significance (Student's t test). Finally we compared our results from the qualitative and quantitative analyses.
RESULTS
We received responses from 74 (89%) of the 83 participants. All 74 provided narratives plus ratings of helpful feedback incidents, and 28 also provided narratives and ratings of unhelpful feedback incidents.
Qualitative Analyses
Helpful Feedback Techniques.
The qualitative analyses showed that feedback techniques in helpful incidents included a focus on “skills” as well as “personal styles.” Reinforcing feedback included focus on specific skills such as being able to lead a group discussion, giving feedback, setting up a role play, and handling challenging incidents. Reinforcing feedback also focused on personal styles, such as being quiet, verbally assertive, being nonthreatening, flexible, and being facilitative. For example: “I was complimented in detailed, specific ways for giving good feedback” and “I was reinforced for my verbal assertiveness in sharing a story.”
Similarly, corrective feedback included “focus on skills in group dynamics” (overfunctioning, overprotecting others in the group, not introducing myself, isolating someone, going too far, crossing someone's personal boundaries, and giving feedback poorly). Helpful corrective feedback also involved personal styles (talking too much, saying “OK” too much, being unspecific, “sermonizing,” and interrupting others), and personal approaches (coming across as harsh and threatening, and not appreciating the goals of others). Respondents also described helpful feedback incidents that were neutral in content (neither corrective nor reinforcing) involving learning, such as “I learned the difference between sharing a story versus sharing my own feelings about what someone else is saying.”
The way in which feedback was given to participants strongly affected their perceptions of its helpfulness. For example, helpful incidents were associated with techniques such as “giving feedback lovingly, supportively, and caringly,”“being gentle and not hitting someone over the head with his or her mistakes,” and “being concerned to understand the other person's position.” Participants appreciated accurate and clear feedback about particular behaviors. Feedback that included specific suggestions for improvement was seen as very important, especially if someone modeled what he or she had in mind. Being able to request and then to receive feedback was also appreciated. An example of helpful, corrective feedback illustrates several of these behaviors:
While viewing with others a videotape of an interview with a simulated patient [in which] I was the interviewer, I realized that I looked and felt uncomfortable. I sought feedback from others without first stating my own impressions. I got the feedback that I seemed competent, businesslike, but grim.... The group's observations corroborated and brought into clearer focus my own. Then there was some useful discussion about how I could modify my style and take better care of myself. This may be a turning point for me. I was amazed to see how much genuine caring can be manifested by strangers, and how helpful it can be.
In this quotation, we understand that a friendly, caring climate was established. The participant sought particular feedback from this group. In group discussion, she described her personal goals and her problem. This participant asked the group to reflect on their observations of her behaviors and used them to clarify her self-assessment. During the ensuing discussion on how to modify her style, she received suggestions for improvement.
Unhelpful Feedback Techniques.
One participant perceived a reinforcing positive feedback incident as unhelpful, suggesting that it was too general, unspecific, and did not address the link between the action and the person. A technique consistently associated with unhelpful incidents involved not eliciting a person's ideas, feelings, or goals; for example, “feedback was based on goals different from mine, indicating a lack of understanding,” and “feedback involved another participant projecting his or her own safety issues onto others.” Feedback incidents that involved judgments were perceived as unhelpful and unfair, such as when participants felt slighted, abused, blamed, or rejected. Similarly, participants did not appreciate receiving feedback that they perceived as personal judgments, such as “you're obsessive-compulsive,”“you're narrow-minded,” and insults, such as “doctors ought to shut up.” Participants did not like receiving lectures or being given information that they regarded as redundant or gratuitous. Respondents also disliked receiving feedback in inappropriate places, such as a crowded elevator.
Quantitative Analyses
The semantic differential ratings of feedback techniques associated with helpful and unhelpful feedback incidents are presented in Figure 1 in the form of two profiles. We calculated the difference between the mean ratings for the bipolar descriptors. All the differences were significant (p < .001), as was the overall difference (Student's t= 10.21, p < .001, df= 101). The ratings of the 74 helpful incidents were clearly associated with the nine recommended feedback techniques (range of 3.8–4.8, on a 5-point scale where 5.0 represents closest association with the recommended technique). The following were the highest rated feedback techniques: the feedback giver based the feedback on observations (mean 4.8, CI ± 0.1), created a respectful, friendly teaching, climate (mean 4.6, CI ± 0.1), and was nonjudgmental in approach (mean 4.5, CI ± 0.1). These recommended feedback techniques thus are associated with feedback incidents perceived as helpful.
Figure 1.

Profile of behaviors associated with helpful and unhelpful feedback incidents (mean scores and confidence intervals).
The ratings of the 28 unhelpful incidents showed a weaker association with the nonrecommended feedback techniques (with a range of 1.7–3.8, where 1.0 represents closest association with the nonrecommended technique). Only six of the nine nonrecommended techniques (those with mean scores less than 3) were associated with the unhelpful incidents. These techniques included the following: did not elicit participants' ideas and feelings before giving the feedback (mean 1.7, CI ± 0.4); offered no suggestions for improvement (mean 2.2, CI ± 0.5), and was not goal-based (mean 2.3, CI ± 0.5), and was judgmental (mean 2.3, CI ± 0.5). These nonrecommended feedback techniques thus are associated with feedback incidents being perceived as unhelpful. Three recommended techniques were associated with the unhelpful feedback incidents: focused feedback on specifics, based it on observations, and focused on behaviors.
The Spearman rank correlation between the nine measures (mean scores for helpful and unhelpful incidents) was r= .77, p= .01. We suggest that the paired mean scores with the greatest difference are the most “telling” in terms of being effective feedback techniques. The pairs with the greatest difference were that feedback is nonjudgmental (vs judgmental); the right amount of information (vs too much or too little feedback); goal-based (vs not goal-based); elicitation of thoughts and feelings (vs no elicitation); and suggestions for improvement (vs no suggestions for improvement).
Comparison Between Qualitative and Quantitative Data
We compared our qualitative and quantitative findings and found a remarkable agreement between the ideas generated from the narratives and the ratings in the semantic differential. The qualitative analyses elaborated on the items in a useful way. The only difference was that the qualitative analyses suggested that giving feedback in inappropriate places such as crowded elevators was not appreciated and therefore unhelpful.
DISCUSSION
The qualitative narrative data and quantitative semantic differential data are congruent and substantiate the literature-based recommended techniques for giving effective feedback. All the recommended techniques do appear to be descriptive of feedback incidents perceived by the recipients as helpful. Many respondents mentioned helpful feedback incidents associated with corrective as well as reinforcing feedback that involved the recommended techniques. One respondent, however, described an unhelpful feedback incident involving unspecific praise, which substantiates the importance of giving specific feedback based on observations, even when praising someone.
Only five of the nonrecommended techniques were associated with unhelpful feedback incidents. Evidence was lacking for the association of three nonrecommended feedback techniques with unhelpful feedback incidents: focusing on generalities; basing feedback on hearsay; and focusing on personality. The reasons for this may have been contextual—the course participants were allocated to groups that did not know each other, and therefore had no previous experiences on which to make comments that were based on hearsay or on personalities.
The recommended and nonrecommended techniques were significantly positively correlated, which was surprising to us as we expected a negative correlation. From these results we suggest that when feedback is perceived as unhelpful, the reason may be that the feedback giver either used some nonrecommended techniques (problem of commission), or did not use other recommended techniques (problem of omission). In other words, the feedback techniques that feedback givers do use are as important as those that they neglect to use.
The limitations of our study concern the low number of unhelpful feedback incidents compared with helpful incidents. This may be due to a highly successful course, highly skillful facilitators, respondents' fatigue, or perhaps the order in which the questions were asked (we asked for a helpful feedback incident before asking for an unhelpful incident). This relatively low number makes our assessment of the concept of unhelpful feedback somewhat less robust, but does not invalidate our findings, especially for qualitative analyses. The validity (or trustworthiness) for this study is high because respondents were rating incidents generated from their own recent experiences in the course.
The respondents came from many different institutions (nationally and internationally), and represented numerous medical disciplines, which gave us confidence in the representativeness of the study. We suggest that the relationships between teachers and students, attending physicians and residents, preceptors and medical students, and physicians and patients are analogous, and that the results from a faculty development course on patient interview skills may be generalizable to other types of medical training. Similar to the way in which problems in patient-physician relationships are encountered when patients feel ignored or insulted by their physicians,10 when a teacher's attempt to give feedback “goes wrong,” the student may feel personally judged, or that his or her opinions, thoughts, and ideas have been ignored or overlooked. Further research is indicated with medical students and residents, and to determine the relative importance of the different descriptors.
Our findings are consistent with general principles of adult learning, which suggest that adult learners welcome feedback, especially when it is based on their performance and tailored to their goals.11 These findings are supported by research in constructivist learning and teaching,12 which suggests that teachers should: (1) create an appropriate learning climate and orient the students to the focus of the session; (2) elicit the student's knowledge, skills, or attitudes; (3) diagnose the problems and decide on the appropriate feedback topic for the proposed session; (4) intervene by helping the respondent to reflect on his or her knowledge, attitudes, and skills, and facilitate his or her improvement through teaching tailored to particular problems; (5) apply the points made to specific situations; and (6) review the session in order to check the student's understanding after the conversation. Following this model, we suggest that the principles in Table 2 can be applied to giving both reinforcing and corrective feedback.
Table 2.
Feedback Model

These findings have application for faculty development on the topic of giving feedback effectively in clinical medical education, especially because faculty find giving feedback so difficult. The findings are also important in programs for training residents how to teach. They may be relevant in teaching trainees how to handle feedback more effectively, and avoiding the trap of becoming defensive when valuable information is being shared with them.
In conclusion, giving feedback, whether reinforcing and corrective, is an essential component of clinical education. This study focused on clinician-teachers, a population that is in need of study, particularly because they are the people who give much of the feedback in medical training. The data substantiate the recommended techniques described in the literature, and suggest both the “do's and don'ts” of giving effective feedback. We believe the findings may be generalizable to other populations such as medical students and residents in clinical medical education settings. Our data suggest that avoidance of giving feedback, although understandable, is unwarranted. When done well, even corrective feedback is seen as helpful and highly appreciated.
Acknowledgments
The authors thank Judith Van Kirk, MS, in the Department of Medicine at the University of Wisconsin and Liesel Copeland, PhD, The Cleveland Clinic and Peter Hewson, DPhil, in the School of Curriculum and Instruction at the University of Wisconsin for help with data analysis, and Thomas Lang at The Cleveland Clinic for editorial assistance.
References
- 1.Ende J. Feedback in clinical medical education. JAMA. 1983;250(8):777–81. [PubMed] [Google Scholar]
- 2.Isaacson JH, Posk LK, Litaker DG, Halperin AK. Resident perceptions of the evaluation process. Society of General Internal Medicine. J Gen Intern Med. 1995;10(suppl):89. [Google Scholar]
- 3.Westberg J, Jason H. Collaborative Clinical Education: The Foundation of Effective Health Care. New York, NY: Springer Company; 1993. [Google Scholar]
- 4.Scholtes PR. The Team Handbook: How to Use Teams to Improve Quality. Madison, Wis: Joiner Associates; 1988. [Google Scholar]
- 5.Lipkin M, Kaplan C, Clark W, Novack DH. Teaching medical interviewing: the Lipkin model. In: Lipkin M, Putnam SM, Lazare A, editors. The Medical Interview: Clinical Care, Education and Research. New York, NY: Springer-Verlag; 1995. pp. 413–22. In ed. [Google Scholar]
- 6.Sandelowski M. Telling stories: narrative approaches in qualitative research. IMAGE: J Nurs Sch. 1991;23(3):161–6. doi: 10.1111/j.1547-5069.1991.tb00662.x. [DOI] [PubMed] [Google Scholar]
- 7.Crabtree BF, Miller WL. Doing Qualitative Research. Newbury Park, Calif: Sage Publications; 1992. [Google Scholar]
- 8.Osgood CE, Suci GJ, Tannenbaum PH. The Measurement of Meaning. Urbana. Ill: University of Illinois Press; 1957. [Google Scholar]
- 9.Albreck PL, Settle RB. The Survey Research Handbook. (2nd ed.) Chicago, Ill: Richard D Irwin, Inc; 1995. [Google Scholar]
- 10.Beckman H, Markakis K, Suchman A, Frankel R. The doctor-patient relationship and malpractice. Arch Intern Med. 1994;154:1365–70. [PubMed] [Google Scholar]
- 11.Knowles MS. San Francisco, Calif: Jossey-Bass Publishers; 1980. The Modern Practice of Adult Education. [Google Scholar]
- 12.Hewson MG. Clinical teaching in the ambulatory setting. J Gen Intern Med. 1992;7:76–82. doi: 10.1007/BF02599107. [DOI] [PubMed] [Google Scholar]